
Massachusetts Laborer Dies After Arm is Caught in Rock Crushing Machine Conveyor Belt
Case: 02-MA-001-01
Release Date: February 24, 2004
SUMMARY
On February 7, 2002, a 37-year-old male laborer (the victim) was fatally injured when he became caught between a conveyor belt and an idler pulley of a rock crushing machine. The victim’s job consisted of sweeping and shoveling the area around the rock-crushing machine. Approximately 20 minutes after the victim arrived at work he was found underneath the rock crushing machine with his arm caught between a conveyor belt and an idler pulley. The co-worker, with the use of a cutting torch, cut the idler pulley off of the machine freeing the victim. A call was placed for emergency assistance and personnel from the local police department arrived at the scene within minutes. The victim was rushed to a local hospital were he was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
- ensure that all exposed and accessible sections of conveyors on rock crushing machines are guarded
- perform a hazard analysis prior to equipment use to ensure it is safe for employees
- provide training for employees on the proper use and the hazards of equipment at the workplace
- develop, implement and enforce the basic elements of a lockout/tagout program
- ensure that workers who are part of a multilingual workforce comprehend safety training for their assigned tasks
In addition, rock crushing machine manufacturers should:
- ensure that all moving parts, including conveyors, are guarded
- consider installing pull cable emergency stops.
INTRODUCTION
On February 11, 2002, the Massachusetts FACE Program was notified by the Occupational Health and Safety Administration (OSHA) through the 24-hour Occupational Fatality Hotline, that on February 7, 2002, a 37-year-old male laborer was fatally injured when he was caught between a conveyor belt and idler pulley of a rock crushing machine. An investigation was immediately initiated. On March 14, 2002 the Massachusetts FACE Program Director and an investigator traveled to the incident location where the victim’s employer was interviewed. The Massachusetts FACE Program Director traveled back to the incident site on March 26, 2002 to complete the employer interview. The police report, death certificate, corporate information, OSHA information and photographs were reviewed during the course of the investigation.
The company, a general contractor for roadway construction projects, also recycled earth products, such as soil, concrete and stone, and had been in business for 75 years at the time of the incident. The company employed eight people: three equipment operators, three laborers, one sales person and one office worker. Two of the eight employees were assigned to the rock crushing operation. The company had been performing the rock crushing task for the past eight years in a different location with an older model machine. The current rock crushing location, where the incident took place, had been in use for the past year.
The victim was an immigrant whose primary language was Portuguese and could not speak or read English. The company hired him as a laborer one-week before the incident took place. The company did have a health and safety program and held daily morning meetings, which included discussion of safety topics. The employer stated that the victim’s training had been both on-the-job and reading relevant task-related sections of the company’s health and safety program. There was no union representation at the company. The victim’s prior employment had been as a landscaper.
INVESTIGATION
The company involved in the incident was a family owned business, with two brothers as the current owners. The incident location, which was purchased approximately one year prior to the incident, consisted mainly of the rock crushing (recycling) operation. Non-contaminated earth materials, such as soil, concrete and rock, were delivered to the site and crushed into a gravel based solid fill, which was then sold to construction companies. The earth materials that were crushed were generated from the other section of the company, road construction.
The rock crushing operation had been manned with two employees, a machine operator/co-owner and a laborer, the victim. The employer described the victim’s tasks as general grounds keeping that consisted of sweeping debris into piles and shoveling up the debris piles. The victim’s on-the-job training consisted of showing him where to sweep and place shoveled debris piles. The employer reported that the victim was warned about the rock crushing machine hazards and not to go near the machine. In addition, the employer stated that the victim was shown the machine’s affixed warning stickers and the hazard areas identified by the stickers.
The machine involved in the incident was a 2001, “portable rock crushing plant”(Figure 1). The company had recently traded in their older rock crushing machine for a model that could process a larger volume of material. The rock crushing machine involved in the incident was diesel powered and weighed approximately 122,500 pounds.
Once the earth materials were transported onsite, they were placed into piles and eventually loaded into the machine’s hopper by a front-end loader. The hopper opening measured 48 inches by 34 inches and could hold 17 cubic yards of material. The earth materials were automatically fed from the hopper into the crushing area, which was located directly below the hopper. The crushing area consisted of a large rotating paddle type wheel with a rotor diameter of 47 inches. The crushed earth materials were then screened and the smaller debris was sent by conveyor to a discharge pile and larger debris were sent back to the crushing area.
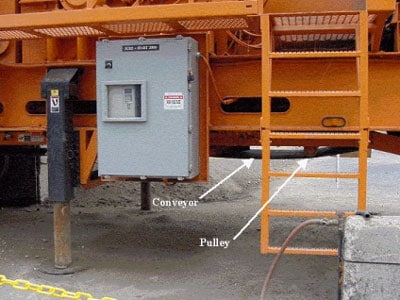
On the day of the incident, the rock crushing machine operator arrived on site before the victim and turned on the machine so it could warm up before use. The victim had arrived at the work site at 6:55 a.m. and at approximately 7:20 a.m., the machine operator found the victim caught by one of the rock crushing machine’s conveyor belts and an idler pulley. The location of the victim was underneath the machine near the electrical panel (Figure 2). The machine operator shut down the rock crushing machine and used an acetylene and oxygen torch to cut the idler pulley off of the machine, freeing the victim. Because the incident was not witnessed, it is unknown why the victim was close to the conveyor or how he became caught.
A call was placed for emergency medical assistance (EMS) and an ambulance responded to the scene within minutes and transported the victim to a hospital. Personnel from the local police department arrived on site a short time later and started an investigation. The victim was pronounced dead at the hospital.
At the time of the incident, the company did not have a lockout / tagout program. By the time of the FACE on site investigation, the company had developed and implemented a lockout / tagout program as requested by OSHA.
CAUSE OF DEATH
The medical examiner listed the cause of death as cardiopulmonary arrest due to shock due to crush.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that all exposed and accessible sections of conveyors on rock crushing machines are guarded.
Discussion: In this case, although the unguarded section of the rock crushing machine’s conveyor was located underneath the machine, it was still an accessible and exposed moving machine part and should had been guarded either with a point of operation guard or a barrier guard. It is the employers responsibility to ensure that machine operators and other employees who work in close proximity to machines are protected from all exposed and accessible moving machine parts. When considering altering a piece of equipment, such as adding a guard, the manufacturer of the equipment and an engineer should be consulted. Identifying hazards associated with operating machines can be accomplished by performing hazard analyses as discussed below. In addition, there are federal regulations1 that have been specifically written for machine guarding. The OSHA regulation states “One or more methods of machine guarding shall be provided to protect the operator and other employees in the machine area from hazards such as those created by point of operation, ingoing nip points, rotating parts, flying chips and sparks.”
Recommendation #2: Employers should perform a hazard analysis prior to equipment use to ensure it is safe for employees.
Discussion: A hazard analysis is a way of focusing on job tasks to identify hazards before injuries occur. Hazard analyses should be performed on all equipment, both new and old, to identify uncontrolled hazards. Once hazards are identified, the employer should take steps to eliminate or control these hazards.
Employers might assume that new equipment is “safe” as designed by the manufacturer. Although the rock crushing machine involved in the incident was less than one year old at the time of the incident, a section of the conveyor was unguarded. A hazard analysis of the machine by the employer prior to use might have revealed this hazard leading the employer to take steps to eliminate this hazard.
Recommendation #3: Employers should provide training for employees on the proper use and the hazards of equipment at the workplace.
Discussion: Equipment training should be provided to equipment operators and employees that will work in close proximity to the equipment. This training should include, but not be limited to, how to safely operate the equipment as outlined in the operator’s manual from the manufacturer and any other instructions or precautions that might be listed in the manual, such as the need to lockout/tagout a machine. Lockout/tagout program is discussed in recommendation #4. After the training is conducted, the employees’ knowledge should be tested by having them demonstrate their ability to operate or work around the equipment safely. The employer should keep documentation for each trained employee.
In this case, the victim had been employed with the company for approximately one week prior to the incident. While the victim was not assigned to operate the rock crushing machine, his job required him to work in close proximity to the machine and the company provided training that included warnings of hazards associated with the rock crushing machine. In addition, the training should have included basic machine operations and procedures to follow during an emergency.
Recommendation #4: Employers should develop, implement and enforce the basic elements of a lockout/tagout program.
Discussion: A lockout/tagout program should be developed by employers that addresses machines’ hazardous energy sources, along with the methods and means to isolate them. The lockout/tagout program should also address when lockout/tagout is necessary, and who is required to perform it, including machine operators and maintenance personnel as well as laborers working in close proximity to the machine. An enforced lockout/tagout program and employee training based on this program will help assure that workers are not exposed to moving machine parts.
Control of hazardous energy (lockout/tagout) is required by OSHA (29 CFR 1910.147)2 when any of the following conditions occur:
- The employee must either remove or bypass machine guards or other safety devices, resulting in exposure to hazards at the point of operation;
- The employee is required to place any part of his or her body in contact with the point of operation of the operational machine or piece of equipment; or
- The employee is required to place any part of his or her body into a danger zone associated with a machine operating cycle.
At the time of the incident, the company did not have a lockout/tagout program. One month later, when the FACE program was at the incident location, the company had a lockout/tagout program in place as requested by OSHA.
Recommendation #5: Employers should ensure that workers who are part of a multilingual workforce comprehend safety training for their assigned tasks.
Discussion: Overcoming language and literacy barriers is crucial to providing a safe work environment for a multilingual workforce. Companies should develop and provide training for workers in a language and at a literacy level workers are able to comprehend. This also applies to any training documents that require a worker’s signature. Interpreters should be available to explain to workers any work environment and task completion changes3 that were made since the training materials were produced.
In this case, the company provided training that included warnings of hazards associated with the rock crushing machine, but the victim might not have fully understood the hazards because his primary language was not English, the language in which the training was provided.
Recommendation #6: Manufacturers of rock crushing machines should ensure that all moving parts, including conveyors, are guarded.
Discussion: Although the manufacturer had designed many built-in guards on the rock crushing machine the section of conveyor involved in the incident, located partially underneath the machine, had not been guarded. The manufacturer should consider designing a point of operation guard for the section of the conveyor where the victim was caught. In addition, the manufacturer should develop a retrofit guard for all older rock crushing machines that pose this same hazard.
During the second site visit, the company involved in the incident reported that they had been in contact with the machine manufacturer about the possibility of adding a guard to the section of the conveyor that was unguarded.
Recommendation #7: Manufacturers of rock crushing machines should consider installing pull cable emergency stops.
Discussion: Emergency stops are a safety feature that overrides all other controls located on the machine. In this case, an emergency stop could be in the form of a pull cable that surrounds the entire machine’s perimeter4 rather than multiple spaced out push buttons. The emergency stop would be activated immediately, when the cable is pulled, shutting down the machine. This type of emergency stop is typically used for conveyors in warehouses.
REFERENCES
- Code of Federal Regulations, 29 CFR 1910.212 Machinery and Machine Guarding, General requirements for all machines, Government Printing Office.
- Code of Federal Regulations, 29 CFR 1910.147 General Environmental Controls, The control of hazardous energy (lockout/tagout), Government Printing Office.
- NIOSH FACE Report Number 2003-06, Hispanic Carpenter Dies After Being Crushed Between the Loader Bucket of a Backhoe/Loader and a Concrete Building – North Carolina.
- Honeywell, Sensing and Control, Safety Cable Pull Switch for Emergency Stop, http://honeywell.com/Pages/Home.aspx (Link updated 3/27/2013)
ILLUSTRATIONS
 |
|
Figure 1 – Rock Crushing Machine
|
 |
|
Figure 2 – Conveyor and Idler Pulley
|
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.