
Cement Finisher Dies After 17-Foot Fall Through Unguarded Floor Opening-North Carolina
FACE 9321
SUMMARY
A 38-year-old male cement finisher (the victim) died of injuries he received after stepping backwards and falling through an unguarded floor opening. The victim was one of 13 subcontractor employees pouring cement for a three-story addition to a textile mill. At the time of the incident, one half of the floor of the second story was being poured. The entire floor measured 84 feet wide by 119 feet long and contained eight unguarded openings, each measuring 32 inches wide by 18 feet long. These openings were to be used as vents and ducts for service cables. The floor also contained a 13-foot by 9-foot, 8-inch opening for an elevator shaft; the opening was guarded by a steel rope barrier. The victim and a co-worker (facing away from each other) were working approximately 10 feet apart, finishing the poured concrete with aluminum bull floats. The victim, who was walking backwards as he worked the bull float, stepped into one of the unguarded floor openings. He fell 17 feet to the concrete floor below, striking his head. The co-worker did not see the victim fall, but heard him yell; however, the apprentice superintendent for the prime contractor was on the second story and saw the victim fall through the opening. Textile mill workers on the first floor also saw the victim fall, and ran to his aid. The victim was unconscious but breathing. The emergency medical service (EMS) was summoned and transported the victim to the hospital where he died 12 days later. NIOSH investigators concluded that, to prevent similar occurrences, employers should:
- implement 29 CFR 1926.500 (b)(1) and (8), which requires that all floor and platform openings be protected with a standard railing or a floor opening cover secured against displacement
- address worker safety issues in the planning phase of construction projects
- develop and implement a comprehensive written safety program.
Additionally, prime contractors should:
- utilize contract language that requires subcontractors to implement a site-specific safety and health program prior to the initiation of work.
INTRODUCTION
On July 2, 1993, a 38-year-old male cement finisher (the victim) died of injuries he received on June 21, 1993, when he stepped backwards into an unguarded floor opening and fell 17 feet to the concrete floor below. On July 6, 1993, officials of the North Carolina Occupational Safety and Health Administration (NCOSHA) notified the Division of Safety Research (DSR) of this fatality, and requested technical assistance. On August 10, 1993, a safety specialist from DSR investigated the incident and reviewed the circumstances with employer representatives and officials of NCOSHA.
The employer in this incident was a temporary employment service which supplied 22 employees to a concrete contractor. At the time of the incident, the concrete contractor was the only client of the temporary service, and both establishments were operated by the same owners. Neither establishment had a written safety program, and training was provided on the job. Tailgate safety meetings were conducted periodically by the crew supervisor, who was also responsible for worker safety at the jobsite. The victim had worked for the temporary service for 7 years. The service had been in operation for approximately 25 years and had experienced no previous fatalities.
INVESTIGATION
The employer had been subcontracted to do the concrete work for an addition to the spinning area of a textile mill that produced fortrel polyester fiber. The addition was three stories high and measured 84 feet by 119 feet. The employer had a 13-man crew at the site performing various tasks, such as forming areas prior to pouring concrete, laying steel decking on which the concrete would be poured, and working the cement with bull floats.
On the day of the incident, the job was approximately 80 percent complete and work had progressed to the floor of the second story. The forming of the floor had been completed. One half of the floor was to be poured on the day of the incident and the rest of the concrete was to be poured the following day.
Eight unguarded floor openings, each measuring 32 inches wide by 18 feet long, had been formed into the floor. These openings would be used as vents and ducts for service cables. A ninth floor opening measuring 13 feet long by 9 feet 8 inches wide, marked the location of the elevator shaft and was guarded by a steel rope barrier (Figure).
The crew supervisor approached the apprentice superintendent for the prime contractor 1 week before the pour was to take place and requested that the floor openings be covered. When the openings were not yet covered on the day of the pour, the crew supervisor again approached the apprentice superintendent. The men discussed the issue and decided that each would tell their respective workers to be extremely careful around the openings. Witnesses stated during NCOSHA interviews that some of the openings were covered by wooden pallets that measured 40 inches by 48 inches. The pallets were obtained from a second subcontractor doing concrete block work on the addition; however, at the time of the incident, the second subcontractor had removed some of the pallets from the floor openings to return them for a pre-paid deposit. It could not be determined whether or not the floor opening involved in the incident had previously been covered by the pallets, or if any of the floor openings were covered at the time of the incident.
At approximately 11 a.m., the victim and another cement finisher were on the second story floor guiding the pump truck, which was pouring and working down the concrete. When the surface of a section of the poured concrete was relatively smooth and level, workers would further smooth the surface, using aluminum bull floats. The two men were working approximately 10 feet apart, but were not facing each other. The apprentice superintendent was on the second story in the vicinity of the elevator shaft opening.
As the victim was walking backward floating the concrete, he stepped into the unguarded opening and fell approximately 17 feet to the concrete floor below, striking his head. The co-worker did not see the victim fall, but heard him yell. The apprentice superintendent saw a portion of the victim’s body fall through the opening.
Textile mill workers on the first floor also saw the victim fall and ran to aid him. The victim was unconscious but breathing. The EMS was summoned; it arrived within 15 minutes and transported the victim to the hospital, where he remained in a coma until his death 12 days later on July 2, 1993.
CAUSE OF DEATH
The coroner listed the cause of death as closed head trauma-skull fracture.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should implement 29 CFR 1926.500 (b)(1) and (8), which requires that all floor and platform openings be protected with a standard railing or a floor opening cover secured against displacement.
Discussion: Prior to the start of work, floor openings should be protected with a standard railing, or covered or guarded with materials that are installed so as to prevent displacement. After the incident, the openings were properly fitted with secured plywood covers by the prime contractor.
Recommendation #2: Employers should address worker safety in the planning phase of construction projects.
Discussion: Safety concerns should be addressed and incorporated into all construction projects during the planning phase and throughout the entire project. Such a procedure would allow for the identification of potential hazards prior to the initiation of work so that appropriate intervention strategies could be implemented.
Recommendation #3: Employers should develop and implement a comprehensive written safety program.
Discussion: Employers should develop and implement a comprehensive written safety program which includes, but is not limited to, the proper use of fall protection equipment, the recognition and control of fall hazards, and should include appropriate worker training in the proper methods of covering/guarding floor openings to prevent falls through the openings. Development, implementation, and enforcement of a written safety program and the establishment of standard safety practices will demonstrate to workers the employer’s commitment to safety.
Recommendation #4: Prime contractors should utilize contract language that requires subcontractors to implement a site-specific safety and health program prior to the initiation of work.
Discussion: Prime contractors should use contract language that requires all subcontractors to identify how they intend to implement a site-specific safety and health program prior to the initiation of work. Subcontractors’ safety programs should be consistent and compatible with the prime contractor’s safety program. The contract should contain clear and concise language as to which party is responsible for a given safety or health issue. Any differences should be negotiated before work begins.
Once the provisions for these responsibilities have been established, the respective parties should ensure that the provisions of the contract regarding safety and health are upheld.
REFERENCES
Office of the Federal Register: Code of Federal Regulations, Labor 29 Part 1926.500 (b)(1) and (8), July 1, 1992.
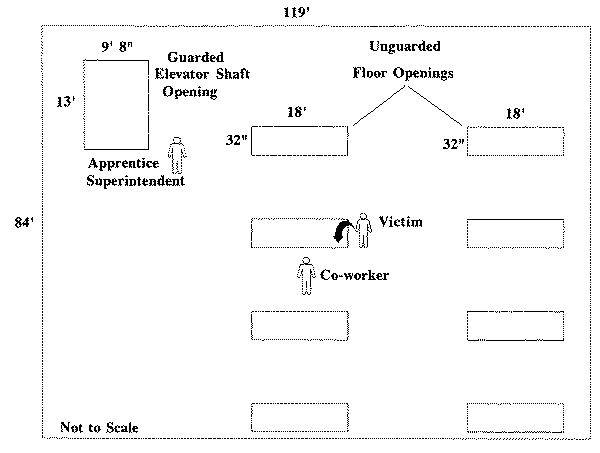
Figure.