Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Settings, 2005
Please note:This report has been corrected and replaces the electronic PDF version that was published on December 30, 2005.
Prepared by
Paul A. Jensen, PhD, Lauren A. Lambert, MPH, Michael F. Iademarco, MD, Renee Ridzon, MD
Division of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention
The material in this report originated in the National Center for HIV, STD, and TB Prevention, Kevin Fenton, MD, PhD, Director; and the Division of Tuberculosis Elimination, Kenneth G. Castro, MD, Director.
Corresponding preparer: Paul A. Jensen, PhD, Division of Tuberculosis Elimination, National Center for HIV, STD, and TB Prevention, 1600 Clifton Rd., NE, MS E-10, Atlanta, GA 30333. Telephone: 404-639-8310; Fax: 404-639-8604; E-mail: pej4@cdc.gov.
Summary
In 1994, CDC published the Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Facilities, 1994. The guidelines were issued in response to 1) a resurgence of tuberculosis (TB) disease that occurred in the United States in the mid-1980s and early 1990s, 2) the documentation of several high-profile health-care–associated (previously termed "nosocomial") outbreaks related to an increase in the prevalence of TB disease and human immunodeficiency virus (HIV) coinfection, 3) lapses in infection-control practices, 4) delays in the diagnosis and treatment of persons with infectious TB disease, and 5) the appearance and transmission of multidrug-resistant (MDR) TB strains. The 1994 guidelines, which followed statements issued in 1982 and 1990, presented recommendations for TB-infection control based on a risk assessment process that classified health-care facilities according to categories of TB risk, with a corresponding series of administrative, environmental, and respiratory-protection control measures.
The TB infection-control measures recommended by CDC in 1994 were implemented widely in health-care facilities in the United States. The result has been a decrease in the number of TB outbreaks in health-care settings reported to CDC and a reduction in health-care–associated transmission of Mycobacterium tuberculosis to patients and health-care workers (HCWs). Concurrent with this success, mobilization of the nation's TB-control programs succeeded in reversing the upsurge in reported cases of TB disease, and case rates have declined in the subsequent 10 years. Findings indicate that although the 2004 TB rate was the lowest recorded in the United States since national reporting began in 1953, the declines in rates for 2003 (2.3%) and 2004 (3.2%) were the smallest since 1993. In addition, TB infection rates greater than the U.S. average continue to be reported in certain racial/ethnic populations. The threat of MDR TB is decreasing, and the transmission of M. tuberculosis in health-care settings continues to decrease because of implementation of infection-control measures and reductions in community rates of TB.
Given the changes in epidemiology and a request by the Advisory Council for the Elimination of Tuberculosis (ACET) for review and update of the 1994 TB infection-control document, CDC has reassessed the TB infection-control guidelines for health-care settings. This report updates TB control recommendations reflecting shifts in the epidemiology of TB, advances in scientific understanding, and changes in health-care practice that have occurred in the United States during the preceding decade. In the context of diminished risk for health-care–associated transmission of M. tuberculosis, this document places emphasis on actions to maintain momentum and expertise needed to avert another TB resurgence and to eliminate the lingering threat to HCWs, which is mainly from patients or others with unsuspected and undiagnosed infectious TB disease. CDC prepared the current guidelines in consultation with experts in TB, infection control, environmental control, respiratory protection, and occupational health. The new guidelines have been expanded to address a broader concept; health-care–associated settings go beyond the previously defined facilities. The term "health-care setting" includes many types, such as inpatient settings, outpatient settings, TB clinics, settings in correctional facilities in which health care is delivered, settings in which home-based health-care and emergency medical services are provided, and laboratories handling clinical specimens that might contain M. tuberculosis. The term "setting" has been chosen over the term "facility," used in the previous guidelines, to broaden the potential places for which these guidelines apply.
Introduction
Overview
In 1994, CDC published the Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health Care Facilities, 1994 (1). The guidelines were issued in response to 1) a resurgence of tuberculosis (TB) disease that occurred in the United States in the mid-1980s and early 1990s, 2) the documentation of multiple high-profile health-care–associated (previously "nosocomial") outbreaks related to an increase in the prevalence of TB disease and human immunodeficiency virus (HIV) coinfection, 3) lapses in infection-control practices, 4) delays in the diagnosis and treatment of persons with infectious TB disease (2,3), and 5) the appearance and transmission of multidrug-resistant (MDR) TB strains (4,5).
The 1994 guidelines, which followed CDC statements issued in 1982 and 1990 (1,6,7), presented recommendations for TB infection control based on a risk assessment process. In this process, health-care facilities were classified according to categories of TB risk,with a corresponding series of environmental and respiratory-protection control measures.
The TB infection-control measures recommended by CDC in 1994 were implemented widely in health-care facilities nationwide (8–15). As a result, a decrease has occurred in 1) the number of TB outbreaks in health-care settings reported to CDC and 2) health-care–associated transmission of M. tuberculosis to patients and health-care workers (HCWs) (9,16–23). Concurrent with this success, mobilization of the nation's TB-control programs succeeded in reversing the upsurge in reported cases of TB disease, and case rates have declined in the subsequent 10 years (4,5). Findings indicate that although the 2004 TB rate was the lowest recorded in the United States since national reporting began in 1953, the declines in rates for 2003 (2.3%) and 2004 (3.2%) were the lowest since 1993. In addition, TB rates higher than the U.S. average continue to be reported in certain racial/ethnic populations (24). The threat of MDR TB is decreasing, and the transmission of M. tuberculosis in health-care settings continues to decrease because of implementation of infection-control measures and reductions in community rates of TB (4,5,25).
Despite the general decline in TB rates in recent years, a marked geographic variation in TB case rates persists, which means that HCWs in different areas face different risks (10). In 2004, case rates varied per 100,000 population: 1.0 in Wyoming, 7.1 in New York, 8.3 in California, and 14.6 in the District of Columbia (26). In addition, despite the progress in the United States, the 2004 rate of 4.9 per 100,000 population remained higher than the 2000 goal of 3.5. This goal was established as part of the national strategic plan for TB elimination; the final goal is <1 case per 1,000,000 population by 2010 (4,5,26).
Given the changes in epidemiology and a request by the Advisory Council for the Elimination of Tuberculosis (ACET) for review and updating of the 1994 TB infection-control document, CDC has reassessed the TB infection-control guidelines for health-care settings. This report updates TB-control recommendations, reflecting shifts in the epidemiology of TB (27), advances in scientific understanding, and changes in health-care practice that have occurred in the United States in the previous decade (28). In the context of diminished risk for health-care–associated transmission of M. tuberculosis, this report emphasizes actions to maintain momentum and expertise needed to avert another TB resurgence and eliminate the lingering threat to HCWs, which is primarily from patients or other persons with unsuspected and undiagnosed infectious TB disease.
CDC prepared the guidelines in this report in consultation with experts in TB, infection control, environmental control, respiratory protection, and occupational health. This report replaces all previous CDC guidelines for TB infection control in health-care settings (1,6,7). Primary references citing evidence-based science are used in this report to support explanatory material and recommendations. Review articles, which include primary references, are used for editorial style and brevity.
The following changes differentiate this report from previous guidelines:
The risk assessment process includes the assessment of additional aspects of infection control.
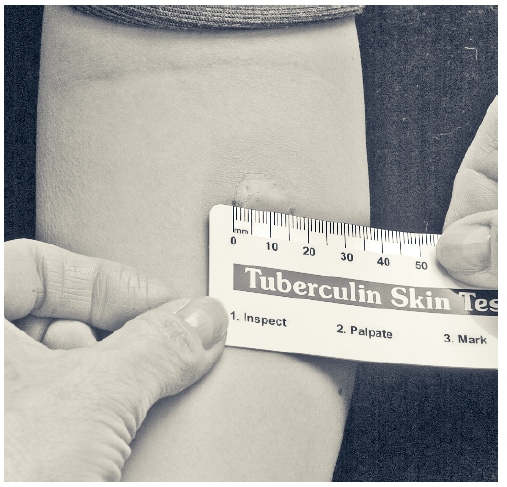
The term "tuberculin skin tests" (TSTs) is used instead of purified protein derivative (PPD).
The whole-blood interferon gamma release assay (IGRA), QuantiFERON(r)-TB Gold test (QFT-G) (Cellestis Limited, Carnegie, Victoria, Australia), is a Food and Drug Administration (FDA)–approved in vitro cytokine-based assay for cell-mediated immune reactivity to M. tuberculosis and might be used instead of TST in TB screening programs for HCWs. This IGRA is an example of a blood assay for M. tuberculosis (BAMT).
The frequency of TB screening for HCWs has been decreased in various settings, and the criteria for determination of screening frequency have been changed.
The scope of settings in which the guidelines apply has been broadened to include laboratories and additional outpatient and nontraditional facility-based settings.
Criteria for serial testing for M. tuberculosis infection of HCWs are more clearly defined. In certain settings, this change will decrease the number of HCWs who need serial TB screening.
These recommendations usually apply to an entire health-care setting rather than areas within a setting.
New terms, airborne infection precautions (airborne precautions) and airborne infection isolation room (AII room), are introduced.
Recommendations for annual respirator training, initial respirator fit testing, and periodic respirator fit testing have been added.
The evidence of the need for respirator fit testing is summarized.
Information on ultraviolet germicidal irradiation (UVGI) and room-air recirculation units has been expanded.
Additional information regarding MDR TB and HIV infection has been included.
In accordance with relevant local, state, and federal laws, implementation of all recommendations must safeguard the confidentiality and civil rights of all HCWs and patients who have been infected with M. tuberculosis and who developTB disease.
The 1994 CDC guidelines were aimed primarily at hospital-based facilities, which frequently refer to a physical building or set of buildings. The 2005 guidelines have been expanded to address a broader concept. Setting has been chosen instead of "facility" to expand the scope of potential places for which these guidelines apply (Appendix A). "Setting" is used to describe any relationship (physical or organizational) in which HCWs might share air space with persons with TB disease or in which HCWs might be in contact with clinical specimens. Various setting types might be present in a single facility. Health-care settings include inpatient settings, outpatient settings, and nontraditional facility-based settings.
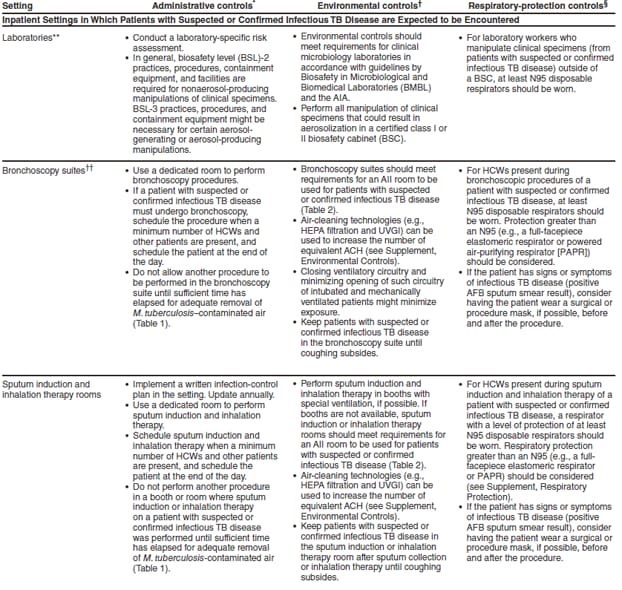
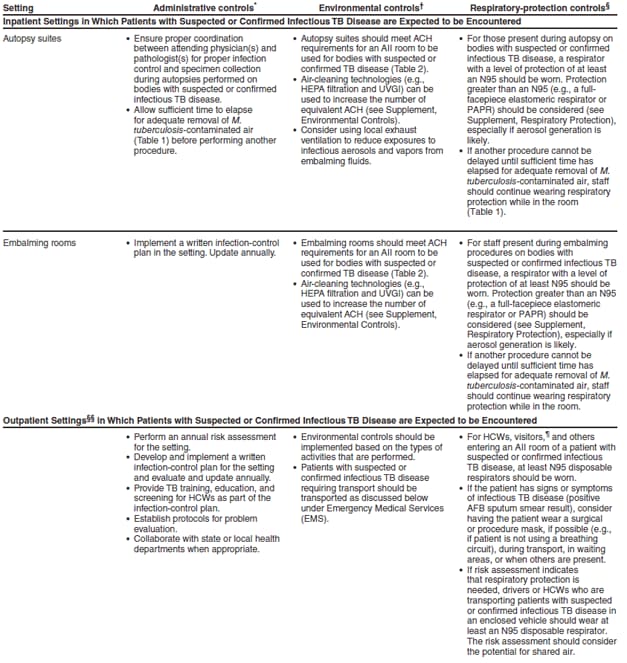
Inpatient settings include patient rooms, emergency departments (EDs), intensive care units (ICUs), surgical suites, laboratories, laboratory procedure areas, bronchoscopy suites, sputum induction or inhalation therapy rooms, autopsy suites, and embalming rooms.
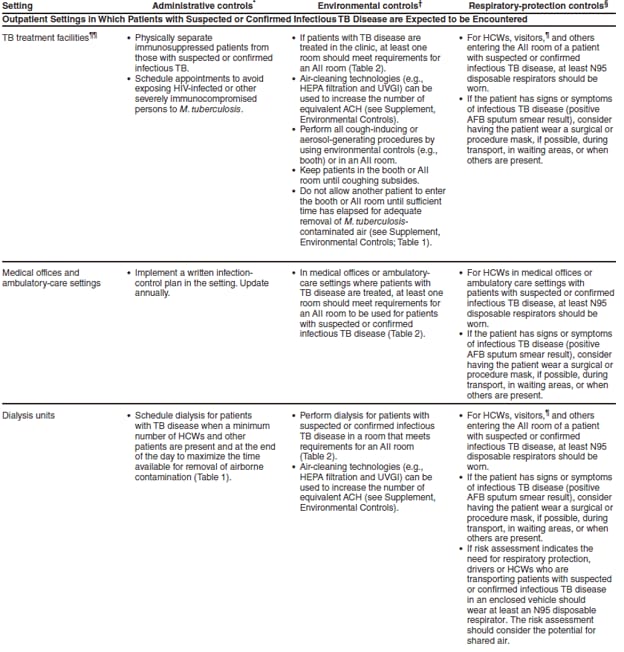
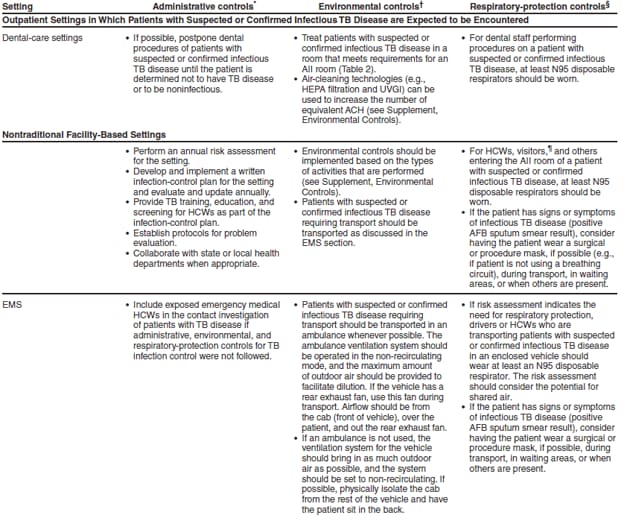
Outpatient settings include TB treatment facilities, medical offices, ambulatory-care settings, dialysis units, and dental-care settings.
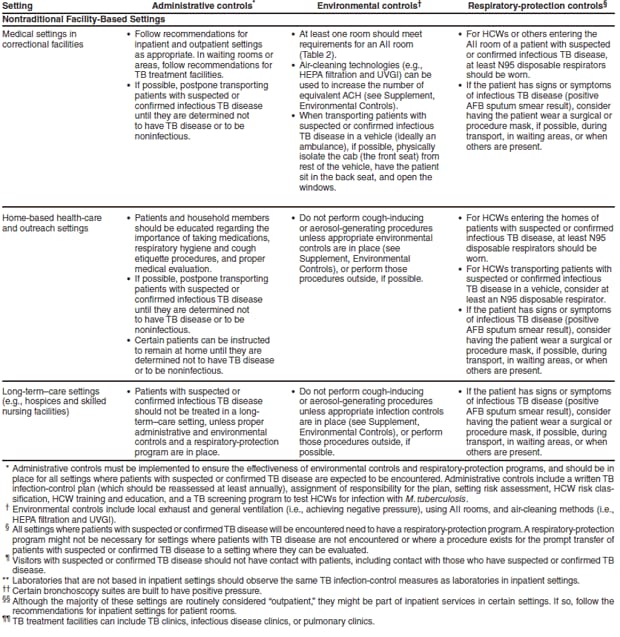
Nontraditional facility-based settings include emergency medical service (EMS), medical settings in correctional facilities (e.g., prisons, jails, and detention centers), home-based health-care and outreach settings, long-term–care settings (e.g., hospices, skilled nursing facilities), and homeless shelters. Other settings in which suspected and confirmed TB patients might be encountered might include cafeterias, general stores, kitchens, laundry areas, maintenance shops, pharmacies, and law enforcement settings.
HCWs Who Should Be Included in a TB Surveillance Program
HCWs refer to all paid and unpaid persons working in health-care settings who have the potential for exposure to M. tuberculosis through air space shared with persons with infectious TB disease. Part time, temporary, contract, and full-time HCWs should be included in TB screening programs. All HCWs who have duties that involve face-to-face contact with patients with suspected or confirmed TB disease (including transport staff) should be included in a TB screening program.
The following are HCWs who might be included in a TB screening program:
Administrators or managers
Bronchoscopy staff
Chaplains
Clerical staff
Computer programmers
Construction staff
Correctional officers
Craft or repair staff
Dental staff
Dietician or dietary staff
ED staff
Engineers
Food service staff
Health aides
Health and safety staff
Housekeeping or custodial staff
Homeless shelter staff
Infection-control staff
ICU staff
Janitorial staff
Laboratory staff
Maintenance staff
Morgue staff
Nurses
Outreach staff
Pathology laboratory staff
Patient transport staff, including EMS
Pediatric staff
Pharmacists
Phlebotomists
Physical and occupational therapists
Physicians (assistant, attending, fellow, resident, or intern), including
— anesthesiologists
— pathologists
— psychiatrists
— psychologists
Public health educators or teachers
Public safety staff
Radiology staff
Respiratory therapists
Scientists
Social workers
Students (e.g., medical, nursing, technicians, and allied health)
Technicians (e.g., health, laboratory, radiology, and animal)
Veterinarians
Volunteers
In addition, HCWs who perform any of the following activities should also be included in the TB screening program.
entering patient rooms or treatment rooms whether or not a patient is present;
participating in aerosol-generating or aerosol-producing procedures (e.g., bronchoscopy, sputum induction, and administration of aerosolized medications) (29);
participating in suspected or confirmed M. tuberculosis specimen processing; or
installing, maintaining, or replacing environmental controls in areas in which persons with TB disease are encountered.
Pathogenesis, Epidemiology, and Transmission of M. tuberculosis
M. tuberculosis is carried in airborne particles called droplet nuclei that can be generated when persons who have pulmonary or laryngeal TB disease cough, sneeze, shout, or sing (30,31). The particles are approximately 1–5 µm; normal air currents can keep them airborne for prolonged periods and spread them throughout a room or building (32). M. tuberculosis is usually transmitted only through air, not by surface contact. After the droplet nuclei are in the alveoli, local infection might be established, followed by dissemination to draining lymphatics and hematogenous spread throughout the body (33). Infection occurs when a susceptible person inhales droplet nuclei containing M. tuberculosis, and the droplet nuclei traverse the mouth or nasal passages, upper respiratory tract, and bronchi to reach the alveoli. Persons with TB pleural effusions might also have concurrent unsuspected pulmonary or laryngeal TB disease.
Usually within 2–12 weeks after initial infection with M. tuberculosis, the immune response limits additional multiplication of the tubercle bacilli, and immunologic test results for M. tuberculosis infection become positive. However, certain bacilli remain in the body and are viable for multiple years. This condition is referred to as latent tuberculosis infection (LTBI). Persons with LTBI are asymptomatic (they have no symptoms of TB disease) and are not infectious.
In the United States, LTBI has been diagnosed traditionally based on a PPD-based TST result after TB disease has been excluded. In vitro cytokine-based immunoassays for the detection of M. tuberculosis infection have been the focus of intense research and development. One such blood assay for M. tuberculosis (or BAMT) is an IGRA, the QuantiFERON(r)-TB test (QFT), and the subsequently developed version, QFT-G. The QFT-G measures cell-mediated immune responses to peptides from two M. tuberculosis proteins that are not present in any Bacille Calmette-Guérin (BCG) vaccine strain and that are absent from the majority of nontuberculous mycobacteria (NTM), also known as mycobacteria other than TB (MOTT). QFT-G was approved by FDA in 2005 and is an available option for detecting M. tuberculosis infection. CDC recommendations for the United States regarding QFT and QFT-G have been published (34,35). Because this field is rapidly evolving, in this report, BAMT will be used generically to refer to the test currently available in the United States.
Additional cytokine-based immunoassays are under development and might be useful in the diagnosis of M. tuberculosis infection. Future FDA-licensed products in combination with CDC-issued recommendations might provide additional diagnostic alternatives. The latest CDC recommendations for guidance on diagnostic use of these and related technologies are available at http://www.cdc.gov/nchstp/tb/pubs/mmwr/html/Maj_guide/Diagnosis.htm.
Typically, approximately 5%–10% of persons who become infected with M. tuberculosis and who are not treated for LTBI will develop TB disease during their lifetimes (1). The risk for progression of LTBI to TB disease is highest during the first several years after infection (36–38).
Persons at Highest Risk for Exposure to and Infection with M. tuberculosis
Characteristics of persons exposed to M. tuberculosis that might affect the risk for infection are not as well defined. The probability that a person who is exposed to M. tuberculosis will become infected depends primarily on the concentration of infectious droplet nuclei in the air and the duration of exposure to a person with infectious TB disease. The closer the proximity and the longer the duration of exposure, the higher the risk is for being infected.
Close contacts are persons who share the same air space in a household or other enclosed environment for a prolonged period (days or weeks, not minutes or hours) with a person with pulmonary TB disease (39). A suspect TB patient is a person in whom a diagnosis of TB disease is being considered, whether or not antituberculosis treatment has been started. Persons generally should not remain a suspect TB patient for >3 months (30,39).
In addition to close contacts, the following persons are also at higher risk for exposure to and infection with M. tuberculosis. Persons listed who are also close contacts should be top priority.
Foreign-born persons, including children, especially those who have arrived to the United States within 5 years after moving from geographic areas with a high incidence of TB disease (e.g., Africa, Asia, Eastern Europe, Latin America, and Russia) or who frequently travel to countries with a high prevalence of TB disease.
Residents and employees of congregate settings that are high risk (e.g., correctional facilities, long-term–care facilities [LTCFs], and homeless shelters).
HCWs who serve patients who are at high risk.
HCWs with unprotected exposure to a patient with TB disease before the identification and correct airborne precautions of the patient.
Certain populations who are medically underserved and who have low income, as defined locally.
Populations at high risk who are defined locally as having an increased incidence of TB disease.
Infants, children, and adolescents exposed to adults in high-risk categories.
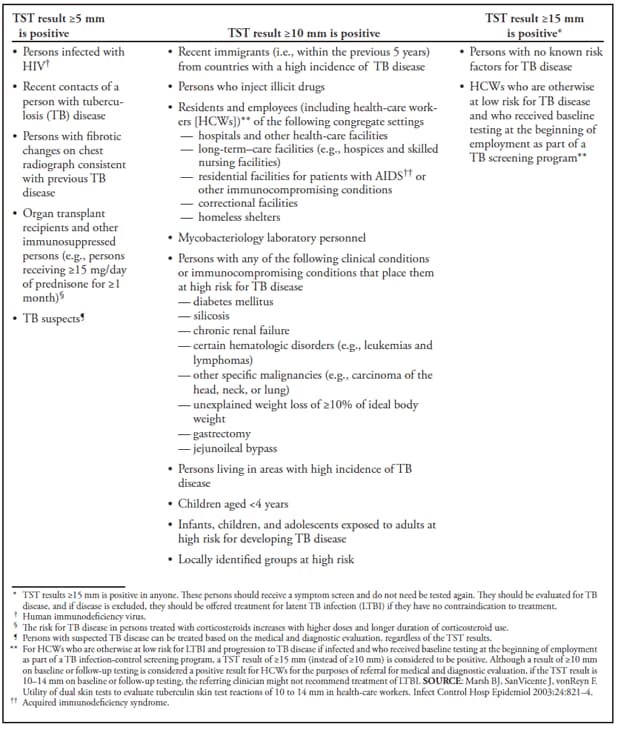
Persons Whose Condition is at High Risk for Progression From LTBI to TB Disease
The following persons are at high risk for progressing from LTBI to TB disease:
persons infected with HIV;
persons infected with M. tuberculosis within the previous 2 years;
infants and children aged <4 years;
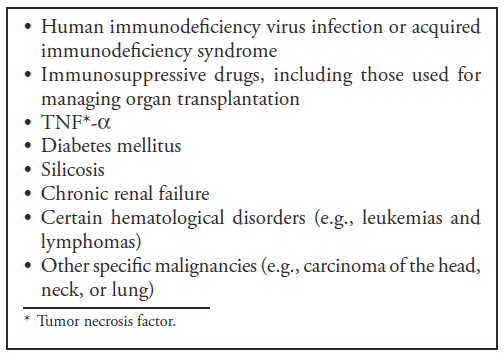
persons with any of the following clinical conditions or other immunocompromising conditions
— silicosis,
— diabetes mellitus,
— chronic renal failure,
— certain hematologic disorders (leukemias and lymphomas),
— other specific malignancies (e.g., carcinoma of the head, neck, or lung),
— body weight ≥10% below ideal body weight,
— prolonged corticosteroid use,
— other immunosuppressive treatments (including tumor necrosis factor-alpha [TNF-α] antagonists),
— organ transplant,
— end-stage renal disease (ESRD), and
— intestinal bypass or gastrectomy; and
persons with a history of untreated or inadequately treated TB disease, including persons with chest radiograph findings consistent with previous TB disease.
Persons who use tobacco or alcohol (40,41), illegal drugs, including injection drugs and crack cocaine (42–47), might also be at increased risk for infection and disease. However, because of multiple other potential risk factors that commonly occur among such persons, use of these substances has been difficult to identify as separate risk factors.
HIV infection is the greatest risk factor for progression from LTBI to TB disease (22,39,48,49). Therefore, voluntary HIV counseling, testing, and referral should be routinely offered to all persons at risk for LTBI (1,50,51). Health-care settings should be particularly aware of the need for preventing transmission of M. tuberculosis in settings in which persons infected with HIV might be encountered or might work (52).
All HCWs should be informed regarding the risk for developing TB disease after being infected with M. tuberculosis (1). However, the rate of TB disease among persons who are HIV-infected and untreated for LTBI in the United States is substantially higher, ranging from 1.7–7.9 TB cases per 100 person-years (53). Persons infected with HIV who are already severely immunocompromised and who become newly infected with M. tuberculosis have a greater risk for developing TB disease, compared with newly infected persons without HIV infection (39,53–57).
The percentage of patients with TB disease who are HIV-infected is decreasing in the United States because of improved infection-control practices and better diagnosis and treatment of both HIV infection and TB. With increased voluntary HIV counseling and testing and the increasing use of treatment for LTBI, TB disease will probably continue to decrease among HIV-infected persons in the United States (58). Because the risk for disease is particularly high among HIV-infected persons with M. tuberculosis infection, HIV-infected contacts of persons with infectious pulmonary or laryngeal TB disease must be evaluated for M. tuberculosis infection, including the exclusion of TB disease, as soon as possible after learning of exposure (39,49,53).
Vaccination with BCG probably does not affect the risk for infection after exposure, but it might decrease the risk for progression from infection with M. tuberculosis to TB disease, preventing the development of miliary and meningeal disease in infants and young children (59,60). Although HIV infection increases the likelihood of progression from LTBI to TB disease (39,49), whether HIV infection increases the risk for becoming infected if exposed to M. tuberculosis is not known.
Characteristics of a Patient with TB Disease That Increase the Risk for Infectiousness
The following characteristics exist in a patient with TB disease that increases the risk for infectiousness:
respiratory tract disease with involvement of the larynx (substantially infectious);
respiratory tract disease with involvement of the lung or pleura (exclusively pleural involvement is less infectious);
failure to cover the mouth and nose when coughing;
incorrect, lack of, or short duration of antituberculosis treatment; and
undergoing cough-inducing or aerosol-generating procedures (e.g., bronchoscopy, sputum induction, and administration of aerosolized medications) (29).
Environmental Factors That Increase the Risk for Probability of Transmission of M. tuberculosis
The probability of the risk for transmission of M. tuberculosis is increased as a result of various environmental factors.
Exposure to TB in small, enclosed spaces.
Inadequate local or general ventilation that results in insufficient dilution or removal of infectious droplet nuclei.
Recirculation of air containing infectious droplet nuclei.
Inadequate cleaning and disinfection of medical equipment.
Improper procedures for handling specimens.
Risk for Health-Care–Associated Transmission of M. tuberculosis
Transmission of M. tuberculosis is a risk in health-care settings (57,61–79). The magnitude of the risk varies by setting, occupational group, prevalence of TB in the community, patient population, and effectiveness of TB infection-control measures. Health-care–associated transmission of M. tuberculosis has been linked to close contact with persons with TB disease during aerosol-generating or aerosol-producing procedures, including bronchoscopy (29,63,80–82), endotracheal intubation, suctioning (66), other respiratory procedures (8,9,83–86), open abscess irrigation (69,83), autopsy (71,72,77), sputum induction, and aerosol treatments that induce coughing (87–90).
Of the reported TB outbreaks in health-care settings, multiple outbreaks involved transmission of MDR TB strains to both patients and HCWs (56,57,70,87,91–94). The majority of the patients and certain HCWs were HIV-infected, and progression to TB and MDR TB disease was rapid. Factors contributing to these outbreaks included delayed diagnosis of TB disease, delayed initiation and inadequate airborne precautions, lapses in AII practices and precautions for cough-inducing and aerosol-generating procedures, and lack of adequate respiratory protection. Multiple studies suggest that the decline in health-care–associated transmission observed in specific institutions is associated with the rigorous implementation of infection-control measures (11,12,18–20,23,95–97). Because various interventions were implemented simultaneously, the effectiveness of each intervention could not be determined.
After the release of the 1994 CDC infection-control guidelines, increased implementation of recommended infection-control measures occurred and was documented in multiple national surveys (13,15,98,99). In a survey of approximately 1,000 hospitals, a TST program was present in nearly all sites, and 70% reported having an AII room (13). Other surveys have documented improvement in the proportion of AII rooms meeting CDC criteria and proportion of HCWs using CDC-recommended respiratory protection and receiving serial TST (15,98). A survey of New York City hospitals with high caseloads of TB disease indicated 1) a decrease in the time that patients with TB disease spent in EDs before being transferred to a hospital room, 2) an increase in the proportion of patients initially placed in AII rooms, 3) an increase in the proportion of patients started on recommended antituberculosis treatment and reported to the local or state health department, and 4) an increase in the use of recommended respiratory protection and environmental controls (99). Reports of increased implementation of recommended TB infection controls combined with decreased reports of outbreaks of TB disease in health-care settings suggest that the recommended controls are effective in reducing and preventing health-care–associated transmission of M. tuberculosis (28).
Less information is available regarding the implementation of CDC-recommended TB infection-control measures in settings other than hospitals. One study identified major barriers to implementation that contribute to the costs of a TST program in health departments and hospitals, including personnel costs, HCWs' time off from work for TST administration and reading, and training and education of HCWs (100). Outbreaks have occurred in outpatient settings (i.e., private physicians' offices and pediatric settings) where the guidelines were not followed (101–103). CDC-recommended TB infection-control measures are implemented in correctional facilities, and certain variations might relate to resources, expertise, and oversight (104–106).
Fundamentals of TB Infection Control
One of the most critical risks for health-care–associated transmission of M. tuberculosis in health-care settings is from patients with unrecognized TB disease who are not promptly handled with appropriate airborne precautions (56,57,93,104) or who are moved from an AII room too soon (e.g., patients with unrecognized TB and MDR TB) (94). In the United States, the problem of MDR TB, which was amplified by health-care–associated transmission, has been substantially reduced by the use of standardized antituberculosis treatment regimens in the initial phase of therapy, rapid drug-susceptibility testing, directly observed therapy (DOT), and improved infection-control practices (1). DOT is an adherence-enhancing strategy in which an HCW or other specially trained health professional watches a patient swallow each dose of medication and records the dates that the administration was observed. DOT is the standard of care for all patients with TB disease and should be used for all doses during the course of therapy for TB disease and for LTBI whenever feasible.
All health-care settings need a TB infection-control program designed to ensure prompt detection, airborne precautions, and treatment of persons who have suspected or confirmed TB disease (or prompt referral of persons who have suspected TB disease for settings in which persons with TB disease are not expected to be encountered). Such a program is based on a three-level hierarchy of controls, including administrative, environmental, and respiratory protection (86,107,108).
Administrative Controls
The first and most important level of TB controls is the use of administrative measures to reduce the risk for exposure to persons who might have TB disease. Administrative controls consist of the following activities:
assigning responsibility for TB infection control in the setting;
conducting a TB risk assessment of the setting;
developing and instituting a written TB infection-control plan to ensure prompt detection, airborne precautions, and treatment of persons who have suspected or confirmed TB disease;
ensuring the timely availability of recommended laboratory processing, testing, and reporting of results to the ordering physician and infection-control team;
implementing effective work practices for the management of patients with suspected or confirmed TB disease;
ensuring proper cleaning and sterilization or disinfection of potentially contaminated equipment (usually endoscopes);
training and educating HCWs regarding TB, with specific focus on prevention, transmission, and symptoms;
screening and evaluating HCWs who are at risk for TB disease or who might be exposed to M. tuberculosis (i.e., TB screening program);
applying epidemiologic-based prevention principles, including the use of setting-related infection-control data;
using appropriate signage advising respiratory hygiene and cough etiquette; and
coordinating efforts with the local or state health department.
HCWs with TB disease should be allowed to return to work when they 1) have had three negative AFB sputum smear results (109–112) collected 8–24 hours apart, with at least one being an early morning specimen because respiratory secretions pool overnight; and 2) have responded to antituberculosis treatment that will probably be effective based on susceptibility results. In addition, HCWs with TB disease should be allowed to return to work when a physician knowledgeable and experienced in managing TB disease determines that HCWs are noninfectious (see Treatment Procedures for LTBI and TB Disease). Consideration should also be given to the type of setting and the potential risk to patients (e.g., general medical office versus HIV clinic) (see Supplements, Estimating the Infectiousness of a TB Patient; Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease).
Environmental Controls
The second level of the hierarchy is the use of environmental controls to prevent the spread and reduce the concentration of infectious droplet nuclei in ambient air.
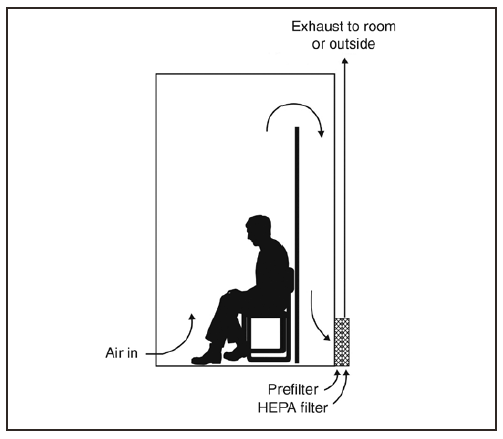
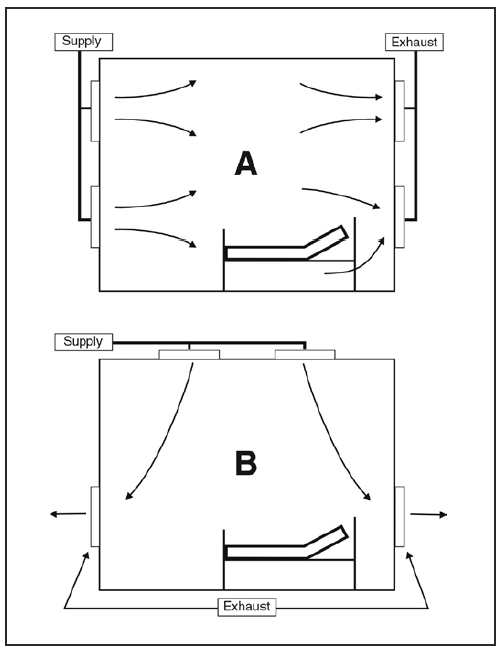
Primary environmental controls consist of controlling the source of infection by using local exhaust ventilation (e.g., hoods, tents, or booths) and diluting and removing contaminated air by using general ventilation.
Secondary environmental controls consist of controlling the airflow to prevent contamination of air in areas adjacent to the source (AII rooms) and cleaning the air by using high efficiency particulate air (HEPA) filtration or UVGI.
Respiratory-Protection Controls
The first two control levels minimize the number of areas in which exposure to M. tuberculosis might occur and, therefore, minimize the number of persons exposed. These control levels also reduce, but do not eliminate, the risk for exposure in the limited areas in which exposure can still occur. Because persons entering these areas might be exposed to M. tuberculosis, the third level of the hierarchy is the use of respiratory protective equipment in situations that pose a high risk for exposure. Use of respiratory protection can further reduce risk for exposure of HCWs to infectious droplet nuclei that have been expelled into the air from a patient with infectious TB disease (see Respiratory Protection). The following measures can be taken to reduce the risk for exposure:
implementing a respiratory-protection program,
training HCWs on respiratory protection, and
training patients on respiratory hygiene and cough etiquette procedures.
Relevance to Biologic Terrorism Preparedness
MDR M. tuberculosis is classified as a category C agent of biologic terrorism (113). Implementation of the TB infection-control guidelines described in this document is essential for preventing and controlling transmission of M. tuberculosis in health-care settings. Additional information is at http://www.bt.cdc.gov and http://www.idsociety.org/bt/toc.htm (114).
Recommendations for Preventing Transmission of M. tuberculosis in Health-Care Settings
TB Infection-Control Program
Every health-care setting should have a TB infection-control plan that is part of an overall infection-control program. The specific details of the TB infection-control program will differ, depending on whether patients with suspected or confirmed TB disease might be encountered in the setting or whether patients with suspected or confirmed TB disease will be transferred to another health-care setting. Administrators making this distinction should obtain medical and epidemiologic consultation from state and local health departments.
TB Infection-Control Program for Settings in Which Patients with Suspected or Confirmed TB Disease Are Expected To Be Encountered
The TB infection-control program should consist of administrative controls, environmental controls, and a respiratory-protection program. Every setting in which services are provided to persons who have suspected or confirmed infectious TB disease, including laboratories and nontraditional facility-based settings, should have a TB infection-control plan. The following steps should be taken to establish a TB infection-control program in these settings:
Assign supervisory responsibility for the TB infection-control program to a designated person or group with expertise in LTBI and TB disease, infection control, occupational health, environmental controls, and respiratory protection. Give the supervisor or supervisory body the support and authority to conduct a TB risk assessment, implement and enforce TB infection-control policies, and ensure recommended training and education of HCWs.
— Train the persons responsible for implementing and enforcing the TB infection-control program.
— Designate one person with a back-up as the TB resource person to whom questions and problems should be addressed, if supervisory responsibility is assigned to a committee.
Develop a written TB infection-control plan that outlines a protocol for the prompt recognition and initiation of airborne precautions of persons with suspected or confirmed TB disease, and update it annually.
Conduct a problem evaluation (see Problem Evaluation) if a case of suspected or confirmed TB disease is not promptly recognized and appropriate airborne precautions not initiated, or if administrative, environmental, or respiratory-protection controls fail.
Perform a contact investigation in collaboration with the local or state health department if health-care–associated transmission of M. tuberculosis is suspected (115). Implement and monitor corrective action.
Collaborate with the local or state health department to develop administrative controls consisting of the risk assessment, the written TB infection-control plan, management of patients with suspected or confirmed TB disease, training and education of HCWs, screening and evaluation of HCWs, problem evaluation, and coordination.
Implement and maintain environmental controls, including AII room(s) (see Environmental Controls).
Implement a respiratory-protection program.
Perform ongoing training and education of HCWs (see Suggested Components of an Initial TB Training and Education Program for HCWs).
Create a plan for accepting patients who have suspected or confirmed TB disease if they are transferred from another setting.
TB Infection-Control Program for Settings in Which Patients with Suspected or Confirmed TB Disease Are Not Expected To Be Encountered
Settings in which TB patients might stay before transfer should still have a TB infection-control program in place consisting of administrative, environmental, and respiratory-protection controls. The following steps should be taken to establish a TB infection-control program in these settings:
Assign responsibility for the TB infection-control program to appropriate personnel.
Develop a written TB infection-control plan that outlines a protocol for the prompt recognition and transfer of persons who have suspected or confirmed TB disease to another health-care setting. The plan should indicate procedures to follow to separate persons with suspected or confirmed infectious TB disease from other persons in the setting until the time of transfer. Evaluate the plan annually, if possible, to ensure that the setting remains one in which persons who have suspected or confirmed TB disease are not encountered and that they are promptly transferred.
Conduct a problem evaluation (see Problem Evaluation) if a case of suspected or confirmed TB disease is not promptly recognized, separated from others, and transferred.
Perform an investigation in collaboration with the local or state health department if health-care–associated transmission of M. tuberculosis is suspected.
Collaborate with the local or state health department to develop administrative controls consisting of the risk assessment and the written TB infection-control plan.
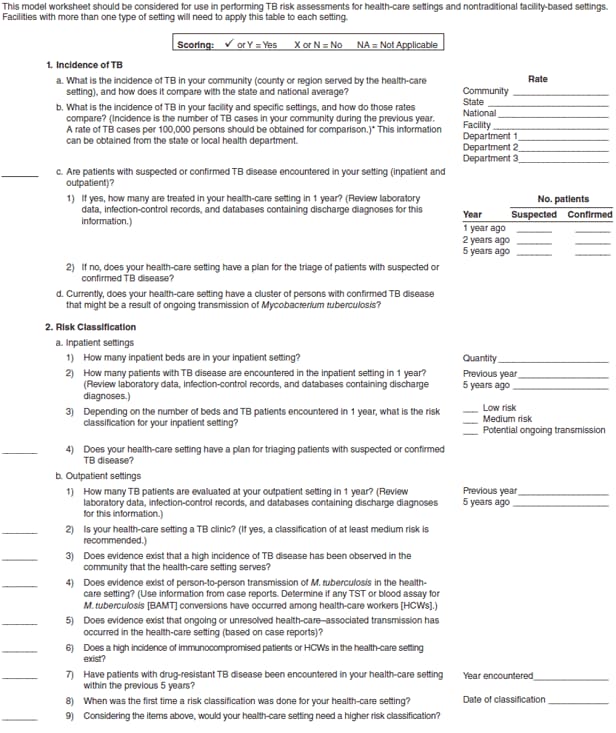
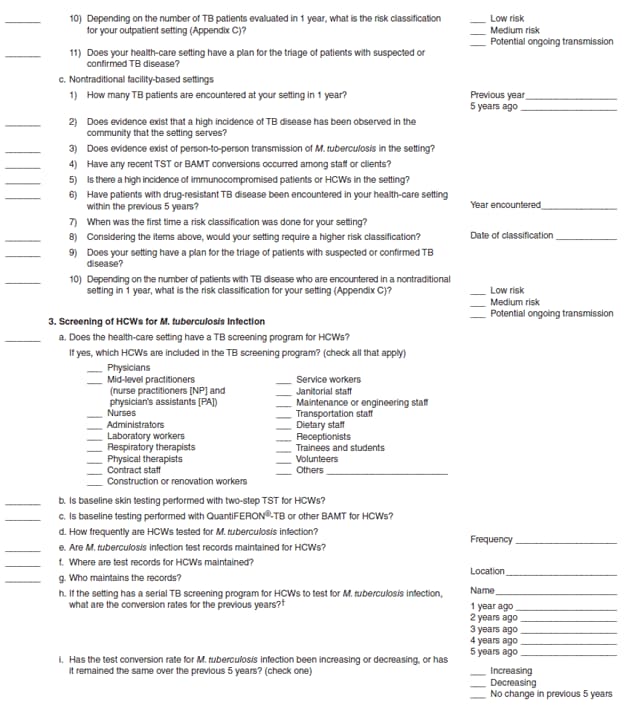
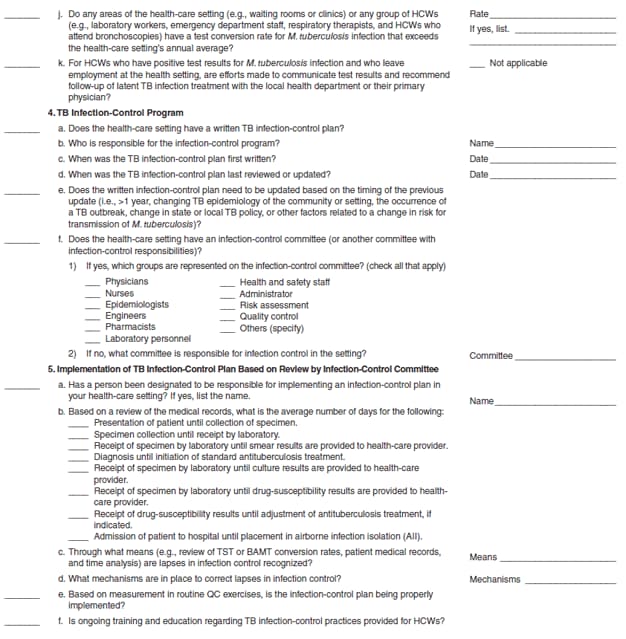
TB Risk Assessment
Every health-care setting should conduct initial and ongoing evaluations of the risk for transmission of M. tuberculosis, regardless of whether or not patients with suspected or confirmed TB disease are expected to be encountered in the setting. The TB risk assessment determines the types of administrative, environmental, and respiratory-protection controls needed for a setting and serves as an ongoing evaluation tool of the quality of TB infection control and for the identification of needed improvements in infection-control measures. Part of the risk assessment is similar to a program review that is conducted by the local TB-control program (42). The TB Risk Assessment Worksheet (Appendix B) can be used as a guide for conducting a risk assessment. This worksheet frequently does not specify values for acceptable performance indicators because of the lack of scientific data.
TB Risk Assessment for Settings in Which Patients with Suspected or Confirmed TB Disease Are Expected To Be Encountered
The initial and ongoing risk assessment for these settings should consist of the following steps:
Review the community profile of TB disease in collaboration with the state or local health department.
Consult the local or state TB-control program to obtain epidemiologic surveillance data necessary to conduct a TB risk assessment for the health-care setting.
Review the number of patients with suspected or confirmed TB disease who have been encountered in the setting during at least the previous 5 years.
Determine if persons with unrecognized TB disease have been admitted to or were encountered in the setting during the previous 5 years.
Determine which HCWs need to be included in a TB screening program and the frequency of screening (based on risk classification) (Appendix C).
Ensure the prompt recognition and evaluation of suspected episodes of health-care–associated transmission of M. tuberculosis.
Identify areas in the setting with an increased risk for health-care–associated transmission of M. tuberculosis, and target them for improved TB infection controls.
Assess the number of AII rooms needed for the setting. The risk classification for the setting should help to make this determination, depending on the number of TB patients examined. At least one AII room is needed for settings in which TB patients stay while they are being treated, and additional AII rooms might be needed, depending on the magnitude of patient-days of cases of suspected or confirmed TB disease. Additional AII rooms might be considered if options are limited for transferring patients with suspected or confirmed TB disease to other settings with AII rooms.
Determine the types of environmental controls needed other than AII rooms (see TB Airborne Precautions).
Determine which HCWs need to be included in the respiratory-protection program.
Conduct periodic reassessments (annually, if possible) to ensure
— proper implementation of the TB infection-control plan,
— prompt detection and evaluation of suspected TB cases,
— prompt initiation of airborne precautions of suspected infectious TB cases,
— recommended medical management of patients with suspected or confirmed TB disease (31),
— functional environmental controls,
— implementation of the respiratory-protection program, and
— ongoing HCW training and education regarding TB.
Recognize and correct lapses in infection control.
TB Risk Assessment for Settings in Which Patients with Suspected or Confirmed TB Disease Are Not Expected To Be Encountered
The initial and ongoing risk assessment for these settings should consist of the following steps:
Review the community profile of TB disease in collaboration with the local or state health department.
Consult the local or state TB-control program to obtain epidemiologic surveillance data necessary to conduct a TB risk assessment for the health-care setting.
Determine if persons with unrecognized TB disease were encountered in the setting during the previous 5 years.
Determine if any HCWs need to be included in the TB screening program.
Determine the types of environmental controls that are currently in place, and determine if any are needed in the setting (Appendices A and D).
Document procedures that ensure the prompt recognition and evaluation of suspected episodes of health-care–associated transmission of M. tuberculosis.
Conduct periodic reassessments (annually, if possible) to ensure 1) proper implementation of the TB infection-control plan; 2) prompt detection and evaluation of suspected TB cases; 3) prompt initiation of airborne precautions of suspected infectious TB cases before transfer; 4) prompt transfer of suspected infectious TB cases; 5) proper functioning of environmental controls, as applicable; and 6) ongoing TB training and education for HCWs.
Recognize and correct lapses in infection control.
Use of Risk Classification to Determine Need for TB Screening and Frequency of Screening HCWs
Risk classification should be used as part of the risk assessment to determine the need for a TB screening program for HCWs and the frequency of screening (Appendix C). A risk classification usually should be determined for the entire setting. However, in certain settings (e.g., health-care organizations that encompass multiple sites or types of services), specific areas defined by geography, functional units, patient population, job type, or location within the setting might have separate risk classifications. Examples of assigning risk classifications have been provided (see Risk Classification Examples).
TB Screening Risk Classifications
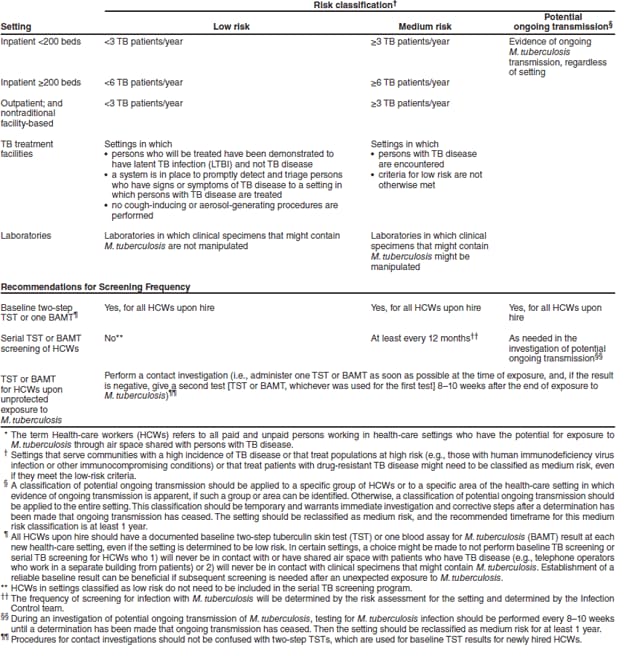
The three TB screening risk classifications are low risk, medium risk, and potential ongoing transmission. The classification of low risk should be applied to settings in which persons with TB disease are not expected to be encountered, and, therefore, exposure to M. tuberculosis is unlikely. This classification should also be applied to HCWs who will never be exposed to persons with TB disease or to clinical specimens that might contain M. tuberculosis.
The classification of medium risk should be applied to settings in which the risk assessment has determined that HCWs will or will possibly be exposed to persons with TB disease or to clinical specimens that might contain M. tuberculosis.
The classification of potential ongoing transmission should be temporarily applied to any setting (or group of HCWs) if evidence suggestive of person-to-person (e.g., patient-to-patient, patient-to-HCW, HCW-to-patient, or HCW-to-HCW) transmission of M. tuberculosis has occurred in the setting during the preceding year. Evidence of person-to-person transmission of M. tuberculosis includes 1) clusters of TST or BAMT conversions, 2) HCW with confirmed TB disease, 3) increased rates of TST or BAMT conversions, 4) unrecognized TB disease in patients or HCWs, or 5) recognition of an identical strain of M. tuberculosis in patients or HCWs with TB disease identified by deoxyribonucleic acid (DNA) fingerprinting.
If uncertainty exists regarding whether to classify a setting as low risk or medium risk, the setting typically should be classified as medium risk.
TB Screening Procedures for Settings (or HCWs) Classified as Low Risk
All HCWs should receive baseline TB screening upon hire, using two-step TST or a single BAMT to test for infection with M. tuberculosis.
After baseline testing for infection with M. tuberculosis, additional TB screening is not necessary unless an exposure to M. tuberculosis occurs.
HCWs with a baseline positive or newly positive test result for M. tuberculosis infection (i.e., TST or BAMT) or documentation of treatment for LTBI or TB disease should receive one chest radiograph result to exclude TB disease (or an interpretable copy within a reasonable time frame, such as 6 months). Repeat radiographs are not needed unless symptoms or signs of TB disease develop or unless recommended by a clinician (39,116).
TB Screening Procedures for Settings (or HCWs) Classified as Medium Risk
All HCWs should receive baseline TB screening upon hire, using two-step TST or a single BAMT to test for infection with M. tuberculosis.
After baseline testing for infection with M. tuberculosis, HCWs should receive TB screening annually (i.e., symptom screen for all HCWs and testing for infection with M. tuberculosis for HCWs with baseline negative test results).
HCWs with a baseline positive or newly positive test result for M. tuberculosis infection or documentation of previous treatment for LTBI or TB disease should receive one chest radiograph result to exclude TB disease. Instead of participating in serial testing, HCWs should receive a symptom screen annually. This screen should be accomplished by educating the HCW about symptoms of TB disease and instructing the HCW to report any such symptoms immediately to the occupational health unit. Treatment for LTBI should be considered in accordance with CDC guidelines (39).
TB Screening Procedures for Settings (or HCWs) Classified as Potential Ongoing Transmission
Testing for infection with M. tuberculosis might need to be performed every 8–10 weeks until lapses in infection control have been corrected, and no additional evidence of ongoing transmission is apparent.
The classification of potential ongoing transmission should be used as a temporary classification only. It warrants immediate investigation and corrective steps. After a determination that ongoing transmission has ceased, the setting should be reclassified as medium risk. Maintaining the classification of medium risk for at least 1 year is recommended.
Settings Adopting BAMT for Use in TB Screening
Settings that use TST as part of TB screening and want to adopt BAMT can do so directly (without any overlapping TST) or in conjunction with a period of evaluation (e.g., 1 or 2 years) during which time both TST and BAMT are used. Baseline testing for BAMT would be established as a single step test. As with the TST, BAMT results should be recorded in detail. The details should include date of blood draw, result in specific units, and the laboratory interpretation (positive, negative, or indeterminate—and the concentration of cytokine measured, for example, interferon-gamma [IFN-γ]).
Risk Classification Examples
Inpatient Settings with More Than 200 Beds
If less than six TB patients for the preceding year, classify as low risk. If greater than or equal to six TB patients for the preceding year, classify as medium risk.
Inpatient Settings with Less Than 200 Beds
If less than three TB patients for the preceding year, classify as low risk. If greater than or equal to three TB patients for the preceding year, classify as medium risk.
Outpatient, Outreach, and Home-Based Health-Care Settings
If less than three TB patients for the preceding year, classify as low risk. If greater than or equal to three TB patients for the preceding year, classify as medium risk.
Hypothetical Risk Classification Examples
The following hypothetical situations illustrate how assessment data are used to assign a risk classification. The risk classifications are for settings in which patients with suspected or confirmed infectious TB disease are expected to be encountered.
Example A. The setting is a 150-bed hospital located in a small city. During the preceding year, the hospital admitted two patients with a diagnosis of TB disease. One was admitted directly to an AII room, and one stayed on a medical ward for 2 days before being placed in an AII room. A contact investigation of exposed HCWs by hospital infection-control personnel in consultation with the state or local health department did not identify any health-care–associated transmission. Risk classification: low risk.
Example B. The setting is an ambulatory-care site in which a TB clinic is held 2 days per week. During the preceding year, care was delivered to six patients with TB disease and approximately 50 persons with LTBI. No instances of transmission of M. tuberculosis were noted. Risk classification: medium risk (because it is a TB clinic).
Example C. The setting is a large publicly funded hospital in a major metropolitan area. The hospital admits an average of 150 patients with TB disease each year, comprising 35% of the city burden. The setting has a strong TB infection-control program (i.e., annually updates infection-control plan, fully implements infection-control plan, and has enough AII rooms [see Environmental Controls]) and an annual conversion rate (for tests for M. tuberculosis infection) among HCWs of 0.5%. No evidence of health-care–associated transmission is apparent. The hospital has strong collaborative linkages with the state or local health department. Risk classification: medium risk (with close ongoing surveillance for episodes of transmission from unrecognized cases of TB disease, test conversions for M. tuberculosis infection in HCWs as a result of health-care–associated transmission, and specific groups or areas in which a higher risk for health-care–associated transmission exists).
Example D. The setting is an inpatient area of a correctional facility. A proportion of the inmates were born in countries where TB disease is endemic. Two cases of TB disease were diagnosed in inmates during the preceding year. Risk classification: medium risk (Correctional facilities should be classified as at least medium risk).
Example E. A hospital located in a large city admits 35 patients with TB disease per year, uses QFT-G to measure M. tuberculosis infection, and has an overall HCW M. tuberculosis infection test conversion rate of 1.0%. However, on annual testing, three of the 20 respiratory therapists tested had QFT-G conversions, for a rate of 15%. All of the respiratory therapists who tested positive received medical evaluations, had TB disease excluded, were diagnosed with LTBI, and were offered and completed a course of treatment for LTBI. None of the respiratory therapists had known exposures to M. tuberculosis outside the hospital. The problem evaluation revealed that 1) the respiratory therapists who converted had spent part of their time in the pulmonary function laboratory where induced sputum specimens were collected, and 2) the ventilation in the laboratory was inadequate. Risk classification: potential ongoing transmission for the respiratory therapists (because of evidence of health-care–associated transmission). The rest of the setting was classified as medium risk. To address the problem, booths were installed for sputum induction. On subsequent testing for M. tuberculosis infection, no conversions were noted at the repeat testing 3 months later, and the respiratory therapists were then reclassified back to medium risk.
Example F. The setting is an ambulatory-care center associated with a large health maintenance organization (HMO). The patient volume is high, and the HMO is located in the inner city where TB rates are the highest in the state. During the preceding year, one patient who was known to have TB disease was evaluated at the center. The person was recognized as a TB patient on his first visit and was promptly triaged to an ED with an AII room capacity. While in the ambulatory-care center, the patient was held in an area separate from HCWs and other patients and instructed to wear a surgical or procedure mask, if possible. QFT-G was used for infection-control surveillance purposes, and a contact investigation was conducted among exposed staff, and no QFT-G conversions were noted. Risk classification: low risk.
Example G. The setting is a clinic for the care of persons infected with HIV. The clinic serves a large metropolitan area and a patient population of 2,000. The clinic has an AII room and a TB infection-control program. All patients are screened for TB disease upon enrollment, and airborne precautions are promptly initiated for anyone with respiratory complaints while the patient is being evaluated. During the preceding year, seven patients who were encountered in the clinic were subsequently determined to have TB disease. All patients were promptly put into an AII room, and no contact investigations were performed. The local health department was promptly notified in all cases. Annual TST has determined a conversion rate of 0.3%, which is low compared with the rate of the hospital with which the clinic is associated. Risk classification: medium risk (because persons infected with HIV might be encountered).
Example H. A home health-care agency employs 125 workers, many of whom perform duties, including nursing, physical therapy, and basic home care. The agency did not care for any patients with suspected or confirmed TB disease during the preceding year. Approximately 30% of the agency's workers are foreign-born, many of whom have immigrated within the previous 5 years. At baseline two-step testing, four had a positive initial TST result, and two had a positive second-step TST result. All except one of these workers was foreign-born. Upon further screening, none were determined to have TB disease. The home health-care agency is based in a major metropolitan area and delivers care to a community where the majority of persons are poor and medically underserved and TB case rates are higher than the community as a whole. Risk classification: low risk (because HCWs might be from populations at higher risk for LTBI and subsequent progression to TB disease because of foreign birth and recent immigration or HIV-infected clients might be overrepresented, medium risk could be considered).
Screening HCWs Who Transfer to Other Health-Care Settings
All HCWs should receive baseline TB screening, even in settings considered to be low risk. Infection-control plans should address HCWs who transfer from one health-care setting to another and consider that the transferring HCWs might be at an equivalent or higher risk for exposure in different settings. Infection-control plans might need to be customized to balance the assessed risks and the efficacy of the plan based on consideration of various logistical factors. Guidance is provided based on different scenarios.
Because some institutions might adopt BAMT for the purposes of testing for M. tuberculosis infection, infection-control programs might be confronted with interpreting historic and current TST and BAMT results when HCWs transfer to a different setting. On a case-by-case basis, expert medical opinion might be needed to interpret results and refer patients with discordant BAMT and TST baseline results. Therefore, infection-control programs should keep all records when documenting previous test results. For example, an infection-control program using a BAMT strategy should request and keep historic TST results of a HCW transferring from a previous setting. Even if the HCW is transferring from a setting that used BAMT to a setting that uses BAMT, historic TST results might be needed when in the future the HCW transfers to a setting that uses TST. Similarly, historic BAMT results might be needed when the HCW transfers from a setting that used TST to a setting that uses BAMT.
HCWs transferring from low-risk to low-risk settings. After a baseline result for infection with M. tuberculosis is established and documented, serial testing for M. tuberculosis infection is not necessary.
HCWs transferring from low-risk to medium-risk settings. After a baseline result for infection with M. tuberculosis is established and documented, annual TB screening (including a symptom screen and TST or BAMT for persons with previously negative test results) should be performed.
HCWs transferring from low- or medium-risk settings to settings with a temporary classification of potential ongoing transmission. After a baseline result for infection with M. tuberculosis is established, a decision should be made regarding follow-up screening on an individual basis. If transmission seems to be ongoing, consider including the HCW in the screenings every 8–10 weeks until a determination has been made that ongoing transmission has ceased. When the setting is reclassified back to medium-risk, annual TB screening should be resumed.
Calculation and Use of Conversion Rates for M. tuberculosis Infection
The M. tuberculosis infection conversion rate is the percentage of HCWs whose test result for M. tuberculosis infection has converted within a specified period. Timely detection of M. tuberculosis infection in HCWs not only facilitates treatment for LTBI, but also can indicate the need for a source case investigation and a revision of the risk assessment for the setting. Conversion in test results for M. tuberculosis, regardless of the testing method used, is usually interpreted as presumptive evidence of new M. tuberculosis infection, and recent infections are associated with an increased risk for progression to TB disease.
For administrative purposes, a TST conversion is ≥10 mm increase in the size of the TST induration during a 2-year period in 1) an HCW with a documented negative (<10 mm) baseline two-step TST result or 2) a person who is not an HCW with a negative (<10 mm) TST result within 2 years.
In settings conducting serial testing for M. tuberculosis infection (medium-risk settings), use the following steps to estimate the risk for test conversion in HCWs.
Calculate a conversion rate by dividing the number of conversions among HCWs in the setting in a specified period (numerator) by the number of HCWs who received tests in the setting over the same period (denominator) multiplied by 100 (see Use of Conversion Test Data for M. tuberculosis Infection To Identify Lapses in Infection Control).
Identify areas or groups in the setting with a potentially high risk for M. tuberculosis transmission by comparing conversion rates in HCWs with potential exposure to patients with TB disease to conversion rates in HCWs for whom health-care–associated exposure to M. tuberculosis is not probable.
Use of Conversion Test Data for M. tuberculosis Infection To Identify Lapses in Infection Control
Conversion rates above the baseline level (which will be different in each setting) should instigate an investigation to evaluate the likelihood of health-care–associated transmission. When testing for M. tuberculosis infection, if conversions are determined to be the result of well-documented community exposure or probable false-positive test results, then the risk classification of the setting does not need to be adjusted.
For settings that no longer perform serial testing for M. tuberculosis infection among HCWs, reassessment of the risk for the setting is essential to ensure that the infection-control program is effective. The setting should have ongoing communication with the local or state health department regarding incidence and epidemiology of TB in the population served and should ensure that timely contact investigations are performed for HCWs or patients with unprotected exposure to a person with TB disease.
Example Calculation of Conversion Rates
Medical Center A is classified as medium risk and uses TST for annual screening. At the end of 2004, a total of 10,051 persons were designated as HCWs. Of these, 9,246 had negative baseline test results for M. tuberculosis infection. Of the HCWs tested, 10 experienced an increase in TST result by ≥10 mm. The overall setting conversion rate for 2004 is 0.11%. If five of the 10 HCWs whose test results converted were among the 100 HCWs employed in the ICU of Hospital X (in Medical Center A), then the ICU setting-specific conversion rate for 2004 is 5%.
Evaluation of HCWs for LTBI should include information from a serial testing program, but this information must be interpreted as only one part of a full assessment. TST or BAMT conversion criteria for administrative (surveillance) purposes are not applicable for medical evaluation of HCWs for the diagnosis of LTBI (see Supplement, Surveillance and Detection of M. tuberculosis Infections in Health-Care Workers [HCWs]).
Evaluation of TB Infection-Control Procedures and Identification of Problems
Annual evaluations of the TB infection-control plan are needed to ensure the proper implementation of the plan and to recognize and correct lapses in infection control. Previous hospital admissions and outpatient visits of patients with TB disease should be noted before the onset of TB symptoms. Medical records of a sample of patients with suspected and confirmed TB disease who were treated or examined at the setting should be reviewed to identify possible problems in TB infection control. The review should be based on the factors listed on the TB Risk Assessment Worksheet (Appendix B).
Time interval from suspicion of TB until initiation of airborne precautions and antituberculosis treatment to:
— suspicion of TB disease and patient triage to proper AII room or referral center for settings that do not provide care for patients with suspected or confirmed TB disease;
— admission until TB disease was suspected;
— admission until medical evaluation for TB disease was performed;
— admission until specimens for AFB smears and polymerase chain reaction (PCR)–based nucleic acid amplification (NAA) tests for M. tuberculosis were ordered;
— admission until specimens for mycobacterial culture were ordered;
— ordering of AFB smears, NAA tests, and mycobacterial culture until specimens were collected;
— collection of specimens until performance and AFB smear results were reported;
— collection of specimens until performance and culture results were reported;
— collection of specimens until species identification was reported;
— collection of specimens until drug-susceptibility test results were reported;
— admission until airborne precautions were initiated; and
— admission until antituberculosis treatment was initiated.
Duration of airborne precautions.
Measurement of meeting criteria for discontinuing airborne precautions. Certain patients might be correctly discharged from an AII room to home.
Patient history of previous admission.
Adequacy of antituberculosis treatment regimens.
Adequacy of procedures for collection of follow-up sputum specimens.
Adequacy of discharge planning.
Number of visits to outpatient setting from the start of symptoms until TB disease was suspected (for outpatient settings).
Work practices related to airborne precautions should be observed to determine if employers are enforcing all practices, if HCWs are adhering to infection-control policies, and if patient adherence to airborne precautions is being enforced. Data from the case reviews and observations in the annual risk assessment should be used to determine the need to modify 1) protocols for identifying and initiating prompt airborne precautions for patients with suspected or confirmed infectious TB disease, 2) protocols for patient management, 3) laboratory procedures, or 4) TB training and education programs for HCWs.
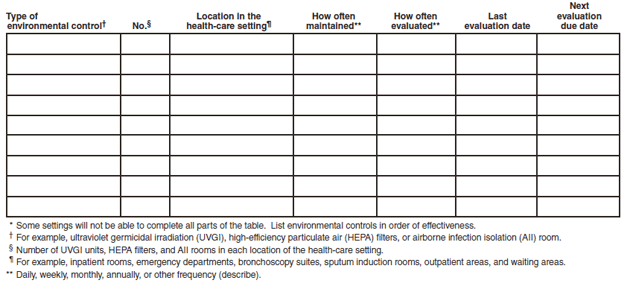
Environmental Assessment
Data from the most recent environmental evaluation should be reviewed to determine if recommended environmental controls are in place (see Suggested Components of an Initial TB Training and Education Program for HCWs).
Environmental control maintenance procedures and logs should be reviewed to determine if maintenance is conducted properly and regularly.
Environmental control design specifications should be compared with guidelines from the American Institute of Architects (AIA) and other ventilation guidelines (117,118) (see Risk Classification Examples) and the installed system performance.
Environmental data should be used to assist building managers and engineers in evaluating the performance of the installed system.
The number and types of aerosol-generating or aerosol-producing procedures (e.g., specimen processing and manipulation, bronchoscopy, sputum induction, and administration of aerosolized medications) performed in the setting should be assessed.
The number of AII rooms should be suitable for the setting based on AIA Guidelines and the setting risk assessment. The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has adapted the AIA guidelines when accrediting facilities (118).
Suggested Components of an Initial TB Training and Education Program for HCWs
The following are suggested components of an initial TB training and education program:
1. Clinical Information
Basic concepts of M. tuberculosis transmission, pathogenesis, and diagnosis, including the difference between LTBI and TB disease and the possibility of reinfection after previous infection with M. tuberculosis or TB disease.
Symptoms and signs of TB disease and the importance of a high index of suspicion for patients or HCWs with these symptoms.
Indications for initiation of airborne precautions of inpatients with suspected or confirmed TB disease.
Policies and indications for discontinuing airborne precautions.
Principles of treatment for LTBI and for TB disease (indications, use, effectiveness, and potential adverse effects).
2. Epidemiology of TB
Epidemiology of TB in the local community, the United States, and worldwide.
Risk factors for TB disease.
3. Infection-Control Practices to Prevent and Detect M. tuberculosis Transmission in Health-Care Settings
Overview of the TB infection-control program.
Potential for occupational exposure to infectious TB disease in health-care settings.
Principles and practices of infection control to reduce the risk for transmission of M. tuberculosis, including the hierarchy of TB infection-control measures, written policies and procedures, monitoring, and control measures for HCWs at increased risk for exposure to M. tuberculosis.
Rationale for infection-control measures and documentation evaluating the effect of these measures in reducing occupational TB risk exposure and M. tuberculosis transmission.
Reasons for testing for M. tuberculosis infection, importance of a positive test result for M. tuberculosis infection, importance of participation in a TB screening program, and importance of retaining documentation of previous test result for M. tuberculosis infection, chest radiograph results, and treatment for LTBI and TB disease.
Efficacy and safety of BCG vaccination and principles of screening for M. tuberculosis infection and interpretation in BCG recipients.
Procedures for investigating an M. tuberculosis infection test conversion or TB disease occurring in the workplace.
Joint responsibility of HCWs and employers to ensure prompt medical evaluation after M. tuberculosis test conversion or development of symptoms or signs of TB disease in HCWs.
Role of HCW in preventing transmission of M. tuberculosis.
Responsibility of HCWs to promptly report a diagnosis of TB disease to the setting's administration and infection-control program.
Responsibility of clinicians and the infection-control program to report to the state or local health department a suspected case of TB disease in a patient (including autopsy findings) or HCW.
Responsibilities and policies of the setting, the local health department, and the state health department to ensure confidentiality for HCWs with TB disease or LTBI.
Responsibility of the setting to inform EMS staff who transported a patient with suspected or confirmed TB disease.
Responsibilities and policies of the setting to ensure that an HCW with TB disease is noninfectious before returning to duty.
Importance of completing therapy for LTBI or TB disease to protect the HCW's health and to reduce the risk to others.
Proper implementation and monitoring of environmental controls (see Environmental Controls).
Training for safe collection, management, and disposal of clinical specimens.
Required Occupational Safety and Health Administration (OSHA) record keeping on HCW test conversions for M. tuberculosis infection.
Record-keeping and surveillance of TB cases among patients in the setting.
Proper use of (see Respiratory Protection) and the need to inform the infection-control program of factors that might affect the efficacy of respiratory protection as required by OSHA.
Success of adherence to infection-control practices in decreasing the risk for transmission of M. tuberculosis in health-care settings.
4. TB and Immunocompromising Conditions
Relationship between infection with M. tuberculosis and medical conditions and treatments that can lead to impaired immunity.
Available tests and counseling and referrals for persons with HIV infection, diabetes, and other immunocompromising conditions associated with an increased risk for progression to TB disease.
Procedures for informing employee health or infection-control personnel of medical conditions associated with immunosuppression.
Policies on voluntary work reassignment options for immunocompromised HCWs.
Applicable confidentiality safeguards of the health-care setting, locality, and state.
5. TB and Public Health
Role of the local and state health department's TB-control program in screening for LTBI and TB disease, providing treatment, conducting contact investigations and outbreak investigations, and providing education, counseling, and responses to public inquiries.
Roles of CDC and of OSHA.
Availability of information, advice, and counseling from community sources, including universities, local experts, and hotlines.
Responsibility of the setting's clinicians and infection-control program to promptly report to the state or local health department a case of suspected TB disease or a cluster of TST or BAMT conversions.
Responsibility of the setting's clinicians and infection-control program to promptly report to the state or local health department a person with suspected or confirmed TB disease who leaves the setting against medical advice.
Managing Patients Who Have Suspected or Confirmed TB Disease: General Recommendations
The primary TB risk to HCWs is the undiagnosed or unsuspected patient with infectious TB disease. A high index of suspicion for TB disease and rapid implementation of precautions are essential to prevent and interrupt transmission. Specific precautions will vary depending on the setting.
Prompt Triage
Within health-care settings, protocols should be implemented and enforced to promptly identify, separate from others, and either transfer or manage persons who have suspected or confirmed infectious TB disease. When patients' medical histories are taken, all patients should be routinely asked about 1) a history of TB exposure, infection, or disease; 2) symptoms or signs of TB disease; and 3) medical conditions that increase their risk for TB disease (see Supplements, Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease). The medical evaluation should include an interview conducted in the patient's primary language, with the assistance of a qualified medical interpreter, if necessary. HCWs who are the first point of contact should be trained to ask questions that will facilitate detection of persons who have suspected or confirmed infectious TB disease. For assistance with language interpretation, contact the local and state health department. Interpretation resources are also available (119) at http://www.atanet.org; http://www.languageline.com; and http://www.ncihc.org.
A diagnosis of respiratory TB disease should be considered for any patient with symptoms or signs of infection in the lung, pleura, or airways (including larynx), including coughing for ≥3 weeks, loss of appetite, unexplained weight loss, night sweats, bloody sputum or hemoptysis, hoarseness, fever, fatigue, or chest pain. The index of suspicion for TB disease will vary by geographic area and will depend on the population served by the setting. The index of suspicion should be substantially high for geographic areas and groups of patients characterized by high TB incidence (26).
Special steps should be taken in settings other than TB clinics. Patients with symptoms suggestive of undiagnosed or inadequately treated TB disease should be promptly referred so that they can receive a medical evaluation. These patients should not be kept in the setting any longer than required to arrange a referral or transfer to an AII room. While in the setting, symptomatic patients should wear a surgical or procedure mask, if possible, and should be instructed to observe strict respiratory hygiene and cough etiquette procedures (see Glossary) (120–122).
Immunocompromised persons, including those who are HIV-infected, with infectious TB disease should be physically separated from other persons to protect both themselves and others. To avoid exposing HIV-infected or otherwise severely immunocompromised persons to M. tuberculosis, consider location and scheduling issues to avoid exposure.
TB Airborne Precautions
Within health-care settings, TB airborne precautions should be initiated for any patient who has symptoms or signs of TB disease, or who has documented infectious TB disease and has not completed antituberculosis treatment. For patients placed in AII rooms because of suspected infectious TB disease of the lungs, airway, or larynx, airborne precautions may be discontinued when infectious TB disease is considered unlikely and either 1) another diagnosis is made that explains the clinical syndrome or 2) the patient has three consecutive, negative AFB sputum smear results (109–112,123). Each of the three sputum specimens should be collected in 8–24-hour intervals (124), and at least one specimen should be an early morning specimen because respiratory secretions pool overnight. Generally, this method will allow patients with negative sputum smear results to be released from airborne precautions in 2 days.
The classification of the risk assessment of the health-care setting is used to determine how many AII rooms each setting needs, depending on the number of TB patients examined. At least one AII room is needed for settings in which TB patients stay while they are being treated, and additional AII rooms might be needed depending on the magnitude of patient-days of persons with suspected or confirmed TB disease (118). Additional rooms might be considered if options are limited for transferring patients with suspected or confirmed TB disease to other settings with AII rooms. For example, for a hospital with 120 beds, a minimum of one AII room is needed, possibly more, depending on how many TB patients are examined in 1 year.
TB Airborne Precautions for Settings in Which Patients with Suspected or Confirmed TB Disease Are Expected To Be Encountered
Settings that plan to evaluate and manage patients with TB disease should have at least one AII room or enclosure that meets AII requirements (see Environmental Controls; and Supplement, Environmental Controls). These settings should develop written policies that specify 1) indications for airborne precautions, 2) persons authorized to initiate and discontinue airborne precautions, 3) specific airborne precautions, 4) AII room-monitoring procedures, 5) procedures for managing patients who do not adhere to airborne precautions, and 6) criteria for discontinuing airborne precautions.
A high index of suspicion should be maintained for TB disease. If a patient has suspected or confirmed TB disease, airborne precautions should be promptly initiated. Persons with suspected or confirmed TB disease who are inpatients should remain in AII rooms until they are determined to be noninfectious and have demonstrated a clinical response to a standard multidrug antituberculosis treatment regimen or until an alternative diagnosis is made. If the alternative diagnosis cannot be clearly established, even with three negative sputum smear results, empiric treatment of TB disease should strongly be considered (see Supplement, Estimating the Infectiousness of a TB Patient). Outpatients with suspected or confirmed infectious TB disease should remain in AII rooms until they are transferred or until their visit is complete.
TB Airborne Precautions for Settings in Which Patients with Suspected or Confirmed TB Disease Are Not Expected To Be Encountered
Settings in which patients with suspected or confirmed TB disease are not expected to be encountered do not need an AII room or a respiratory-protection program for the prevention of transmission of M. tuberculosis. However, follow these steps in these settings.
A written protocol should be developed for referring patients with suspected or confirmed TB disease to a collaborating referral setting in which the patient can be evaluated and managed properly. The referral setting should provide documentation of intent to collaborate. The protocol should be reviewed routinely and revised as needed.
Patients with suspected or confirmed TB disease should be placed in an AII room, if available, or in a room that meets the requirements for an AII room, or in a separate room with the door closed, apart from other patients and not in an open waiting area. Adequate time should elapse to ensure removal of M. tuberculosis–contaminated room air before allowing entry by staff or another patient (Tables 1 and
2).
If an AII room is not available, persons with suspected or confirmed infectious TB disease should wear a surgical or procedure mask, if possible. Patients should be instructed to keep the mask on and to change the mask if it becomes wet. If patients cannot tolerate a mask, they should observe strict respiratory hygiene and cough etiquette procedures.
AII Room Practices
AII rooms should be single-patient rooms in which environmental factors and entry of visitors and HCWs are controlled to minimize the transmission of M. tuberculosis. All HCWs who enter an AII room should wear at least N95 disposable respirators (see Respiratory Protection). Visitors may be offered respiratory protection (i.e., N95) and should be instructed by HCWs on the use of the respirator before entering an AII room. AII rooms have specific requirements for controlled ventilation, negative pressure, and air filtration (118) (see Environmental Controls). Each inpatient AII room should have a private bathroom.
Settings with AII Rooms
Health-care personnel settings with AII rooms should
keep doors to AII rooms closed except when patients, HCWs, or others must enter or exit the room (118);
maintain enough AII rooms to provide airborne precautions of all patients who have suspected or confirmed TB disease. Estimate the number of AII rooms needed based on the results of the risk assessment for the setting;
monitor and record direction of airflow (i.e., negative pressure) in the room on a daily basis, while the room is being used for TB airborne precautions. Record results in an electronic or readily retrievable document;
consider grouping AII rooms in one part of the health-care setting to limit costs, reduce the possibility of transmitting M. tuberculosis to other patients, facilitate the care of TB patients, and facilitate the installation and maintenance of optimal environmental controls (particularly ventilation). Depending on the architecture and the environmental control systems of a particular setting, AII rooms might be grouped either horizontally (e.g., a wing of a facility) or vertically (e.g., the last few rooms of separate floors of a facility);
perform diagnostic and treatment procedures (e.g., sputum collection and inhalation therapy) in an AII room.
ensure patient adherence to airborne precautions. In their primary language, with the assistance of a qualified medical interpreter, if necessary, educate patients (and family and visitors) who are placed in an AII room about M. tuberculosis transmission and the reasons for airborne precautions. For assistance with language interpretation, contact the local and state health department. Interpretation resources are available (119) at http://www.atanet.org; http://www.languageline.com; and http://www.ncihc.org. Facilitate patient adherence by using incentives (e.g., provide telephones, televisions, or radios in AII rooms; and grant special dietary requests) and other measures. Address problems that could interfere with adherence (e.g., management of withdrawal from addictive substances, including tobacco); and
ensure that patients with suspected or confirmed infectious TB disease who must be transported to another area of the setting or to another setting for a medically essential procedure bypass the waiting area and wear a surgical or procedure mask, if possible. Drivers, HCWs, and other staff who are transporting persons with suspected or confirmed infectious TB disease might consider wearing an N95 respirator. Schedule procedures on patients with TB disease when a minimum number of HCWs and other patients are present and as the last procedure of the day to maximize the time available for removal of airborne contamination (Tables 1 and
2).
Diagnostic Procedures
Diagnostic procedures should be performed in settings with appropriate infection-control capabilities. The following recommendations should be applied for diagnosing TB disease and for evaluating patients for potential infectiousness.
Clinical Diagnosis
A complete medical history should be obtained, including symptoms of TB disease, previous TB disease and treatment, previous history of infection with M. tuberculosis, and previous treatment of LTBI or exposure to persons with TB disease. A physical examination should be performed, including chest radiograph, microscopic examination, culture, and, when indicated, NAA testing of sputum (39,53,125,126). If possible, sputum induction with aerosol inhalation is preferred, particularly when the patient cannot produce sputum. Gastric aspiration might be necessary for those patients, particularly children, who cannot produce sputum, even with aerosol inhalation (127–130). Bronchoscopy might be needed for specimen collection, especially if sputum specimens have been nondiagnostic and doubt exists as to the diagnosis (90,111,127,128,131–134).
All patients with suspected or confirmed infectious TB disease should be placed under airborne precautions until they have been determined to be noninfectious (see Supplement, Estimating the Infectiousness of a TB Patient). Adult and adolescent patients who might be infectious include persons who are coughing; have cavitation on chest radiograph; have positive AFB sputum smear results; have respiratory tract disease with involvement of the lung, pleura or airways, including larynx, who fail to cover the mouth and nose when coughing; are not on antituberculosis treatment or are on incorrect antituberculosis treatment; or are undergoing cough-inducing or aerosol-generating procedures (e.g., sputum induction, bronchoscopy, and airway suction) (30,135).
Persons diagnosed with extrapulmonary TB disease should be evaluated for the presence of concurrent pulmonary TB disease. An additional concern in infection control with children relates to adult household members and visitors who might be the source case (136). Pediatric patients, including adolescents, who might be infectious include those who have extensive pulmonary or laryngeal involvement, prolonged cough, positive sputum AFB smears results, cavitary TB on chest radiograph (as is typically observed in immunocompetent adults with TB disease), or those for whom cough-inducing or aerosol-generating procedures are performed (136,137).
Although children are uncommonly infectious, pediatric patients should be evaluated for infectiousness by using the same criteria as for adults (i.e., on the basis of pulmonary or laryngeal involvement). Patients with suspected or confirmed TB disease should be immediately reported to the local public health authorities so that arrangements can be made for tracking their treatment to completion, preferably through a case management system, so that DOT can be arranged and standard procedures for identifying and evaluating TB contacts can be initiated. Coordinate efforts with the local or state health department to arrange treatment and long-term follow-up and evaluation of contacts.
Laboratory Diagnosis
To produce the highest quality laboratory results, laboratories performing mycobacteriologic tests should be skilled in both the laboratory and the administrative aspects of specimen processing. Laboratories should use or have prompt access to the most rapid methods available: 1) fluorescent microscopy and concentration for AFB smears; 2) rapid NAA testing for direct detection of M. tuberculosis in patient specimens (125); 3) solid and rapid broth culture methods for isolation of mycobacteria; 4) nucleic acid probes or high pressure liquid chromatography (HPLC) for species identification; and 5) rapid broth culture methods for drug susceptibility testing. Laboratories should incorporate other more rapid or sensitive tests as they become available, practical, and affordable (see Supplement, Diagnostic Procedures for LTBI and TB Disease) (138,139).
In accordance with local and state laws and regulations, a system should be in place to ensure that laboratories report any positive results from any specimens to clinicians within 24 hours of receipt of the specimen (139,140). Certain settings perform AFB smears on-site for rapid results (and results should be reported to clinicians within 24 hours) and then send specimens or cultures to a referral laboratory for identification and drug-susceptibility testing. This referral practice can speed the receipt of smear results but delay culture identification and drug-susceptibility results. Settings that cannot provide the full range of mycobacteriologic testing services should contract with their referral laboratories to ensure rapid results while maintaining proficiency for on-site testing. In addition, referral laboratories should be instructed to store isolates in case additional testing is necessary.
All drug susceptibility results on M. tuberculosis isolates should be reported to the local or state health department as soon as these results are available. Laboratories that rarely receive specimens for mycobacteriologic analysis should refer specimens to a laboratory that performs these tests routinely. The reference laboratory should provide rapid testing and reporting. Out-of-state reference laboratories should provide all results to the local or state health department from which the specimen originated.
Special Considerations for Persons Who Are at High Risk for TB Disease or in Whom TB Disease Might Be Difficult to Diagnose
The probability of TB disease is higher among patients who 1) previously had TB disease or were exposed to M. tuberculosis, 2) belong to a group at high risk for TB disease or, 3) have a positive TST or BAMT result. TB disease is strongly suggested if the diagnostic evaluation reveals symptoms or signs of TB disease, a chest radiograph consistent with TB disease, or AFB in sputum or from any other specimen. TB disease can occur simultaneously in immunocompromised persons who have pulmonary infections caused by other organisms (e.g., Pneumocystis jaroveci [formerly P. carinii] and M. avium complex) and should be considered in the diagnostic evaluation of all such patients with symptoms or signs of TB disease (53).
TB disease can be difficult to diagnose in persons who have HIV infection (49) (or other conditions associated with severe suppression of cell mediated immunity) because of nonclassical or normal radiographic presentation or the simultaneous occurrence of other pulmonary infections (e.g., P. jaroveci or M. avium complex) (2). Patients who are HIV-infected are also at greater risk for having extrapulmonary TB (2). The difficulty in diagnosing TB disease in HIV-infected can be compounded by the possible lower sensitivity and specificity of sputum smear results for detecting AFB (53,141) and the overgrowth of cultures with M. avium complex in specimens from patients infected with both M. tuberculosis and M. avium complex. The TST in patients with advanced HIV infection is unreliable and cannot be used in clinical decision making (35,53,142).
For immunocompromised patients who have respiratory symptoms or signs that are attributed initially to infections or conditions other than TB disease, conduct an evaluation for coexisting TB disease. If the patient does not respond to recommended treatment for the presumed cause of the pulmonary abnormalities, repeat the evaluation (see Supplement, Diagnostic Procedures for LTBI and TB Disease). In certain settings in which immunocompromised patients and patients with TB disease are examined, implementing airborne precautions might be prudent for all persons at high risk. These persons include those infected with HIV who have an abnormal chest radiograph or respiratory symptoms, symptomatic foreign-born persons who have immigrated within the previous 5 years from TB-endemic countries, and persons with pulmonary infiltrates on chest radiograph, or symptoms or signs of TB disease.
Initiation of Treatment
For patients who have confirmed TB disease or who are considered highly probable to have TB disease, promptly start antituberculosis treatment in accordance with current guidelines (see Supplements, Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease) (31). In accordance with local and state regulations, local health departments should be notified of all cases of suspected TB.
DOT is the standard of care for all patients with TB disease and should be used for all doses during the course of therapy for treatment of TB disease. All inpatient medication should be administered by DOT and reported to the state or local health department. Rates of relapse and development of drug-resistance are decreased when DOT is used (143–145). All patients on intermittent (i.e., once or twice per week) treatment for TB disease or LTBI should receive DOT. Settings should collaborate with the local or state health department on decisions concerning inpatient DOT and arrangements for outpatient DOT (31).
Managing Patients Who Have Suspected or Confirmed TB Disease: Considerations for Special Circumstances and Settings
The recommendations for preventing transmission of M. tuberculosis are applicable to all health-care settings, including those that have been described (Appendix A). These settings should each have independent risk assessments if they are stand-alone settings, or each setting should have a detailed section written as part of the risk assessment for the overall setting.
Minimum Requirements
The specific precautions for the settings included in this section vary, depending on the setting.
Inpatient Settings
Emergency Departments (EDs)
The symptoms of TB disease are usually symptoms for which patients might seek treatment in EDs. Because TB symptoms are common and nonspecific, infectious TB disease could be encountered in these settings. The use of ED-based TB screening has not been demonstrated to be consistently effective (146).
The amount of time patients with suspected or confirmed infectious TB disease spend in EDs and urgent-care settings should be minimized. Patients with suspected or confirmed infectious TB disease should be promptly identified, evaluated, and separated from other patients. Ideally, such patients should be placed in an AII room. When an AII room is not available, use a room with effective general ventilation, and use air cleaning technologies (e.g., a portable HEPA filtration system), if available, or transfer the patient to a setting or area with recommended infection-control capacity. Facility engineering personnel with expertise in heating, ventilation, and air conditioning (HVAC) and air handlers have evaluated how this option is applied to ensure no over pressurization of return air or unwanted deviations exists in design of air flow in the zone.
EDs with a high volume of patients with suspected or confirmed TB disease should have at least one AII room (see TB Risk Assessment). Air-cleaning technologies (e.g., HEPA filtration and UVGI) can be used to increase equivalent air changes per hour (ACH) in waiting areas (Table 1). HCWs entering an AII room or any room with a patient with infectious TB disease should wear at least an N95 disposable respirator. After a patient with suspected or confirmed TB disease exits a room, allow adequate time to elapse to ensure removal of M. tuberculosis-contaminated room air before allowing entry by staff or another patient (Tables 1 and
2).
Before a patient leaves an AII room, perform an assessment of 1) the patient's need to discontinue airborne precautions, 2) the risk for transmission and the patient's ability to observe strict respiratory hygiene, and 3) cough etiquette procedures. Patients with suspected or confirmed infectious TB who are outside an AII room should wear a surgical or procedure mask, if possible. Patients who cannot tolerate masks because of medical conditions should observe strict respiratory hygiene and cough etiquette procedures.
Intensive Care Units (ICUs)
Patients with infectious TB disease might become sick enough to require admission to an ICU. Place ICU patients with suspected or confirmed infectious TB disease in an AII room, if possible. ICUs with a high volume of patients with suspected or confirmed TB disease should have at least one AII room (Appendix B). Air-cleaning technologies (e.g., HEPA filtration and UVGI) can be used to increase equivalent ACH in waiting areas (see Environmental Controls).
HCWs entering an AII room or any room with a patient with infectious TB disease should wear at least an N95 disposable respirator. To help reduce the risk for contaminating a ventilator or discharging M. tuberculosis into the ambient air when mechanically ventilating (i.e., with a ventilator or manual resuscitator) a patient with suspected or confirmed TB disease, place a bacterial filter on the patient's endotracheal tube (or at the expiratory side of the breathing circuit of a ventilator) (147–151). In selecting a bacterial filter, give preference to models specified by the manufacturer to filter particles 0.3 µm in size in both the unloaded and loaded states with a filter efficiency of ≥95% (i.e., filter penetration of <5%) at the maximum design flow rates of the ventilator for the service life of the filter, as specified by the manufacturer.
Surgical Suites
Surgical suites require special infection-control considerations for preventing transmission of M. tuberculosis. Normally, the direction of airflow should be from the operating room (OR) to the hallway (positive pressure) to minimize contamination of the surgical field. Certain hospitals have procedure rooms with reversible airflow or pressure, whereas others have positive-pressure rooms with a negative pressure anteroom. Surgical staff, particularly those close to the surgical field, should use respiratory protection (e.g., a valveless N95 disposable respirator) to protect themselves and the patient undergoing surgery.
When possible, postpone non-urgent surgical procedures on patients with suspected or confirmed TB disease until the patient is determined to be noninfectious or determined to not have TB disease. When surgery cannot be postponed, procedures should be performed in a surgical suite with recommended ventilation controls. Procedures should be scheduled for patients with suspected or confirmed TB disease when a minimum number of HCWs and other patients are present in the surgical suite, and at the end of the day to maximize the time available for removal of airborne contamination (Tables 1 and
2).
If a surgical suite or an OR has an anteroom, the anteroom should be either 1) positive pressure compared with both the corridor and the suite or OR (with filtered supply air) or 2) negative pressure compared with both the corridor and the suite or OR. In the usual design in which an OR has no anteroom, keep the doors to the OR closed, and minimize traffic into and out of the room and in the corridor. Using additional air-cleaning technologies (e.g., UVGI) should be considered to increase the equivalent ACH. Air-cleaning systems can be placed in the room or in surrounding areas to minimize contamination of the surroundings after the procedure (114) (see Environmental Controls).
Ventilation in the OR should be designed to provide a sterile environment in the surgical field while preventing contaminated air from flowing to other areas in the health-care setting. Personnel steps should be taken to reduce the risk for contaminating ventilator or anesthesia equipment or discharging tubercle bacilli into the ambient air when operating on a patient with suspected or confirmed TB disease (152). A bacterial filter should be placed on the patient's endotracheal tube (or at the expiratory side of the breathing circuit of a ventilator or anesthesia machine, if used) (147–151). When selecting a bacterial filter, give preference to models specified by the manufacturer to filter particles 0.3 µm in size in both the unloaded and loaded states with a filter efficiency of ≥95% (i.e., filter penetration of <5%) at the maximum design flow rates of the ventilator for the service life of the filter, as specified by the manufacturer.
When surgical procedures (or other procedures that require a sterile field) are performed on patients with suspected or confirmed infectious TB, respiratory protection should be worn by HCWs to protect the sterile field from the respiratory secretions of HCWs and to protect HCWs from the infectious droplet nuclei generated from the patient. When selecting respiratory protection, do not use valved or positive-pressure respirators, because they do not protect the sterile field. A respirator with a valveless filtering facepiece (e.g., N95 disposable respirator) should be used.
Postoperative recovery of a patient with suspected or confirmed TB disease should be in an AII room in any location where the patient is recovering (118). If an AII or comparable room is not available for surgery or postoperative recovery, air-cleaning technologies (e.g., HEPA filtration and UVGI) can be used to increase the number of equivalent ACH (see Environmental Controls); however, the infection-control committee should be involved in the selection and placement of these supplemental controls.
Laboratories
Staff who work in laboratories that handle clinical specimens encounter risks not typically present in other areas of a health-care setting (153–155). Laboratories that handle TB specimens include 1) pass-through facilities that forward specimens to reference laboratories for analysis; 2) diagnostic laboratories that process specimens and perform acid-fast staining and primary culture for M. tuberculosis; and 3) facilities that perform extensive identification, subtyping, and susceptibility studies.
Procedures involving the manipulation of specimens or cultures containing M. tuberculosis introduce additional substantial risks that must be addressed in an effective TB infection-control program. Personnel who work with mycobacteriology specimens should be thoroughly trained in methods that minimize the production of aerosols and undergo periodic competency testing to include direct observation of their work practices. Risks for transmission of M. tuberculosis in laboratories include aerosol formation during any specimen or isolate manipulation and percutaneous inoculation from accidental exposures. Biosafety recommendations for laboratories performing diagnostic testing for TB have been published (74,75,138,156,157).
In laboratories affiliated with a health-care setting (e.g., a hospital) and in free-standing laboratories, the laboratory director, in collaboration with the infection-control staff for the setting, and in consultation with the state TB laboratory, should develop a risk-based infection-control plan for the laboratory that minimizes the risk for exposure to M. tuberculosis. Consider factors including 1) incidence of TB disease (including drug-resistant TB) in the community and in patients served by settings that submit specimens to the laboratory, 2) design of the laboratory, 3) level of TB diagnostic service offered, 4) number of specimens processed, and 5) whether or not aerosol-generating or aerosol-producing procedures are performed and the frequency at which they are performed. Referral laboratories should store isolates in case additional testing is necessary.
Biosafety level (BSL)-2 practices and procedures, containment equipment, and facilities are required for nonaerosol-producing manipulations of clinical specimens (e.g., preparing direct smears for acid-fast staining when done in conjunction with training and periodic checking of competency) (138). All specimens suspected of containing M. tuberculosis (including specimens processed for other microorganisms) should be handled in a Class I or II biological safety cabinet (BSC) (158,159). Conduct all aerosol-generating activities (e.g., inoculating culture media, setting up biochemical and antimicrobic susceptibility tests, opening centrifuge cups, and performing sonication) in a Class I or II BSC (158).
For laboratories that are considered at least medium risk (Appendix C), conduct testing for M. tuberculosis infection at least annually among laboratorians who perform TB diagnostics or manipulate specimens from which M. tuberculosis is commonly isolated (e.g., sputum, lower respiratory secretions, or tissues) (Appendix D). More frequent testing for M. tuberculosis is recommended in the event of a documented conversion among laboratory staff or a laboratory accident that poses a risk for exposure to M. tuberculosis (e.g., malfunction of a centrifuge leading to aerosolization of a sample).
Based on the risk assessment for the laboratory, employees should use personal protective equipment (including respiratory protection) recommended by local regulations for each activity. For activities that have a low risk for generating aerosols, standard personal protective equipment consists of protective laboratory coats, gowns, or smocks designed specifically for use in the laboratory. Protective garments should be left in the laboratory before going to nonlaboratory areas.
For all laboratory procedures, disposable gloves should be worn. Gloves should be disposed of when work is completed, the gloves are overtly contaminated, or the integrity of the glove is compromised. Local or state regulations should determine procedures for the disposal of gloves. Face protection (e.g., goggles, full-facepiece respirator, face shield, or other splatter guard) should also be used when manipulating specimens inside or outside a BSC. Use respiratory protection when performing procedures that can result in aerosolization outside a BSC. The minimum level of respiratory protection is an N95 filtering facepiece respirator. Laboratory workers who use respiratory protection should be provided with the same training on respirator use and care and the same fit testing as other HCWs.
After documented laboratory accidents, conduct an investigation of exposed laboratory workers. Laboratories in which specimens for mycobacteriologic studies (e.g., AFB smears and cultures) are processed should follow the AIA and CDC/National Institute of Health guidelines (118,159) (see Environmental Controls). BSL-3 practices, containment equipment, and facilities are recommended for the propagation and manipulation of cultures of M. tuberculosis complex (including M. bovis) and for animal studies in which primates that are experimentally or naturally infected with M. tuberculosis or M. bovis are used. Animal studies in which guinea pigs or mice are used can be conducted at animal BSL-2. Aerosol infection methods are recommended to be conducted at BSL-3 (159).
Bronchoscopy Suites
Because bronchoscopy is a cough-inducing procedure that might be performed on patients with suspected or confirmed TB disease, bronchoscopy suites require special attention (29,81,160,161). Bronchoscopy can result in the transmission of M. tuberculosis either through the airborne route (29,63,81,86,162) or a contaminated bronchoscope (80,82,163–170). Closed and effectively filtered ventilatory circuitry and minimizing opening of such circuitry in intubated and mechanically ventilated patients might minimize exposure (see Intensive Care Units) (149).
If possible, avoid bronchoscopy on patients with suspected or confirmed TB disease or postpone the procedure until the patient is determined to be noninfectious, by confirmation of the three negative AFB sputum smear results (109–112). When collection of spontaneous sputum specimen is not adequate or possible, sputum induction has been demonstrated to be equivalent to bronchoscopy for obtaining specimens for culture (110). Bronchoscopy might have the advantage of confirmation of the diagnosis with histologic specimens, collection of additional specimens, including post bronchoscopy sputum that might increase the diagnostic yield, and the opportunity to confirm an alternate diagnosis. If the diagnosis of TB disease is suspected, consideration should be given to empiric antituberculosis treatment.
A physical examination should be performed, and a chest radiograph, microscopic examination, culture, and NAA testing of sputum or other relevant specimens should also be obtained, including gastric aspirates (125), as indicated (53,126,131,130). Because 15%–20% of patients with TB disease have negative TST results, a negative TST result is of limited value in the evaluation of the patient with suspected TB disease, particularly in patients from high TB incidence groups in whom TST positive rates exceed 30% (31).
Whenever feasible, perform bronchoscopy in a room that meets the ventilation requirements for an AII room (same as the AIA guidelines parameters for bronchoscopy rooms) (see Environmental Controls). Air-cleaning technologies (e.g., HEPA filtration and UVGI) can be used to increase equivalent ACH.
If sputum specimens must be obtained and the patient cannot produce sputum, consider sputum induction before bronchoscopy (111). In a patient who is intubated and mechanically ventilated, minimize the opening of circuitry. At least N95 respirators should be worn by HCWs while present during a bronchoscopy procedure on a patient with suspected or confirmed infectious TB disease. Because of the increased risk for M. tuberculosis transmission during the performance of bronchoscopy procedures on patients with TB disease, consider using a higher level of respiratory protection than an N95 disposable respirator (e.g., an elastomeric full-facepiece respirator or a powered air-purifying respirator [PAPR] [29]) (see Respiratory Protection).
After bronchoscopy is performed on a patient with suspected or confirmed infectious TB disease, allow adequate time to elapse to ensure removal of M. tuberculosis–contaminated room air before performing another procedure in the same room (Tables 1 and
2). During the period after bronchoscopy when the patient is still coughing, collect at least one sputum for AFB to increase the yield of the procedure. Patients with suspected or confirmed TB disease who are undergoing bronchoscopy should be kept in an AII room until coughing subsides.
Sputum Induction and Inhalation Therapy Rooms
Sputum induction and inhalation therapy induces coughing, which increases the potential for transmission of M. tuberculosis (87,88,90). Therefore, appropriate precautions should be taken when working with patients with suspected or confirmed TB disease. Sputum induction procedures for persons with suspected or confirmed TB disease should be considered after determination that self-produced sputum collection is inadequate and that the AFB smear result on other specimens collected is negative. HCWs who order or perform sputum induction or inhalation therapy in an environment without proper controls for the purpose of diagnosing conditions other than TB disease should assess the patient's risk for TB disease.
Cough-inducing or aerosol-generating procedures in patients with diagnosed TB should be conducted only after an assessment of infectiousness has been considered for each patient and should be conducted in an environment with proper controls. Sputum induction should be performed by using local exhaust ventilation (e.g., booths with special ventilation) or alternatively in a room that meets or exceeds the requirements of an AII room (see Environmental Controls) (90). At least an N95 disposable respirator should be worn by HCWs performing sputum inductions or inhalation therapy on a patient with suspected or confirmed infectious TB disease. Based on the risk assessment, consideration should be given to using a higher level of respiratory protection (e.g., an elastomeric full-facepiece respirator or a PAPR) (see Respiratory Protection) (90).
After sputum induction or inhalation therapy is performed on a patient with suspected or confirmed infectious TB disease, allow adequate time to elapse to ensure removal of M. tuberculosis–contaminated room air before performing another procedure in the same room (Tables 1 and
2). Patients with suspected or confirmed TB disease who are undergoing sputum induction or inhalation therapy should be kept in an AII room until coughing subsides.
Autopsy Suites
Autopsies performed on bodies with suspected or confirmed TB disease can pose a high risk for transmission of M. tuberculosis, particularly during the performance of aerosol-generating procedures (e.g., median sternotomy). Persons who handle bodies might be at risk for transmission of M. tuberculosis (77,78,171–177). Because certain procedures performed as part of an autopsy might generate infectious aerosols, special airborne precautions are required.
Autopsies should not be performed on bodies with suspected or confirmed TB disease without adequate protection for those performing the autopsy procedures. Settings in which autopsies are performed should meet or exceed the requirements of an AII room, if possible (see Environmental Controls), and the drawing in the American Conference of Governmental Industrial Hygienists(r) (ACGIH) Industrial Ventilation Manual VS-99-07 (178). Air should be exhausted to the outside of the building. Air-cleaning technologies (e.g., HEPA filtration or UVGI) can be used to increase the number of equivalent ACH (see Environmental Controls).
As an added administrative measure, when performing autopsies on bodies with suspected or confirmed TB disease, coordination between attending physicians and pathologists is needed to ensure proper infection control and specimen collection. The use of local exhaust ventilation should be considered to reduce exposures to infectious aerosols (e.g., when using a saw, including Striker saw). For HCWs performing an autopsy on a body with suspected or confirmed TB disease, at least N95 disposable respirators should be worn (see Respiratory Protection). Based on the risk assessment, consider using a higher level of respiratory protection than an N95 disposable respirator (e.g., an elastomeric full-facepiece respirator or a PAPR) (see Respiratory Protection).
After an autopsy is performed on a body with suspected or confirmed TB disease, allow adequate time to elapse to ensure removal of M. tuberculosis–contaminated room air before performing another procedure in the same room (Tables 1 and
2). If time delay is not feasible, the autopsy staff should continue to wear respirators while they are in the room.
Embalming Rooms
Tissue or organ removal in an embalming room performed on bodies with suspected or confirmed TB disease can pose a high risk for transmission of M. tuberculosis, particularly during the performance of aerosol-generating procedures. Persons who handle corpses might be at risk for transmission of M. tuberculosis (77,78,171–176). Because certain procedures performed as part of embalming might generate infectious aerosols, special airborne precautions are required.
Embalming involving tissue or organ removal should not be performed on bodies with suspected or confirmed TB disease without adequate protection for the persons performing the procedures. Settings in which these procedures are performed should meet or exceed the requirements of an AII room, if possible (see Environmental Controls), and the drawing in the ACGIH Industrial Ventilation Manual VS-99-07 (178). Air should be exhausted to the outside of the building. Air-cleaning technologies (e.g., HEPA filtration or UVGI) can be used to increase the number of equivalent ACH (see Environmental Controls). The use of local exhaust ventilation should be considered to reduce exposures to infectious aerosols (e.g., when using a saw, including Striker saw) and vapors from embalming fluids.
When HCWs remove tissues or organs from a body with suspected or confirmed TB disease, at least N95 disposable respirators should be worn (see Respiratory Protection). Based on the risk assessment, consider using a higher level of respiratory protection than an N95 disposable respirator (e.g., an elastomeric full-facepiece respirator or a PAPR) (see Respiratory Protection).
After tissue or organ removal is performed on a body with suspected or confirmed TB disease, allow adequate time to elapse to ensure removal of M. tuberculosis–contaminated room air before performing another procedure in the same room (see Environmental Controls). If time delay is not feasible, the staff should continue to wear respirators while in the room.
Outpatient Settings
Outpatient settings might include TB treatment facilities, dental-care settings, medical offices, ambulatory-care settings, and dialysis units. Environmental controls should be implemented based on the types of activities that are performed in the setting.
TB Treatment Facilities
TB treatment facilities might include TB clinics, infectious disease clinics, or pulmonary clinics. TB clinics and other settings in which patients with TB disease and LTBI are examined on a regular basis require special attention. The same principles of triage used in EDs and ambulatory-care settings (see Minimum Requirements) should be applied to TB treatment facilities. These principles include prompt identification, evaluation, and airborne precautions of patients with suspected or confirmed infectious TB disease.
All TB clinic staff, including outreach workers, should be screened for M. tuberculosis infection (Appendix C). Patients with suspected or confirmed infectious TB disease should be physically separated from all patients, but especially from those with HIV infection and other immunocompromising conditions that increase the likelihood of development of TB disease if infected. Immunosuppressed patients with suspected or confirmed infectious TB disease need to be physically separated from others to protect both the patient and others. Appointments should be scheduled to avoid exposing HIV-infected or otherwise severely immunocompromised persons to M. tuberculosis. Certain times of the day should be designated for appointments for patients with infectious TB disease or treat them in areas in which immunocompromised persons are not treated.
Persons with suspected or confirmed infectious TB disease should be promptly placed in an AII room to minimize exposure in the waiting room and other areas of the clinic, and they should be instructed to observe strict respiratory hygiene and cough etiquette procedures. Clinics that provide care for patients with suspected or confirmed infectious TB disease should have at least one AII room. The need for additional AII rooms should be based on the risk assessment for the setting.
All cough-inducing and aerosol-generating procedures should be performed using environmental controls (e.g., in a booth or an AII room) (see Environmental Controls). Patients should be left in the booth or AII room until coughing subsides. Another patient or HCW should not be allowed to enter the booth or AII room until sufficient time has elapsed for adequate removal of M. tuberculosis-contaminated air (see Environmental Controls). A respiratory-protection program should be implemented for all HCWs who work in the TB clinic and who enter AII rooms, visit areas in which persons with suspected or confirmed TB disease are located, or transport patients with suspected or confirmed TB disease in vehicles. When persons with suspected or confirmed infectious TB disease are in the TB clinic and not in an AII room, they should wear a surgical or procedure mask, if possible.
Medical Offices and Ambulatory-Care Settings
The symptoms of TB disease are usually symptoms for which patients might seek treatment in a medical office. Therefore, infectious TB disease could possibly be encountered in certain medical offices and ambulatory-care settings.
Because of the potential for M. tuberculosis transmission in medical offices and ambulatory-care settings, follow the general recommendations for management of patients with suspected or confirmed TB disease and the specific recommendations for EDs (see Intensive Care Units [ICUs]). The risk assessment may be used to determine the need for or selection of environmental controls and the frequency of testing HCWs for M. tuberculosis infection.
Dialysis Units
Certain patients with TB disease need chronic dialysis for treatment of ESRD (179–181). The incidence of TB disease and infection in patients with ESRD might be higher than in the general population (181–183) and might be compounded by the overlapping risks for ESRD and TB disease among patients with diabetes mellitus (39). In addition, certain dialysis patients or patients who are otherwise immunocompromised (e.g., patients with organ transplants) might be on immunosuppressive medications (162,183). Patients with ESRD who need chronic dialysis should have at least one test for M. tuberculosis infection to determine the need for treatment of LTBI. Annual re-screening is indicated if ongoing exposure of ESRD patients to M. tuberculosis is probable.
Hemodialysis procedures should be performed on hospitalized patients with suspected or confirmed TB disease in an AII room. Dialysis staff should use recommended respiratory protection, at least an N95 disposable respirator. Patients with suspected or confirmed TB disease who need chronic hemodialysis might need referral to a hospital or other setting with the ability to perform dialysis procedures in an AII room until the patient is no longer infectious or another diagnosis is made. Certain antituberculosis medications are prescribed differently for hemodialysis patients (31).
Dental-Care Settings
The generation of droplet nuclei containing M. tuberculosis as a result of dental procedures has not been demonstrated (184). Nonetheless, oral manipulations during dental procedures could stimulate coughing and dispersal of infectious particles. Patients and dental HCWs share the same air space for varying periods, which contributes to the potential for transmission of M. tuberculosis in dental settings (185). For example, during primarily routine dental procedures in a dental setting, MDR TB might have been transmitted between two dental workers (186).
To prevent the transmission of M. tuberculosis in dental-care settings, certain recommendations should be followed (187,188). Infection-control policies for each dental health-care setting should be developed, based on the community TB risk assessment (Appendix B), and should be reviewed annually, if possible. The policies should include appropriate screening for LTBI and TB disease for dental HCWs, education on the risk for transmission to the dental HCWs, and provisions for detection and management of patients who have suspected or confirmed TB disease.
When taking a patient's initial medical history and at periodic updates, dental HCWs should routinely document whether the patient has symptoms or signs of TB disease. If urgent dental care must be provided for a patient who has suspected or confirmed infectious TB disease, dental care should be provided in a setting that meets the requirements for an AII room (see Environmental Controls). Respiratory protection (at least N95 disposable respirator) should be used while performing procedures on such patients.
In dental health-care settings that routinely provide care to populations at high risk for TB disease, using engineering controls (e.g., portable HEPA units) similar to those used in waiting rooms or clinic areas of health-care settings with a comparable community-risk profile might be beneficial.
During clinical assessment and evaluation, a patient with suspected or confirmed TB disease should be instructed to observe strict respiratory hygiene and cough etiquette procedures (122). The patient should also wear a surgical or procedure mask, if possible. Non-urgent dental treatment should be postponed, and these patients should be promptly referred to an appropriate medical setting for evaluation of possible infectiousness. In addition, these patients should be kept in the dental health-care setting no longer than required to arrange a referral.
Nontraditional Facility-Based Settings
Nontraditional facility-based settings include EMS, medical settings in correctional facilities, home-based health-care and outreach settings, long-term–care settings (e.g., hospices and skilled nursing facilities), and homeless shelters. Environmental controls should be implemented based on the types of activities that are performed in the setting.
TB is more common in the homeless population than in the general population (189–192). Because persons who visit homeless shelters frequently share exposure and risk characteristics of TB patients who are treated in outpatient clinics, homeless shelters with clinics should observe the same TB infection-control measures as outpatient clinics. ACET has developed recommendations to assist health-care providers, health departments, shelter operators and workers, social service agencies, and homeless persons to prevent and control TB in this population (189).
Emergency Medical Services (EMS)
Although the overall risk is low (193), documented transmission of M. tuberculosis has occurred in EMS occupational settings (194), and approaches to reduce this risk have been described (193,195). EMS personnel should be included in a comprehensive screening program to test for M. tuberculosis infection and provide baseline screening and follow-up testing as indicated by the risk classification of the setting. Persons with suspected or confirmed infectious TB disease who are transported in an ambulance should wear a surgical or procedure mask, if possible, and drivers, HCWs, and other staff who are transporting the patient might consider wearing an N95 respirator.
The ambulance ventilation system should be operated in the nonrecirculating mode, and the maximum amount of outdoor air should be provided to facilitate dilution. If the vehicle has a rear exhaust fan, use this fan during transport. If the vehicle is equipped with a supplemental recirculating ventilation unit that passes air through HEPA filters before returning it to the vehicle, use this unit to increase the number of ACH (188). Air should flow from the cab (front of vehicle), over the patient, and out the rear exhaust fan. If an ambulance is not used, the ventilation system for the vehicle should bring in as much outdoor air as possible, and the system should be set to nonrecirculating. If possible, physically isolate the cab from the rest of the vehicle, and place the patient in the rear seat (194).
EMS personnel should be included in the follow-up contact investigations of patients with infectious TB disease. The Ryan White Comprehensive AIDS Resource Emergency Act of 1990 (Public law 101–381) mandates notification of EMS personnel after they have been exposed to a patient with suspected or confirmed infectious TB disease (Title 42 U.S. Code 1994) (http://hab.hrsa.gov/data2/adap/introduction.htm).
Medical Settings in Correctional Facilities
TB is a substantial health concern in correctional facilities; employees and inmates are at high risk (105,196–205). TB outbreaks in correctional facilities can lead to transmission in surrounding communities (201,206,207). ACET recommends that all correctional facilities have a written TB infection-control plan (196), and multiple studies indicate that screening correctional employees and inmates is a vital TB control measure (204,208,209).
The higher risk for M. tuberculosis transmission in health-care settings in correctional facilities (including jails and prisons) is a result of the disproportionate number of inmates with risk factors for TB infection and TB disease (203,210). Compared with the general population, TB prevalence is higher among inmates and is associated with a higher prevalence of HIV infection (197), increased illicit substance use, lower socioeconomic status (201), and their presence in settings that are at high risk for transmission of M. tuberculosis.
A TB infection-control plan should be developed specifically for that setting, even if the institution is part of a multifacility system (196,211). Medical settings in correctional facilities should be classified as at least medium risk; therefore, all correctional facility health-care personnel and other staff, including correctional officers should be screened for TB at least annually (201,203,208).
Correctional facilities should collaborate with the local or state health department to decide on TB contact investigations and discharge planning (105,212) and to provide TB training and education to inmates and employees (196). Corrections staff should be educated regarding symptoms and signs of TB disease and encouraged to facilitate prompt evaluation of inmates with suspected infectious TB disease (206).
At least one AII room should be available in correctional facilities. Any inmate with suspected or confirmed infectious TB disease should be placed in an AII room immediately or transferred to a setting with an AII room; base the number of additional AII rooms needed on the risk assessment for the setting. Sputum samples should be collected in sputum induction booths or AII rooms, not in inmates' cells. Sputum collection can also be performed safely outside, away from other persons, windows, and ventilation intakes.
Inmates with suspected or confirmed infectious TB disease who must be transported outside an AII room for medically essential procedures should wear a surgical or procedure mask during transport, if possible. If risk assessment indicates the need for respiratory protection, drivers, medical or security staff, and others who are transporting patients with suspected or confirmed infectious TB disease in an enclosed vehicle should consider wearing an N95 disposable respirator.
A respiratory-protection program, including training, education, and fit-testing in the correctional facility's TB infection-control program should be implemented. Correctional facilities should maintain a tracking system for inmate TB screening and treatment and establish a mechanism for sharing this information with state and local health departments and other correctional facilities (196,201). Confidentiality of inmates should be ensured during screening for symptoms or signs of TB disease and risk factors.
Home-Based Health-Care and Outreach Settings
Transmission of M. tuberculosis has been documented in staff who work in home-based health-care and outreach settings (213,214). The setting's infection-control plan should include training that reminds HCWs who provide medical services in the homes of patients or other outreach settings of the importance of early evaluation of symptoms or signs of TB disease for early detection and treatment of TB disease. Training should also include the role of the HCW in educating patients regarding the importance of reporting symptoms or signs of TB disease and the importance of reporting any adverse effects to treatment for LTBI or TB disease.
HCWs who provide medical services in the homes of patients with suspected or confirmed TB disease can help prevent transmission of M. tuberculosis by 1) educating patients and other household members regarding the importance of taking medications as prescribed, 2) facilitating medical evaluation of symptoms or signs of TB disease, and 3) administering DOT, including DOT for treatment of LTBI whenever feasible.
HCWs who provide medical services in the homes of patients should not perform cough-inducing or aerosol-generating procedures on patients with suspected or confirmed infectious TB disease, because recommended infection controls probably will not be in place. Sputum collection should be performed outdoors, away from other persons, windows, and ventilation intakes.
HCWs who provide medical services in the homes of patients with suspected or confirmed infectious TB disease should instruct TB patients to observe strict respiratory hygiene and cough etiquette procedures. HCWs who enter homes of persons with suspected or confirmed infectious TB disease or who transport such persons in an enclosed vehicle should consider wearing at least an N95 disposable respirator (see Respiratory Protection).
Long-Term–Care Facilities (LTCFs)
TB poses a health risk to patients, HCWs, visitors, and volunteers in LTCFs (e.g., hospices and skilled nursing facilities) (215,216). Transmission of M. tuberculosis has occurred in LTCF (217–220), and pulmonary TB disease has been documented in HIV-infected patients and other immunocompromised persons residing in hospices (218,221,222). New employees and residents to these settings should receive a symptom screen and possibly a test for M. tuberculosis infection (see TB Risk Assessment Worksheet).
LTCFs must have adequate administrative and environmental controls, including airborne precautions capabilities and a respiratory-protection program, if they accept patients with suspected or confirmed infectious TB disease. The setting should have 1) a written protocol for the early identification of patients with symptoms or signs of TB disease and 2) procedures for referring these patients to a setting where they can be evaluated and managed. Patients with suspected or confirmed infectious TB disease should not stay in LTCFs unless adequate administrative and environmental controls and a respiratory-protection program are in place. Persons with TB disease who are determined to be noninfectious can remain in the LTCF and do not need to be in an AII room.
Training and Educating HCWs
HCW training and education regarding infection with M. tuberculosis and TB disease is an essential part of administrative controls in a TB surveillance or infection-control program. Training physicians and nurse managers is especially essential because of the leadership role they frequently fulfill in infection control. HCW training and education can increase adherence to TB infection-control measures. Training and education should emphasize the increased risks posed by an undiagnosed person with TB disease in a health-care setting and the specific measures to reduce this risk. HCWs receive various types of training; therefore, combining training for TB infection control with other related trainings might be preferable.
Initial TB Training and Education
The setting should document that all HCWs, including physicians, have received initial TB training relevant to their work setting and additional occupation-specific education. The level and detail of baseline training will vary according to the responsibilities of the HCW and the risk classification of the setting.
Educational materials on TB training are available from various sources at no cost in printed copy, on videotape (223), on compact discs, and the Internet. The local or state health department should have access to additional materials and resources and might be able to help develop a setting-specific TB education program. Suggested components of a baseline TB training program for HCWs have been described previously. CDC's TB website provides information regarding training and education materials (http://www.cdc.gov/tb). Additional training and education materials are available on CDC's TB Education and Training Resources website (http://www.findtbresources.org) and on other TB-related websites and resources (Appendix E).
Physicians, trainees, students, and other HCWs who work in a health-care setting but do not receive payment from that setting should receive baseline training in TB infection-control policies and practices, the TB screening program, and procedures for reporting an M. tuberculosis infection test conversion or diagnosis of TB disease. Initial TB training should be provided before the HCW starts working.
Follow-Up TB Training and Education
All settings should conduct an annual evaluation of the need for follow-up training and education for HCWs based on the number of untrained and new HCWs, changes in the organization and services of the setting, and availability of new TB infection-control information.
If a potential or known exposure to M. tuberculosis occurs in the setting, prevention and control measures should include retraining HCWs in the infection-control procedures established to prevent the recurrence of exposure. If a potential or known exposure results in a newly recognized positive TST or BAMT result, test conversion, or diagnosis of TB disease, education should include information on 1) transmission of M. tuberculosis, 2) noninfectiousness of HCWs with LTBI, and 3) potential infectiousness of HCWs with TB disease.
OSHA requires annual respiratory-protection training for HCWs who use respiratory devices (see Respiratory Protection). HCWs in settings with a classification of potential ongoing transmission should receive additional training and education on 1) symptoms and signs of TB disease, 2) M. tuberculosis transmission, 3) infection-control policies, 4) importance of TB screening for HCWs, and 5) responsibilities of employers and employees regarding M. tuberculosis infection test conversion and diagnosis of TB disease.
TB Infection-Control Surveillance
HCW Screening Programs for TB Support Surveillance and Clinical Care
TB screening programs provide critical information for caring for individual HCWs and information that facilitates detection of M. tuberculosis transmission. The screening program consists of four major components: 1) baseline testing for M. tuberculosis infection, 2) serial testing for M. tuberculosis infection, 3) serial screening for symptoms or signs of TB disease, and 4) TB training and education.
Surveillance data from HCWs can protect both HCWs and patients. Screening can prevent future transmission by identifying lapses in infection control and expediting treatment for persons with LTBI or TB disease. Tests to screen for M. tuberculosis infection should be administered, interpreted, and recorded according to procedures in this report (see Supplement, Diagnostic Procedures for LTBI and TB Disease). Protection of privacy and maintenance of confidentiality of HCW test results should be ensured. Methods to screen for infection with M. tuberculosis are available (30,31,39).
Baseline Testing for M. tuberculosis Infection
Baseline testing for M. tuberculosis infection is recommended for all newly hired HCWs, regardless of the risk classification of the setting and can be conducted with the TST or BAMT. Baseline testing is also recommended for persons who will receive serial TB screening (e.g., residents or staff of correctional facilities or LTCFs) (39,224). Certain settings, with the support of the infection-control committee, might choose not to perform baseline or serial TB screening for HCWs who will never be in contact with or have shared air space with patients who have TB disease (e.g., telephone operators who work in a separate building from patients) or who will never be in contact with clinical specimens that might contain M. tuberculosis.
Baseline test results 1) provide a basis for comparison in the event of a potential or known exposure to M. tuberculosis and 2) facilitate the detection and treatment of LTBI or TB disease in an HCW before employment begins and reduces the risk to patients and other HCWs. If TST is used for baseline testing, two-step testing is recommended for HCWs whose initial TST results are negative (39,224). If the first-step TST result is negative, the second-step TST should be administered 1–3 weeks after the first TST result was read. If either 1) the baseline first-step TST result is positive or 2) the first-step TST result is negative but the second-step TST result is positive, TB disease should be excluded, and if it is excluded, then the HCW should be evaluated for treatment of LTBI. If the first and second-step TST results are both negative, the person is classified as not infected with M. tuberculosis.
If the second test result of a two-step TST is not read within 48–72 hours, administer a TST as soon as possible (even if several months have elapsed) and ensure that the result is read within 48–72 hours (39). Certain studies indicate that positive TST reactions might still be measurable from 4–7 days after testing (225,226). However, if a patient fails to return within 72 hours and has a negative test result, the TST should be repeated (42).
A positive result to the second step of a baseline two-step TST is probably caused by boosting as opposed to recent infection with M. tuberculosis. These responses might result from remote infections with M. tuberculosis, infection with an NTM (also known as MOTT), or previous BCG vaccination. Two-step testing will minimize the possibility that boosting will lead to an unwarranted suspicion of transmission of M. tuberculosis with subsequent testing. A second TST is not needed if the HCW has a documented TST result from any time during the previous 12 months (see Baseline Testing for M. tuberculosis Infection After TST Within the Previous 12 Months).
A positive TST reaction as a result of BCG wanes after 5 years. Therefore, HCWs with previous BCG vaccination will frequently have a negative TST result (74,227–232). Because HCWs with a history of BCG are frequently from high TB-prevalence countries, positive test results for M. tuberculosis infection in HCWs with previous BCG vaccination should be interpreted as representing infection with M. tuberculosis (74,227–233). Although BCG reduces the occurrence of severe forms of TB disease in children and overall might reduce the risk for progression from LTBI to TB disease (234,235), BCG is not thought to prevent M. tuberculosis infection (236). Test results for M. tuberculosis infection for HCWs with a history of BCG should be interpreted by using the same diagnostic cut points used for HCWs without a history of BCG vaccination.
BAMT does not require two-step testing and is more specific than skin testing. BAMT that uses M. tuberculosis-specific antigens (e.g., QFT-G) are not expected to result in false-positive results in persons vaccinated with BCG. Baseline test results should be documented, preferably within 10 days of HCWs starting employment.
Baseline Testing for M. tuberculosis Infection After TST Within the Previous 12 Months
A second TST is not needed if the HCW has a documented TST result from any time during the previous 12 months. If a newly employed HCW has had a documented negative TST result within the previous 12 months, a single TST can be administered in the new setting (Box 1). This additional TST represents the second stage of two-step testing. The second test decreases the possibility that boosting on later testing will lead to incorrect suspicion of transmission of M. tuberculosis in the setting.
A recent TST (performed in ≤12 months) is not a contraindication to a subsequent TST unless the test was associated with severe ulceration or anaphylactic shock, which are substantially rare adverse events (30,237–239). Multiple TSTs are safe and do not increase the risk for a false-positive result or a TST conversion in persons without infection with mycobacteria (39).
Baseline Documentation of a History of TB Disease, a Previously Positive Test Result for M. tuberculosis Infection, or Completion of Treatment for LTBI or TB Disease
Additional tests for M. tuberculosis infection do not need to be performed for HCWs with a documented history of TB disease, documented previously positive test result for M. tuberculosis infection, or documented completion of treatment for LTBI or TB disease. Documentation of a previously positive test result for M. tuberculosis infection can be substituted for a baseline test result if the documentation includes a recorded TST result in millimeters (or BAMT result), including the concentration of cytokine measured (e.g., IFN-γ). All other HCWs should undergo baseline testing for M. tuberculosis infection to ensure that the test result on record in the setting has been performed and measured using the recommended diagnostic the recommended procedures (see Supplement, Diagnostic Procedures for LTBI and TB Disease).
A recent TST (performed in ≤12 months) is not a contraindication to the administration of an additional test unless the TST was associated with severe ulceration or anaphylactic shock, which are substantially rare adverse events (30,237,238). However, the recent test might complicate interpretation of subsequent test results because of the possibility of boosting.
Serial Follow-Up of TB Screening and Testing for M. tuberculosis Infection
The need for serial follow-up screening for groups of HCWs with negative test results for M. tuberculosis infection is an institutional decision that is based on the setting's risk classification. This decision and changes over time based on updated risk assessments should be official and documented. If a serial follow-up screening program is required, the risk assessment for the setting (Appendix B) will determine which HCWs should be included in the program and the frequency of screening. Two-step TST testing should not be performed for follow-up testing.
If possible, stagger follow-up screening (rather than testing all HCWs at the same time each year) so that all HCWs who work in the same area or profession are not tested in the same month. Staggered screening of HCWs (e.g., on the anniversary of their employment or on their birthdays) increases opportunities for early recognition of infection-control problems that can lead to conversions in test results for M. tuberculosis infection. Processing aggregate analysis of TB screening data on a periodic regular basis is important for detecting problems.
HCWs with a Newly Recognized Positive Test Result for M. tuberculosis Infection or Symptoms or Signs of TB Disease
Clinical Evaluation
Any HCW with a newly recognized positive test result for M. tuberculosis infection, test conversion, or symptoms or signs of TB disease should be promptly evaluated. The evaluation should be arranged with employee health, the local or state health department, or a personal physician. Any physicians who evaluate HCWs with suspected TB disease should be familiar with current diagnostic and therapeutic guidelines for LTBI and TB disease (31,39).
The definitions for positive test results for M. tuberculosis infection and test conversion in HCWs are included in this report (see Supplement, Diagnostic Procedures for LTBI and TB Disease). Symptoms of disease in the lung, pleura, or airways, and the larynx include coughing for ≥3 weeks, loss of appetite, unexplained weight loss, night sweats, bloody sputum or hemoptysis, hoarseness, fever, fatigue, or chest pain. The evaluation should include a clinical examination and symptom screen (a procedure used during a clinical evaluation in which patients are asked if they have experienced any symptoms or signs of TB disease), chest radiograph, and collection of sputum specimens.
If TB disease is diagnosed, begin antituberculosis treatment immediately, according to published guidelines (31). The diagnosing clinician (who might not be a physician with the institution's infection-control program) should notify the local or state health department in accordance with disease reporting laws, which generally specify a 24-hour time limit.
If TB disease is excluded, offer the HCW treatment for LTBI in accordance with published guidelines (see Supplements, Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease [39,240]). If the HCW has already completed treatment for LTBI and is part of a TB screening program, instead of participating in serial skin testing, the HCW should be monitored for symptoms of TB disease and should receive any available training, which should include information on the symptoms of TB disease and instructing the HCW to report any such symptoms immediately to occupational health. In addition, annual symptom screens should be performed, which can be administered as part of other HCW screening and education efforts. Treatment for LTBI should be offered to HCWs who are eligible (39).
HCWs with a previously negative test result who have an increase of ≥10 mm induration when examined on follow-up testing probably have acquired M. tuberculosis infection and should be evaluated for TB disease. When disease is excluded, HCWs should be treated for LTBI unless medically contraindicated (39,240).
Chest Radiography
HCWs with a baseline positive or newly positive TST or BAMT result should receive one chest radiograph to exclude a diagnosis of TB disease (or an interpretable copy within a reasonable time frame, such as 6 months). After this baseline chest radiograph is performed and the result is documented, repeat radiographs are not needed unless symptoms or signs of TB disease develop or a clinician recommends a repeat chest radiograph (39,116). Instead of participating in serial testing for M. tuberculosis infection, HCWs with a positive test result for M. tuberculosis infection should receive a symptom screen. The frequency of this symptom screen should be determined by the risk classification for the setting.
Serial follow-up chest radiographs are not recommended for HCWs with documentation of a previously positive test result for M. tuberculosis infection, treatment for LTBI or TB disease, or for asymptomatic HCWs with negative test results for M. tuberculosis infection. HCWs who have a previously positive test result for M. tuberculosis infection and who change jobs should carry documentation of a baseline chest radiograph result (and the positive test result for M. tuberculosis infection) to their new employers.
Workplace Restrictions
HCWs with a baseline positive or newly positive test result for M. tuberculosis infection should receive one chest radiograph result to exclude TB disease (or an interpretable copy within a reasonable time frame, such as 6 months).
HCWs with confirmed infectious pulmonary, laryngeal, endobroncheal, or tracheal TB disease, or a draining TB skin lesion pose a risk to patients, HCWs, and others. Such HCWs should be excluded from the workplace and should be allowed to return to work when the following criteria have been met: 1) three consecutive sputum samples (109–112) collected in 8–24-hour intervals that are negative, with at least one sample from an early morning specimen (because respiratory secretions pool overnight); 2) the person has responded to antituberculosis treatment that will probably be effective (can be based on susceptibility results); and 3) the person is determined to be noninfectious by a physician knowledgeable and experienced in managing TB disease (see Supplements, Estimating the Infectiousness of a TB Patient; Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease).
HCWs with extrapulmonary TB disease usually do not need to be excluded from the workplace as long as no involvement of the respiratory track has occurred. They can be confirmed as noninfectious and can continue to work if documented evidence is available that indicates that concurrent pulmonary TB disease has been excluded.
HCWs receiving treatment for LTBI can return to work immediately. HCWs with LTBI who cannot take or do not accept or complete a full course of treatment for LTBI should not be excluded from the workplace. They should be counseled regarding the risk for developing TB disease and instructed to report any TB symptoms immediately to the occupational health unit.
HCWs who have a documented positive TST or BAMT result and who leave employment should be counseled again, if possible, regarding the risk for developing TB disease and instructed to seek prompt evaluation with the local health department or their primary care physician if symptoms of TB disease develop. Consider mailing letters to former HCWs who have LTBI. This information should be recorded in the HCWs' employee health record when they leave employment.
Asymptomatic HCWs with a baseline positive or newly positive TST or BAMT result do not need to be excluded from the workplace. Treatment for LTBI should be considered in accordance with CDC guidelines (39).
Identification of Source Cases and Recording of Drug-Susceptibility Patterns
If an HCW experiences a conversion in a test result for M. tuberculosis infection, evaluate the HCW for a history of suspected or known exposure to M. tuberculosis to determine the potential source. When the source case is identified, also identify the drug susceptibility pattern of the M. tuberculosis isolate from the source. The drug-susceptibility pattern should be recorded in the HCW's medical or employee health record to guide the treatment of LTBI or TB disease, if indicated.
HCWs with Medical Conditions Associated with Increased Risk for Progression to TB Disease
In settings in which HCWs are severely immunocompromised, additional precautions must be taken. HIV infection is the highest risk factor for progression from LTBI to TB disease (22,39,42,49). Other immunocompromising conditions, including diabetes mellitus, certain cancers, and certain drug treatments, also increase the risk for rapid progression from LTBI to TB disease. TB disease can also adversely affect the clinical course of HIV infection and acquired immunodeficiency syndrome (AIDS) and can complicate HIV treatment (31,39,53).
Serial TB screening beyond that indicated by the risk classification for the setting is not indicated for persons with the majority of medical conditions that suppress the immune system or otherwise increase the risk for infection with M. tuberculosis progressing to TB disease (58). However, consideration should be given to repeating the TST for HIV-infected persons whose initial TST result was negative and whose immune function has improved in response to highly active antiretroviral therapy (HAART) (i.e., those whose CD4-T lymphocyte count has increased to >200 cells/mL).
All HCWs should, however, be encouraged during their initial TB training to determine if they have such a medical condition and should be aware that receiving medical treatment can improve cell-mediated immunity. HCWs should be informed concerning the availability of counseling, testing, and referral for HIV (50,51). In addition, HCWs should know whether they are immunocompromised, and they should be aware of the risks from exposure to M. tuberculosis (1). In certain cases, reassignment to areas in which exposure is minimized or nonexistent might be medically advisable or desirable.
Immunocompromised HCWs should have the option of an assignment in an area or activity where the risk for exposure to M. tuberculosis is low. This choice is a personal decision for the immunocompromised HCW (241) (http://www.eeoc.gov/laws/ada.html). Health-care settings should provide education and follow infection-control recommendations (70).
Information provided by HCWs regarding their immune status and request for voluntary work assignments should be treated confidentially, according to written procedures on the confidential handling of such information. All HCWs should be made aware of these procedures at the time of employment and during initial TB training and education.
Problem Evaluation
Contact investigations might be initiated in response to 1) conversions in test results in HCWs for M. tuberculosis infection, 2) diagnosis of TB disease in an HCW, 3) suspected person-to-person transmission of M. tuberculosis, 4) lapses in TB infection-control practices that expose HCWs and patients to M. tuberculosis, or 5) possible TB outbreaks identified using automated laboratory systems (242). In these situations, the objectives of a contact investigation might be to 1) determine the likelihood that transmission of M. tuberculosis has occurred; 2) determine the extent of M. tuberculosis transmission; 3) identify persons who were exposed, and, if possible, the sources of potential transmission; 4) identify factors that could have contributed to transmission, including failure of environmental infection-control measures, failure to follow infection-control procedures, or inadequacy of current measures or procedures; 5) implement recommended interventions; 6) evaluate the effectiveness of the interventions; and 7) ensure that exposure to M. tuberculosis has been terminated and that the conditions leading to exposure have been eliminated.
Earlier recognition of a setting in which M. tuberculosis transmission has occurred could be facilitated through innovative approaches to TB contact investigations (e.g., network analysis and genetic typing of isolates). Network analysis makes use of information (e.g., shared locations within a setting that might not be collected in traditional TB contact investigations) (45). This type of information might be useful during contact investigations involving hospitals or correctional settings to identify any shared wards, hospital rooms, or cells. Genotyping of isolates is universally available in the United States and is a useful adjunct in the investigation of M. tuberculosis transmission (44,89,243,244). Because the situations prompting an investigation are likely to vary, investigations should be tailored to the individual circumstances. Recommendations provide general guidance for conducting contact investigations (34,115).
General Recommendations for Investigating Conversions in Test Results for M. tuberculosis Infection in HCWs
A test conversion might need to be reported to the health department, depending on state and local regulations. Problem evaluation during contact investigations should be accomplished through cooperation between infection-control personnel, occupational health, and the local or state TB-control program. If a test conversion in an HCW is detected as a result of serial screening and the source is not apparent, conduct a source case investigation to determine the probable source and the likelihood that transmission occurred in the health-care setting (115).
Lapses in TB infection control that might have contributed to the transmission of M. tuberculosis should be corrected. Test conversions and TB disease among HCWs should be recorded and reported, according to OSHA requirements (http://www.osha.gov/recordkeeping). Consult Recording and Reporting Occupational Injuries and Illness (OSHA standard 29 Code of Federal Regulations [CFR], 1904) to determine recording and reporting requirements (245).
Investigating Conversions in Test Results for M. tuberculosis Infection in HCWs: Probable Source Outside the Health-Care Setting
If a test conversion in an HCW is detected and exposure outside the health-care setting has been documented by the corresponding local or state health department, terminate the investigation within the health-care setting.
Investigating Conversions in Test Results for M. tuberculosis Infection in HCWs: Known Source in the Health-Care Setting
An investigation of a test conversion should be performed in collaboration with the local or state health department. If a conversion in an HCW is detected and the HCW's history does not document exposure outside the health-care setting but does identify a probable source in the setting, the following steps should be taken: 1) identify and evaluate close contacts of the suspected source case, including other patients and visitors; 2) determine possible reasons for the exposure; 3) implement interventions to correct the lapse(s) in infection control; and 4) immediately screen HCWs and patients if they were close contacts to the source case. For exposed HCWs and patients in a setting that has chosen to screen for infection with M. tuberculosis by using the TST, the following steps should be taken:
administer a symptom screen;
administer a TST to those who had previously negative TST results; baseline two-step TST should not be performed in contact investigations;
repeat the TST and symptom screen 8–10 weeks after the end of exposure, if the initial TST result is negative (33);
administer a symptom screen, if the baseline TST result is positive;
promptly evaluate (including a chest radiograph) the exposed person for TB disease, if the symptom screen or the initial or 8–10-week follow-up TST result is positive; and
conduct additional medical and diagnostic evaluation (which includes a judgment about the extent of exposure) for LTBI, if TB disease is excluded.
If no additional conversions in the test results for M. tuberculosis infection are detected in the follow-up testing, terminate the investigation. If additional conversions in the tests for M. tuberculosis infection are detected in the follow-up testing, transmission might still be occurring, and additional actions are needed: 1) implement a classification of potential ongoing transmission for the specific setting or group of HCWs; 2) the initial cluster of test conversions should be reported promptly to the local or state health department; 3) possible reasons for exposure and transmission should be reassessed and 4) the degree of adherence to the interventions implemented should be evaluated.
Testing for M. tuberculosis infection should be repeated 8–10 weeks after the end of exposure for HCW contacts who previously had negative test results, and the circle of contacts should be expanded to include other persons who might have been exposed. If no additional TST conversions are detected on the second round of follow-up testing, terminate the investigation. If additional TST conversions are detected on the second round of follow-up testing, maintain a classification of potential ongoing transmission and consult the local or state health department or other persons with expertise in TB infection control for assistance.
The classification of potential ongoing transmission should be used as a temporary classification only. This classification warrants immediate investigation and corrective steps. After determination has been made that ongoing transmission has ceased, the setting should be reclassified as medium risk. Maintaining the classification of medium risk for at least 1 year is recommended.
Investigating a Conversion of a Test Result for M. tuberculosis Infection in an HCW with an Unknown Exposure
If a test conversion in an HCW is detected and the HCW's history does not document exposure outside the health-care setting and does not identify a probable source of exposure in the setting, additional investigation to identify a probable source in the health-care setting is warranted.
If no source case is identified, estimate the interval during which the HCW might have been infected. The interval is usually 8–10 weeks before the most recent negative test result through 2 weeks before the first positive test result. Laboratory and infection-control records should be reviewed to identify all patients (and any HCWs) who have had suspected or confirmed infectious TB disease and who might have transmitted M. tuberculosis to the HCW. If the investigation identifies a probable source, identify and evaluate contacts of the suspected source. Close contacts should be the highest priority for screening.
The following steps should be taken in a setting that uses TST or BAMT to screen for M. tuberculosis: 1) administer a symptom screen and the test routinely used in the setting (i.e., TST or BAMT) to persons who previously had negative results; 2) if the initial result is negative, the test and symptom screen should be repeated 8–10 weeks after the end of exposure; 3) if the symptom screen, the first test result, or the 8–10-week follow-up test result is positive, the presumed exposed person should be promptly evaluated for TB disease, including the use of a chest radiograph; and 4) if TB disease is excluded, additional medical and diagnostic evaluation for LTBI is needed, which includes a judgment regarding the extent of exposure (see Investigating Conversions in Test Results for M. tuberculosis Infection in HCWs: Known Source in the Health-Care Setting).
Investigations That Do Not Identify a Probable Source
If serial TB screening is performed in the setting, review the results of screening of other HCWs in the same area of the health-care setting or same occupational group. If serial TB screening is not performed in the setting or if insufficient numbers of recent results are available, conduct additional TB screening of other HCWs in the same area or occupational group. If the review and screening yield no additional test conversions, and no evidence to indicate health-care–associated transmission exists, then the investigation should be terminated.
Whether HCW test conversions resulted from exposure in the setting or elsewhere or whether true infection with M. tuberculosis has even occurred is uncertain. However, the absence of other data implicating health-care–associated transmission suggests that the conversion could have resulted from 1) unrecognized exposure to M. tuberculosis outside the health-care setting; 2) cross reactivity with another antigen (e.g., BCG or nontuberculous mycobacteria); or 3) errors in applying, reading, or interpreting the test result for M. tuberculosis infection. If the review and screening identify additional test conversions, health-care–associated transmission is more probable.
Evaluation of the patient identification process, TB infection-control policies and practices, and environmental controls to identify lapses that could have led to exposure and transmission should be conducted. If no problems are identified, a classification of potential ongoing transmission should be applied, and the local or state health department or other persons with expertise in TB infection control should be consulted for assistance. If problems are identified, implement recommended interventions and repeat testing for M. tuberculosis infection 8–10 weeks after the end of exposure for HCWs with negative test results. If no additional test conversions are detected in the follow-up testing, terminate the investigation.
Conversions in Test Results for M. tuberculosis Infection Detected in Follow-Up Testing
In follow-up testing, a classification of potential ongoing transmission should be maintained. Possible reasons for exposure and transmission should be reassessed, and the appropriateness of and degree of adherence to the interventions implemented should be evaluated. For HCWs with negative test results, repeat testing for M. tuberculosis infection 8–10 weeks after the end of exposure. The local or state health department or other persons with expertise in TB infection control should be consulted.
If no additional conversions are detected during the second round of follow-up testing, terminate the investigation. If additional conversions are detected, continue a classification of potential ongoing transmission and consult the local or state health department or other persons with expertise in TB infection control.
The classification of potential ongoing transmission should be used as a temporary classification only. This classification warrants immediate investigation and corrective steps. After a determination that ongoing transmission has ceased, the setting should be reclassified as medium risk. Maintaining the classification of medium risk for at least 1 year is recommended.
Investigating a Case of TB Disease in an HCW
Occupational health services and other physicians in the setting should have procedures for immediately notifying the local administrators or infection-control personnel if an HCW is diagnosed with TB disease so that a problem evaluation can be initiated. If an HCW is diagnosed with TB disease and does not have a previously documented positive test result for M. tuberculosis infection, conduct an investigation to identify the probable sources and circumstances for transmission (see General Recommendations for Investigating Conversions in Test Results for M. tuberculosis Infection in HCWs). If an HCW is diagnosed with TB disease, regardless of previous test result status, an additional investigation must be conducted to ascertain whether the disease was transmitted from this HCW to others, including other HCWs, patients, and visitors.
The potential infectiousness of the HCW, if potentially infectious, and the probable period of infectiousness (see Contact Investigations) should be determined. For HCWs with suspected or confirmed infectious TB disease, conduct an investigation that includes 1) identification of contacts (e.g., other HCWs, patients, and visitors), 2) evaluation of contacts for LTBI and TB disease, and 3) notification of the local or state health department for consultation and investigation of community contacts who were exposed outside the health-care setting.
M. tuberculosis genotyping should be performed so that the results are promptly available. Genotyping results are useful adjuncts to epidemiologically based public health investigations of contacts and possible source cases (especially in determining the role of laboratory contamination) (89,166,243,246–261). When confidentiality laws prevent the local or state health department from communicating information regarding a patient's identity, health department staff should work with hospital staff and legal counsel, and the HCW to determine how the hospital can be notified without breaching confidentiality.
Investigating Possible Patient-to-Patient Transmission of M. tuberculosis
Information concerning TB cases among patients in the setting should be routinely recorded for risk classification and risk assessment purposes. Documented information by location and date should include results of sputum smear and culture, chest radiograph, drug-susceptibility testing, and adequacy of infection-control measures.
Each time a patient with suspected or confirmed TB disease is encountered in a health-care setting, an assessment of the situation should be made and the focus should be on 1) a determination of infectiousness of the patient, 2) confirmation of compliance with local public health reporting requirements (including the prompt reporting of a person with suspected TB disease as required), and 3) assessment of the adequacy of infection control.
A contact investigation should be initiated in situations where infection control is inadequate and the patient is infectious. Patients with positive AFB sputum smear results are more infectious than patients with negative AFB sputum smear results, but the possibility exists that patients with negative sputum smear results might be infectious (262). Patients with negative AFB sputum smear results but who undergo aerosol-generating or aerosol-producing procedures (including bronchoscopy) without adequate infection-control measures create a potential for exposure. All investigations should be conducted in consultation with the local public health department.
If serial surveillance of these cases reveals one of the following conditions, patient-to-patient transmission might have occurred, and a contact investigation should be initiated:
A high proportion of patients with TB disease were admitted to or examined in the setting during the year preceding onset of their TB disease, especially when TB disease is identified in patients who were otherwise unlikely to be exposed to M. tuberculosis.
An increase occurred in the number of TB patients diagnosed with drug-resistant TB, compared with the previous year.
Isolates from multiple patients had identical and characteristic drug susceptibility or DNA fingerprint patterns.
Surveillance of TB Cases in Patients Indicates Possible Patient-to-Patient Transmission of M. tuberculosis
Health-care settings should collaborate with the local or state health department to conduct an investigation. For settings in which HCWs are serially tested for M. tuberculosis infection, review HCW records to determine whether an increase in the number of conversions in test results for M. tuberculosis infection has occurred. Patient surveillance data and medical records should be reviewed for additional cases of TB disease. Settings should look for possible exposures from previous or current admissions that might have exposed patients with newly diagnosed TB disease to other patients with TB disease, determining if the patients were admitted to the same room or area, or if they received the same procedure or went to the same treatment area on the same day.
If the investigation suggests that transmission has occurred, possible causes of transmission of M. tuberculosis (e.g., delayed diagnosis of TB disease, institutional barriers to implementing timely and correct airborne precautions, and inadequate environmental controls) should be evaluated. Possible exposure to other patients or HCWs should be determined, and if exposure has occurred, these persons should be evaluated for LTBI and TB disease (i.e., test for M. tuberculosis infection and administer a symptom screen).
If the local or state health department was not previously contacted, settings should notify the health department so that a community contact investigation can be initiated, if necessary. The possibility of laboratory errors in diagnosis or the contamination of bronchoscopes (82,169) or other equipment should be considered (136).
Contact Investigations
The primary goal of contact investigations is to identify secondary cases of TB disease and LTBI among contacts so that therapy can be initiated as needed (263–265). Contact investigations should be collaboratively conducted by both infection-control personnel and local TB-control program personnel.
Initiating a Contact Investigation
A contact investigation should be initiated when 1) a person with TB disease has been examined at a health-care setting, and TB disease was not diagnosed and reported quickly, resulting in failure to apply recommended TB infection controls; 2) environmental controls or other infection-control measures have malfunctioned while a person with TB disease was in the setting; or 3) an HCW develops TB disease and exposes other persons in the setting.
As soon as TB disease is diagnosed or a problem is recognized, standard public health practice should be implemented to prioritize the identification of other patients, HCWs, and visitors who might have been exposed to the index case before TB infection-control measures were correctly applied (52). Visitors of these patients might also be contacts or the source case.
The following activities should be implemented in collaboration with or by the local or state health department (34,266): 1) interview the index case and all persons who might have been exposed; 2) review the medical records of the index case; 3) determine the exposure sites (i.e., where the index case lived, worked, visited, or was hospitalized before being placed under airborne precautions); and 4) determine the infectious period of the index case, which is the period during which a person with TB disease is considered contagious and most capable of transmitting M. tuberculosis to others.
For programmatic purposes, for patients with positive AFB sputum smear results, the infectious period can be considered to begin 3 months before the collection date of the first positive AFB sputum smear result or the symptom onset date (whichever is earlier). The end of the infectious period is the date the patient is placed under airborne precautions or the date of collection of the first of consistently negative AFB sputum smear results (whichever is earlier). For patients with negative AFB sputum smear results, the infectious period can begin 1 month before the symptom onset date and end when the patient is placed under airborne precautions.
The exposure period, the time during which a person shared the same air space with a person with TB disease for each contact, should be determined as well as whether transmission occurred from the index patient to persons with whom the index patient had intense contact. In addition, the following should be determined: 1) intensity of the exposure based on proximity, 2) overlap with the infectious period of the index case, 3) duration of exposure, 4) presence or absence of infection-control measures, 5) infectiousness of the index case, 6) performance of procedures that could increase the risk for transmission during contact (e.g., sputum induction, bronchoscopy, and airway suction), and 7) the exposed cohort of contacts for TB screening.
The most intensely exposed HCWs and patients should be screened as soon as possible after exposure to M. tuberculosis has occurred and 8–10 weeks after the end of exposure if the initial TST result is negative. Close contacts should be the highest priority for screening.
For HCWs and patients who are presumed to have been exposed in a setting that screens for infection with M. tuberculosis using the TST, the following activities should be implemented:
performing a symptom screen;
administering a TST to those who previously had negative TST results;
repeating the TST and symptom screen 8–10 weeks after the end of exposure, if the initial TST result is negative;
promptly evaluating the HCW for TB disease, including performing a chest radiograph, if the symptom screen or the initial or 8–10-week follow-up TST result is positive; and
providing additional medical and diagnostic evaluation for LTBI, including determining the extent of exposure, if TB disease is excluded.
For HCWs and patients who are presumed to have been exposed in a setting that screens for infection with M. tuberculosis using the BAMT, the following activities should be implemented (see Supplement, Surveillance and Detection of M. tuberculosis Infections in Health-Care Settings). If the most intensely exposed persons have test conversions or positive test results for M. tuberculosis infection in the absence of a previous history of a positive test result or TB disease, expand the investigation to evaluate persons with whom the index patient had less contact. If the evaluation of the most intensely exposed contacts yields no evidence of transmission, expanding testing to others is not necessary.
Exposed persons with documented previously positive test results for M. tuberculosis infection do not require either repeat testing for M. tuberculosis infection or a chest radiograph (unless they are immunocompromised or otherwise at high risk for TB disease), but they should receive a symptom screen. If the person has symptoms of TB disease, 1) record the symptoms in the HCW's medical chart or employee health record, 2) perform a chest radiograph, 3) perform a full medical evaluation, and 4) obtain sputum samples for smear and culture, if indicated.
The setting should determine the reason(s) that a TB diagnosis or initiation of airborne precautions was delayed or procedures failed, which led to transmission of M. tuberculosis in the setting. Reasons and corrective actions taken should be recorded, including changes in policies, procedures, and TB training and education practices.
Collaboration with the Local or State Health Department
For assistance with the planning and implementation of TB-control activities in the health-care setting and for names of experts to help with policies, procedures, and program evaluation, settings should coordinate with the local or state TB-control program . By law, the local or state health department must be notified when TB disease is suspected or confirmed in a patient or HCW so that follow up can be arranged and a community contact investigation can be conducted. The local or state health department should be notified as early as possible before the patient is discharged to facilitate followup and continuation of therapy by DOT (31). For inpatient settings, coordinate a discharge plan with the patient (including a patient who is an HCW with TB disease) and the TB-control program of the local or state health department.
Environmental Controls
Environmental controls are the second line of defense in the TB infection-control program, after administrative controls. Environmental controls include technologies for the removal or inactivation of airborne M. tuberculosis. These technologies include local exhaust ventilation, general ventilation, HEPA filtration, and UVGI. These controls help to prevent the spread and reduce the concentration of infectious droplet nuclei in the air. A summary of environmental controls and their use in prevention of transmission of M. tuberculosis is provided in this report (see Supplement, Environmental Controls), including detailed information concerning the application of environmental controls.
Local Exhaust Ventilation
Local exhaust ventilation is a source-control technique used for capturing airborne contaminants (e.g., infectious droplet nuclei or other infectious particles) before they are dispersed into the general environment. In local exhaust ventilation methods, external hoods, enclosing booths, and tents are used. Local exhaust ventilation (e.g., enclosed, ventilated booth) should be used for cough-inducing and aerosol-generating procedures. When local exhaust is not feasible, perform cough-inducing and aerosol-generating procedures in a room that meets the requirements for an AII room.
General Ventilation
General ventilation systems dilute and remove contaminated air and control airflow patterns in a room or setting. An engineer or other professional with expertise in ventilation should be included as part of the staff of the health-care setting or hire a consultant with expertise in ventilation engineering specific to health-care settings. Ventilation systems should be designed to meet all applicable federal, state, and local requirements.
A single-pass ventilation system is the preferred choice in areas in which infectious airborne droplet nuclei might be present (e.g., AII rooms). Use HEPA filtration if recirculation of air is necessary.
AII rooms in health-care settings pre-existing 1994 guidelines should have an airflow of ≥6 ACH. When feasible, the airflow should be increased to ≥12 ACH by 1) adjusting or modifying the ventilation system or 2) using air-cleaning methods (e.g., room-air recirculation units containing HEPA filters or UVGI systems that increase the equivalent ACH). New construction or renovation of health-care settings should be designed so that AII rooms achieve an airflow of ≥12 ACH. Ventilation rates for other areas in health-care settings should meet certain specifications (see Risk Classification Examples). If a variable air volume (VAV) ventilation system is used in an AII room, design the system to maintain the room under negative pressure at all times. The VAV system minimum set point must be adequate to maintain the recommended mechanical and outdoor ACH and a negative pressure ≥0.01 inch of water gauge compared with adjacent areas.
Based on the risk assessment for the setting, the required number of AII rooms, other negative-pressure rooms, and local exhaust devices should be determined. The location of these rooms and devices will depend partially on where recommended ventilation conditions can be achieved. Grouping AII rooms in one area might facilitate the care of patients with TB disease and the installation and maintenance of optimal environmental controls.
AII rooms should be checked for negative pressure by using smoke tubes or other visual checks before occupancy, and these rooms should be checked daily when occupied by a patient with suspected or confirmed TB disease. Design, construct, and maintain general ventilation systems so that air flows from clean to less clean (more contaminated) areas. In addition, design general ventilation systems to provide optimal airflow patterns within rooms and to prevent air stagnation or short-circuiting of air from the supply area to the exhaust area.
Health-care settings serving populations with a high prevalence of TB disease might need to improve the existing general ventilation system or use air-cleaning technologies in general-use areas (e.g., waiting rooms, EMS areas, and radiology suites). Applicable approaches include 1) single-pass, nonrecirculating systems that exhaust air to the outside, 2) recirculation systems that pass air through HEPA filters before recirculating it to the general ventilation system, and 3) room-air recirculation units with HEPA filters and/or UVGI systems.
Air-Cleaning Methods
High-Efficiency Particulate Air (HEPA) Filters
HEPA filters can be used to filter infectious droplet nuclei from the air and must be used 1) when discharging air from local exhaust ventilation booths or enclosures directly into the surrounding room or area and 2) when discharging air from an AII room (or other negative-pressure room) into the general ventilation system (e.g., in settings in which the ventilation system or building configuration makes venting the exhaust to the outside impossible).
HEPA filters can be used to remove infectious droplet nuclei from air that is recirculated in a setting or exhausted directly to the outside. HEPA filters can also be used as a safety measure in exhaust ducts to remove droplet nuclei from air being discharged to the outside. Air can be recirculated through HEPA filters in areas in which 1) no general ventilation system is present, 2) an existing system is incapable of providing sufficient ACH, or 3) air-cleaning (particulate removal) without affecting the fresh-air supply or negative-pressure system is desired. Such uses can increase the number of equivalent ACH in the room or area.
Recirculation of HEPA filtered air can be achieved by exhausting air from the room into a duct, passing it through a HEPA filter installed in the duct, and returning it to the room or the general ventilation system. In addition, recirculation can be achieved by filtering air through HEPA recirculation systems installed on the wall or ceiling of the room or filtering air through portable room-air recirculation units.
To ensure adequate functioning, install HEPA filters carefully and maintain the filters according to the instructions of the manufacturer. Maintain written records of all prefilter and HEPA maintenance and monitoring (114). Manufacturers of room-air recirculation units should provide installation instructions and documentation of the filtration efficiency and of the overall efficiency of the unit (clean air delivery rate) in removing airborne particles from a space of a given size.
UVGI
UVGI is an air-cleaning technology that can be used in a room or corridor to irradiate the air in the upper portion of the room (upper-air irradiation) and is installed in a duct to irradiate air passing through the duct (duct irradiation) or incorporated into room air-recirculation units. UVGI can be used in ducts that recirculate air back into the same room or in ducts that exhaust air directly to the outside. However, UVGI should not be used in place of HEPA filters when discharging air from isolation booths or enclosures directly into the surrounding room or area or when discharging air from an AII room into the general ventilation system. Effective use of UVGI ensures that M. tuberculosis, as contained in an infectious droplet nucleus is exposed to a sufficient dose of ultraviolet-C (UV-C) radiation at 253.7 nanometers (nm) to result in inactivation. Because dose is a function of irradiance and time, the effectiveness of any application is determined by its ability to deliver sufficient irradiance for enough time to result in inactivation of the organism within the infectious droplet. Achieving a sufficient dose can be difficult for airborne inactivation because the exposure time can be substantially limited; therefore, attaining sufficient irradiance is essential.
For each system, follow design guidelines to maximize UVGI effectiveness in equivalent ACH. Because air velocity, air mixing, relative humidity, UVGI intensity, and lamp position all affect the efficacy of UVGI systems, consult a UVGI system designer before purchasing and installing a UVGI system. Experts who might be consulted include industrial hygienists, engineers, and health physicists.
To function properly and minimize potential hazards to HCWs and other room occupants, upper-air UVGI systems should be properly installed, maintained, and labeled. A person knowledgeable in the use of ultraviolet (UV) radiometers or actinometers should monitor UV irradiance levels to ensure that exposures in the work area are within safe exposure levels. UV irradiance levels in the upper-air, where the air disinfection is occurring, should also be monitored to determine that irradiance levels are within the desired effectiveness range.
UVGI tubes should be changed and cleaned according to the instructions of the manufacturer or when irradiance measurements indicate that output is reduced below effective levels. In settings that use UVGI systems, education of HCWs should include 1) basic principles of UVGI systems (mechanism and limitations), 2) potential hazardous effects of UVGI if overexposure occurs, 3) potential for photosensitivity associated with certain medical conditions or use of certain medications, and 4) the importance of maintenance procedures and record-keeping. In settings that use UVGI systems, patients and visitors should be informed of the purpose of UVGI systems and be warned about the potential hazards and safety precautions.
Program Issues
Personnel from engineering, maintenance, safety and infection control, and environmental health should collaborate to ensure the optimal selection, installation, operation, and maintenance of environmental controls. A written maintenance plan should be developed that outlines the responsibility and authority for maintenance of the environmental controls and addresses HCW training needs. Standard operating procedures should include the notification of infection-control personnel before performing maintenance on ventilation systems servicing TB patient-care areas.
Personnel should schedule routine preventive maintenance for all components of the ventilation systems (e.g., fans, filters, ducts, supply diffusers, and exhaust grills) and air-cleaning devices. Quality control (QC) checks should be conducted to verify that environmental controls are operating as designed and that records are current. Provisions for emergency electrical power should be made so that the performance of essential environmental controls is not interrupted during a power failure.
Respiratory Protection
The first two levels of the infection-control hierarchy, administrative and environmental controls, minimize the number of areas in which exposure to M. tuberculosis might occur. In addition, these administrative and environmental controls also reduce, but do not eliminate, the risk in the few areas in which exposures can still occur (e.g., AII rooms and rooms where cough-inducing or aerosol-generating procedures are performed). Because persons entering these areas might be exposed to airborne M. tuberculosis, the third level of the hierarchy is the use of respiratory protective equipment in situations that pose a high risk for exposure (see Supplement, Respiratory Protection).
On October 17, 1997, OSHA published a proposed standard for occupational exposure to M. tuberculosis (267). On December 31, 2003, OSHA announced the termination of rulemaking for a TB standard (268). Previous OSHA policy permitted the use of any Part 84 particulate filter respirator for protection against TB disease (269). Respirator use for TB had been regulated by OSHA under CFR Title 29, Part 1910.139 (29CFR1910.139) (270) and compliance policy directive (CPL) 2.106 (Enforcement Procedures and Scheduling for Occupational Exposure to Tuberculosis). Respirator use for TB is regulated under the general industry standard for respiratory protection (29 CFR 1910.134, http://www.osha.gov/SLTC/respiratoryprotection/index.html) (271). General information concerning respiratory protection for aerosols, including M. tuberculosis, has been published (272–274).
Indications for Use
Respiratory protection should be used by the following persons:
all persons, including HCWs and visitors, entering rooms in which patients with suspected or confirmed infectious TB disease are being isolated;
persons present during cough-inducing or aerosol-generating procedures performed on patients with suspected or confirmed infectious TB disease; and
persons in other settings in which administrative and environmental controls probably will not protect them from inhaling infectious airborne droplet nuclei. These persons might also include persons who transport patients with suspected or confirmed infectious TB disease in vehicles (e.g., EMS vehicles or, ideally, ambulances) and persons who provide urgent surgical or dental care to patients with suspected or confirmed infectious TB disease (see Supplement, Estimating the Infectiousness of a TB Patient).
Laboratorians conducting aerosol-producing procedures might require respiratory protection. A decision concerning use of respiratory protection in laboratories should be made on an individual basis, depending on the type of ventilation in use for the laboratory procedure and the likelihood of aerosolization of viable mycobacteria that might result from the laboratory procedure.
Respiratory-Protection Program
OSHA requires health-care settings in which HCWs use respiratory protection to develop, implement, and maintain a respiratory-protection program. All HCWs who use respiratory protection should be included in the program (see Supplement, Respiratory Protection).
Training HCWs
Annual training regarding multiple topics should be conducted for HCWs, including the nature, extent, and hazards of TB disease in the health-care setting. The training can be conducted in conjunction with other related training regarding infectious disease associated with airborne transmission. In addition, training topics should include the 1) risk assessment process and its relation to the respirator program, including signs and symbols used to indicate that respirators are required in certain areas and the reasons for using respirators; 2) environmental controls used to prevent the spread and reduce the concentration of infectious droplet nuclei; 3) selection of a particular respirator for a given hazard (see Selection of Respirators); 4) operation, capabilities, and limitations of respirators; 5) cautions regarding facial hair and respirator use (275,276); and 6) OSHA regulations regarding respirators, including assessment of employees' knowledge.
Trainees should be provided opportunities to handle and wear a respirator until they become proficient (see Fit Testing). Trainees should also be provided with 1) copies or summaries of lecture materials for use as references and 2) instructions to refer all respirator problems immediately to the respiratory program administrator.
Selection of Respirators
Respiratory protective devices used in health-care settings for protection against M. tuberculosis should meet the following criteria (277,278):
certified by CDC/National Institute for Occupational Safety and Health (NIOSH) as a nonpowered particulate filter respirator (N-, R-, and P-series 95%, 99%, and 100% filtration efficiency), including disposable respirators, or PAPRs with high efficiency filters (279);
ability to adequately fit respirator wearers (e.g., a fit factor of ≥100 for disposable and half facepiece respirators) who are included in a respiratory-protection program; and
ability to fit the different facial sizes and characteristics of HCWs. (This criterion can usually be met by making respirators available in different sizes and models.)
The fit of filtering facepiece respirators varies because of different facial types and respirator characteristics (10,280–289). Assistance with selection of respirators should be obtained through consultation with respirator fit-testing experts, CDC, occupational health and infection-control professional organizations, peer-reviewed research, respirator manufacturers, and advanced respirator training courses.
Fit Testing
A fit test is used to determine which respirator fits the user adequately and to ensure that the user knows when the respirator fits properly. After a risk assessment is conducted to validate the need for respiratory protection, perform fit testing during the initial respiratory-protection program training and periodically thereafter in accordance with federal, state, and local regulations.
Fit testing provides a means to determine which respirator model and size fits the wearer best and to confirm that the wearer can don the respirator properly to achieve a good fit. Periodic fit testing of respirators on HCWs can serve as an effective training tool in conjunction with the content included in employee training and retraining. The frequency of periodic fit testing should be determined by the occurrence of 1) risk for transmission of M. tuberculosis, 2) a change in facial features of the wearer, 3) medical condition that would affect respiratory function, 4) physical characteristics of respirator (despite the same model number), or 5) a change in the model or size of the assigned respirator (281).
Respirator Options: General Recommendations
In situations that require respiratory protection, the minimum respiratory protection device is a filtering facepiece (nonpowered, air-purifying, half-facepiece) respirator (e.g., an N95 disposable respirator). This CDC/NIOSH-certified respirator meets the minimum filtration performance for respiratory protection in areas in which patients with suspected or confirmed TB disease might be encountered. For situations in which the risk for exposure to M. tuberculosis is especially high because of cough-inducing and aerosol-generating procedures, more protective respirators might be needed (see Respirator Options: Special Circumstances).
Respirator Options: Special Circumstances
Visitors to AII rooms and other areas with patients who have suspected or confirmed infectious TB disease may be offered respirators and should be instructed by an HCW on the use of the respirator before entering an AII room (Supplement, Frequently Asked Questions [FAQs] User-Seal Check in Respiratory Protection section). Particulate respirators vary substantially by model, and fit testing is usually not easily available to visitors.
The risk assessment for the setting might identify a limited number of circumstances (e.g., bronchoscopy or autopsy on persons with suspected or confirmed TB disease and selected laboratory procedures) for which a level of respiratory protection that exceeds the minimum level provided by an N95 disposable respirator should be considered. In such circumstances, consider providing HCWs with a level of respiratory protection that both exceeds the minimum criteria and is compatible with patient care delivery. Such protection might include more protective respirators (e.g., full-facepiece respirators or PAPRs) (see Supplement, Respiratory Protection). Detailed information regarding these and other respirators has been published (272,273,278,290).
In certain settings, HCWs might be at risk for both inhalation exposure to M. tuberculosis and mucous membrane exposure to bloodborne pathogens. In these situations, the HCW might wear a nonfluid-resistant respirator with a full-face shield or the combination product surgical mask/N95 disposable respirator to achieve both respiratory protection and fluid protection.
When surgical procedures (or other procedures requiring a sterile field) are performed on persons with suspected or confirmed infectious TB disease, respiratory protection worn by HCWs must also protect the surgical field. The patient should be protected from the HCW's respiratory secretions and the HCW from infectious droplet nuclei that might be expelled by the patient or generated by the procedure. Respirators with exhalation valves and PAPRs do not protect the sterile field.
Settings in which patients with suspected or confirmed infectious TB disease will not be encountered do not need a respiratory-protection program for exposure to M. tuberculosis. However, these settings should have written protocols for the early identification of persons with symptoms or signs of TB disease and procedures for referring these patients to a setting where they can be evaluated and managed. Filtering facepiece respirators should also be available for emergency use by HCWs who might be exposed to persons with suspected or confirmed TB disease before transfer. In addition, respirators and the associated respiratory-protection program might be needed to protect HCWs from other infectious diseases or exposures to harmful vapors and gases. Their availability or projected need for other exposures should be considered in the selection of respirators for protection against TB to minimize replication of effort.
Surgical or procedure masks are designed to prevent respiratory secretions of the wearer from entering the air. To reduce the expulsion of droplet nuclei into the air, persons with suspected or confirmed TB disease should be instructed to observe respiratory hygiene and cough etiquette procedures (122) and should wear a surgical or procedure mask, if possible, when they are not in AII rooms. These patients do not need to wear particulate respirators.
Patients with suspected or confirmed TB disease should never wear any kind of respiratory protection that has an exhalation valve. This type of respirator does not prevent droplet nuclei from being expelled into the air.
Cough-Inducing and Aerosol-Generating Procedures
General Recommendations
Procedures that involve instrumentation of the lower respiratory tract or induction of sputum can increase the likelihood that droplet nuclei will be expelled into the air. These cough-inducing procedures include endotracheal intubation, suctioning, diagnostic sputum induction, aerosol treatments (e.g., pentamidine therapy and nebulized treatments), bronchoscopy, and laryngoscopy. Gastric aspiration and nasogastric tube placement can also induce cough in certain patients. Other procedures that can generate aerosols include irrigating TB abscesses, homogenizing or lyophilizing tissue, performing autopsies on cadavers with untreated TB disease, and other processing of tissue that might contain tubercle bacilli and TB laboratory procedures.
If possible, postpone cough-inducing or aerosol-generating procedures on patients with suspected or confirmed infectious TB disease unless the procedure can be performed with recommended precautions. When a cough-inducing or aerosol-generating procedure must be performed on a patient with suspected or confirmed infectious TB disease, use a local exhaust ventilation device (e.g., booth or special enclosure). If using this device is not feasible, perform the procedure in a room that meets the ventilation requirements for an AII room.
After completion of cough-inducing procedures, keep patients in the AII room or enclosure until coughing subsides. Patients should be given tissues and instructed to cover the mouth and nose with tissues when coughing. Tissues should be disposed of in accordance with the infection-control plan.
Before the booth, enclosure, or room is used for another patient, allow enough time for the removal of ≥99% of airborne contaminants. This interval will vary based on the efficiency of the ventilation or filtration system (Table 1).
For postoperative recovery, do not place the patient in a recovery room with other patients; place the patient in a room that meets the ventilation requirements for an AII room. If the room does not meet the ventilation requirements for an AII room, air-cleaning technologies (e.g., HEPA filtration and UVGI) can be used to increase the number of equivalent ACH (see Supplement, Environmental Controls).
Perform all manipulations of suspected or confirmed M. tuberculosis specimens that might generate aerosols in a BSC. When in rooms or enclosures in which cough-inducing or aerosol-generating procedures are being performed, respiratory protection should be worn.
Special Considerations for Bronchoscopy
Bronchoscopy can result in the transmission of M. tuberculosis either through the airborne route (63,81,86,162) or a contaminated bronchoscope (80,82,163–169). Whenever feasible, perform bronchoscopy in a room that meets the ventilation requirements for an AII room (see Supplement, Environmental Controls). Air-cleaning technologies can be used to increase equivalent ACH. If a bronchoscopy must be performed in a positive-pressure room (e.g., OR), exclude TB disease before performing the procedure. Examine three spontaneous or induced sputum specimens for AFB (if possible) to exclude a diagnosis of TB disease before bronchoscopy is considered as a diagnostic procedure (110,291).
In a patient who is intubated and mechanically ventilated, minimize the opening of circuitry. For HCWs present during bronchoscopic procedures on patients with suspected or confirmed TB disease, a respirator with a level of protection of at least an N95 disposable respirator should be worn. Protection greater than an N95 disposable respirator (e.g., a full-facepiece elastomeric respirator or PAPR) should be considered.
Special Considerations for Administration of Aerosolized Pentamidine and Other Medications
Patients receiving aerosolized pentamidine (or other aerosolized medications) who are immunocompromised and have a confirmed or suspected pulmonary infection (i.e., pneumocystis pneumonia [PCP] or pneumonia caused by P. jaroveci, formerly P. carinii) are also at risk for TB disease. Patients receiving other aerosolized medications might have an immunocompromising condition that puts them at greater risk for TB disease. Patients should be screened for TB disease before initiating prophylaxis with aerosolized pentamidine; a medical history, test for infection with M. tuberculosis, and a chest radiograph should be performed.
Before each subsequent treatment with aerosolized pentamidine, screen patients for symptoms or signs of TB disease. If symptoms or signs are present, evaluate the patient for TB disease. Patients with suspected or confirmed TB disease should be administered oral prophylaxis for P. jaroveci instead of aerosolized pentamidine if clinically practical. Patients receiving other aerosolized medication might have immunocompromising conditions; therefore, if warranted, they should be similarly screened and evaluated, and treatment with oral medications should be considered.
Supplements
Estimating the Infectiousness of a TB Patient
General Principles
Transmission of M. tuberculosis is most likely to result from exposure to persons who have 1) unsuspected pulmonary TB disease and are not receiving antituberculosis treatment, 2) diagnosed TB disease and are receiving inadequate therapy, or 3) diagnosed TB disease and are early in the course of effective therapy. Administration of effective antituberculosis treatment has been associated with decreased infectiousness among persons who have TB disease (292). Effective treatment reduces coughing, the amount of sputum produced, the number of organisms in the sputum, and the viability of the organisms in the sputum. However, the duration of therapy required to decrease or eliminate infectiousness varies (293). Certain TB patients are never infectious, whereas those with unrecognized or inadequately treated drug-resistant TB disease might remain infectious for weeks or months (2,3,87,94,162,294–297). In one study, 17% of transmission occurred from persons with negative AFB smear results (262). Rapid laboratory methods, including PCR-based techniques, can decrease diagnostic delay and reduce the duration of infectiousness (298).
The infectiousness of patients with TB correlates with the number of organisms they expel into the air (299). The number of organisms expelled are related to the following factors: 1) presence of cough lasting ≥3 weeks; 2) cavitation on chest radiograph; 3) positive AFB sputum smear result; 4) respiratory tract disease with involvement of the lung or airways, including larynx; 5) failure to cover the mouth and nose when coughing; 6) lack of, incorrect, or short duration of antituberculosis treatment (300); or 7) undergoing cough-inducing or aerosol-generating procedures (e.g., sputum induction, bronchoscopy, and airway suction). Closed and effectively filtered ventilatory circuitry and minimized opening of such circuitry in intubated and mechanically ventilated patients might minimize exposure (see Intensive Care Units [ICUs]).
Persons with extrapulmonary TB disease usually are not infectious unless they have concomitant pulmonary disease, nonpulmonary disease located in the oral cavity or the larynx, or extrapulmonary disease that includes an open abscess or lesion in which the concentration of organisms is high, especially if drainage from the abscess or lesion is extensive, or if aerosolization of drainage fluid is performed (69,72,77,83,301). Persons with TB pleural effusions might also have concurrent unsuspected pulmonary or laryngeal TB disease. These patients should be considered infectious until pulmonary TB disease is excluded. Patients with suspected TB pleural effusions or extrapulmonary TB disease should be considered pulmonary TB suspects until concomitant pulmonary disease is excluded (302).
Although children with TB disease usually are less likely than adults to be infectious, transmission from young children can occur (135,137). Therefore, children and adolescents with TB disease should be evaluated for infectiousness by using the majority of the same criteria as for adults. These criteria include presence of cough lasting ≥3 weeks; cavitation on chest radiograph; or respiratory tract disease with involvement of lungs, airways, or larynx. Infectiousness would be increased if the patient were on nonstandard or short duration of antituberculosis treatment (300) or undergoing cough-inducing or aerosol-generating procedures (e.g., sputum induction, bronchoscopy, and airway suction). Although gastric lavage is useful in the diagnosis of pediatric TB disease, the grade of the positive AFB smear result does not correlate with infectiousness. Pediatric patients who might be infectious include those who are not on antituberculosis treatment, who have just been started on treatment or are on inadequate treatment, and who have extensive pulmonary or laryngeal involvement (i.e., coughing ≥3 weeks, cavitary TB disease, positive AFB sputum smear results, or undergoing cough-inducing or aerosol-generating procedures). Children who have typical primary TB lesions on chest radiograph and do not have any of these indicators of infectiousness might not need to be placed in an AII room.
No data exist on the transmission of M. tuberculosis and its association with the collection of gastric aspirate specimens. Children who do not have predictors for infectiousness do not need to have gastric aspirates obtained in an AII room or other special enclosure; however, the procedure should not be performed in an area in which persons infected with HIV might be exposed. Because the source case for pediatric TB patients might be a member of the infected child's family, parents and other visitors of all hospitalized pediatric TB patients should be screened for TB disease as soon as possible to ensure that they do not become sources of health-care–associated transmission of M. tuberculosis (303–306).
Patients who have suspected or confirmed TB disease and who are not on antituberculosis treatment usually should be considered infectious if characteristics include
presence of cough;
cavitation on chest radiograph;
positive AFB sputum smear result;
respiratory tract disease with involvement of the lung or airways, including larynx;
failure to cover the mouth and nose when coughing; and
undergoing cough-inducing or aerosol-generating procedures (e.g., sputum induction, bronchoscopy, and airway suction).
If a patient with one or more of these characteristics is on standard multidrug therapy with documented clinical improvement usually in connection with smear conversion over multiple weeks, the risk for infectiousness is reduced.
Suspected TB Disease
For patients placed under airborne precautions because of suspected infectious TB disease of the lungs, airway, or larynx, airborne precautions can be discontinued when infectious TB disease is considered unlikely and either 1) another diagnosis is made that explains the clinical syndrome or 2) the patient has three negative AFB sputum smear results (109–112). Each of the three consecutive sputum specimens should be collected in 8–24-hour intervals (124), and at least one specimen should be an early morning specimen because respiratory secretions pool overnight. Generally, this method will allow patients with negative sputum smear results to be released from airborne precautions in 2 days.
Hospitalized patients for whom the suspicion of TB disease remains after the collection of three negative AFB sputum smear results should not be released from airborne precautions until they are on standard multidrug antituberculosis treatment and are clinically improving. If the patient is believed to not have TB disease because of an alternate diagnosis or because clinical information is not consistent with TB disease, airborne precautions may be discontinued. Therefore, a patient suspected of having TB disease of the lung, airway, or larynx who is symptomatic with cough and not responding clinically to antituberculosis treatment should not be released from an AII room into a non-AII room, and additional sputum specimens should be collected for AFB examination until three negative AFB sputum smear results are obtained (30,31). Additional diagnostic approaches might need to be considered (e.g., sputum induction) and, after sufficient time on treatment, bronchoscopy.
Confirmed TB Disease
A patient who has drug-susceptible TB of the lung, airway, or larynx, who is on standard multidrug antituberculosis treatment, and who has had a substantial clinical and bacteriologic response to therapy (i.e., reduction in cough, resolution of fever, and progressively decreasing quantity of AFB on smear result) is probably no longer infectious. However, because culture and drug-susceptibility results are not usually known when the decision to discontinue airborne precautions is made, all patients with suspected TB disease should remain under airborne precautions while they are hospitalized until they have had three consecutive negative AFB sputum smear results, each collected in 8–24-hour intervals, with at least one being an early morning specimen; have received standard multidrug antituberculosis treatment (minimum of 2 weeks); and have demonstrated clinical improvement.
Discharge to Home of Patients with Suspected or Confirmed TB Disease
If a hospitalized patient who has suspected or confirmed TB disease is deemed medically stable (including patients with positive AFB sputum smear results indicating pulmonary TB disease), the patient can be discharged from the hospital before converting the positive AFB sputum smear results to negative AFB sputum smear results, if the following parameters have been met:
a specific plan exists for follow-up care with the local TB-control program;
the patient has been started on a standard multidrug antituberculosis treatment regimen, and DOT has been arranged;
no infants and children aged <4 years or persons with immunocompromising conditions are present in the household;
all immunocompetent household members have been previously exposed to the patient; and
the patient is willing to not travel outside of the home except for health-care–associated visits until the patient has negative sputum smear results.
Patients with suspected or confirmed infectious TB disease should not be released to health-care settings or homes in which the patient can expose others who are at high risk for progressing to TB disease if infected (e.g., persons infected with HIV or infants and children aged <4 years). Coordination with the local health department TB program is indicated in such circumstances.
Drug-Resistant TB Disease
Because the consequences of transmission of MDR TB are severe, certain infection-control practitioners might choose to keep persons with suspected or confirmed MDR TB disease under airborne precautions during the entire hospitalization or until culture conversion is documented, regardless of sputum smear results. The role of drug resistance in transmission is complex. Transmission of drug-resistant organisms to persons with and without HIV infection has been documented (54,307–309). In certain cases, transmission from patients with TB disease caused by drug-resistant organisms might be extensive because of prolonged infectiousness as a result of delays in diagnosis and delays in initiation of effective therapy (53,94,98,101,255,310,311).
HIV-Associated TB Disease
Although multiple TB outbreaks among HIV-infected persons have been reported (51,52,99), the risk for transmission does not appear to be increased from patients with TB disease and HIV infection, compared with TB patients without HIV infection (54,312–315). Whether persons infected with HIV are more likely to be infected with M. tuberculosis if exposed is unclear; however, after infected with M. tuberculosis, the risk for progression to TB disease in persons infected with HIV is high (316). Progression to TB disease can be rapid, as soon as 1 month after exposure (51,53,54,101).
Diagnostic Procedures for LTBI and TB Disease
LTBI is a condition that develops after exposure to a person with infectious TB disease, and subsequent infection with M. tuberculosis occurs where the bacilli are alive but inactive in the body. Persons who have LTBI but who do not have TB disease are asymptomatic (i.e., have no symptoms), do not feel sick, and cannot spread TB to other persons.
Use of QFT-G for Diagnosing M. tuberculosis Infections in Health-Care Workers (HCWs)
In the United States, LTBI has been traditionally diagnosed based on a positive TST result after TB disease has been excluded. In vitro cytokine-based immunoassays for the detection of M. tuberculosis infection have been the focus of intense research and development. This document uses the term "BAMT" to refer to blood assay for M. tuberculosis infection currently available in the United States.
One such BAMT is QFT (which is PPD-based) and the subsequently developed version, QFT-G. QFT-G measures cell-mediated immune responses to peptides representative of two M. tuberculosis proteins that are not present in any BCG vaccine strain and are absent from the majority of nontuberculosis mycobacteria. This assay was approved by FDA in 2005 and is an available option for detecting M. tuberculosis infection. CDC recommendations for the United States on QFT and QFT-G have been published (35).
QFT-G is an in vitro test based on measuring interferon-gamma (IFN-γ) released in heparinized whole blood when incubated overnight with mitogen (serving as a positive control), Nil (i.e., all reagents except antigens, which sets a baseline), and peptide simulating ESAT-6 (6-kDa early secretory antigenic target) and CFP-10 (10-kDa culture filtrate protein) (measured independently), two different proteins with similar amino acid sequences specific for M. tuberculosis (Box 2). The sequences of ESAT-6 and CFP-10 are not related to each other. The genes encoding these two proteins are usually found next to each other in an operon (i.e., are coexpressed and translated from an mRNA product containing both genes). Although mycobacterial genomes contain multiple copies of each family, QFT-G and Elispot detect immunoreactivity associated only with the ESAT-6 protein and CFP-10 protein encoded by the genes in the region of deletion (RD1). In addition, virulence attributes are associated with the RD1 genes only and not the other homologues.
Specific antigens of these two proteins are found in M. tuberculosis–complex organisms (i.e., M. tuberculosis, M. bovis, M. africanum, M. microti, M. canetti, M. caprae, and M. pinnipedii), but not in the majority of other mycobacteria or in vaccine-variant M. bovis, BCG. Lymphocytes from the majority of persons who have been infected by M. tuberculosis complex indicate their sensitivity to ESAT-6 or CFP-10 by releasing IFN-γ, whereas infection by the majority of other mycobacteria, including BCG, does not appear to cause this sensitivity.
The blood tests using IFN-γ methods require one less patient visit, assess responsiveness to M. tuberculosis antigens, and do not boost anamnestic immune responses. Interpretation of the BAMT result is less subjective than interpretation of a skin test result, and the BAMT result might be affected less by previous BCG vaccination and sensitization to environmental mycobacteria (e.g., M. avium complex) than the PPD-based TST. BAMT might be more efficient and cost effective than TST (35). Screening programs that use BAMT might eliminate the need for two-step testing because this test does not boost sensitization.
Other cytokine-based immunoassays are under development and might be useful in the diagnosis of M. tuberculosis infection. Future FDA-approved products, in combination with CDC-issued recommendations, might provide additional diagnostic alternatives. For guidance on the use of these and related technologies, CDC plans to periodically publish recommendations on the diagnosis of M. tuberculosis infection. BAMT can be used in both testing and infection-control surveillance programs for HCWs.
Use of Tuberculin Skin Test (TST) for Diagnosing M. tuberculosis Infections in HCWs
The TST is frequently the first step of a TB diagnostic evaluation that might lead to diagnosing LTBI. Although currently available preparations of PPD used in TST are <100% sensitive and specific for the detection of LTBI, the TST is currently the most widely used diagnostic test for M. tuberculosis infection in the United States. The TST is less sensitive in patients who have TB disease.
The TST, like all medical tests, is subject to variability (74,228,317), but many of the inherent variations in administering and reading TST results can be avoided by training and attention to detail (318). Details of TST administration and TST result reading procedures are suggested in this report to improve the technical aspects of TST placement and reading, thus reducing observer variations and improving test reliability (Appendix F). These checklists were developed for the National Health and Nutrition Examination Survey (NHANES) to standardize TST placement and reading for research purposes. The suggested TST training recommendations are not mandatory.
Adherence to TST
Operational policies, procedures, and practices at health-care settings can enhance HCW adherence to serial TST. In 2002, one focus group study identified potential barriers and facilitators to adherence with routine TST (319). HCWs identified structural factors (e.g., inconvenient TST screening schedules and locations and long waiting times) that negatively affected adherence. Facilitators to help HCWs adhere to routine TST included active follow-up by supervisors and occupational health staff and work-site visits for TST screening. Misinformation and stigma concerning TB also emerged in the discussions, indicating the need for additional training and education for HCWs.
Administering the TST
For each patient, a risk assessment should be conducted that takes into consideration recent exposure to M. tuberculosis, clinical conditions that increase risk for TB disease if infected, and the program's capacity to deliver treatment for LTBI to determine if the TST should be administered.
The recommended method for TST is the Mantoux method (Appendix F) (223,318,320–322). Mantoux TST training materials supporting the guidance in this report are available at http://www.cdc.gov/tb (223,318,320–325). Multipuncture tests (e.g., Tine(r) tests) are not as reliable as the Mantoux method of skin testing and should not be used as a diagnostic test in the United States (30). Contact the state and local health department for TST resources.
Reading the TST Result
The TST result should be read by a designated, trained HCW 48–72 hours after the TST is placed (39,326,327). If the TST was not read between 48–72 hours, ideally, another TST should be placed as soon as possible and read within 48–72 hours (39). Certain studies indicate that positive TST reactions might still be measurable from 4–7 days after testing (225,226,328). However, if a patient fails to return within 72 hours and has a negative test result, the TST should be repeated (42). Patients and HCWs should not be allowed to read their own TST results. HCWs do not typically measure their own TST results reliably (48).
Reading the TST result consists of first determining the presence or absence of induration (hard, dense, and raised formation) and, if induration is present, measuring the diameter of induration transverse (perpendicular) to the long axis of the forearm (Figure 1) (39,318). Erythema or redness of the skin should not be considered when reading a TST result (Appendix F).
Interpreting TST Results
The positive-predictive value of a TST is the probability that a person with a positive TST result is actually infected with M. tuberculosis. The positive predictive value is dependent on the prevalence of infection with M. tuberculosis in the population being tested and the sensitivity and specificity of the test (228,329,330).
In populations with a low prevalence of M. tuberculosis infection, the probability that a positive TST result represents true infection with M. tuberculosis can be substantially low, especially if the cut point is set too low (i.e., the test is not adequately specific and a low prevalence exists in the population). In populations with a high prevalence of infection with M. tuberculosis and inadequate test specificity, the probability that a positive TST result using the same cut point represents true infection with M. tuberculosis is much higher.
Interpreting TST Results in HCWs
TST result interpretation depends on two factors: 1) measured TST induration in millimeters and 2) the person's risk for being infected with M. tuberculosis and risk for progression to TB disease if infected.
Intepretations of TST and QFT results vary according to the purpose of testing (Box 3). A TST result with no induration (0 mm) or a measured induration below the defined cut point for each category is considered to signify absence of infection with M. tuberculosis.
In the context of TST screening as part of a TB infection-control program, the interpretation of TST results occurs in two distinct parts. The first is the interpretation by standard criteria, without regard to personal risk factors or setting-specific factors of the TST results for infection control, surveillance, and referral purposes. The second is the interpretation by individualized criteria to determine the need for treatment of LTBI.
Determining the need for treatment of LTBI is a subsequent and separate task. For infection-control and surveillance purposes, TST results should be interpreted and recorded under strict criteria, without considering setting-based or personal risk factors (see Supplement, Diagnostic Procedures for LTBI and TB Disease). Any HCW with a positive TST result from serial TB screening should be referred to a medical provider for an evaluation and to determine the need for treatment of LTBI based on individual risk (Box 3).
Interpreting the TST Result for Infection Control and Surveillance
On baseline TST testing, a TST result of ≥10 mm is considered positive for the majority of HCWs, and a TST result of ≥5 mm is considered positive for HCWs who are infected with HIV or who have other immunocompromising conditions (Box 3). All HCWs with positive baseline TST results should be referred for medical and diagnostic evaluation; additional skin testing does not need to be performed.
On serial screening for the purposes of infection-control surveillance, TST results indicating an increase of ≥10 mm within 2 years should be interpreted and recorded as a TST conversion. For the purposes of assessing and monitoring infection control, TST conversion rates should be regularly determined. Health-care settings with a substantial number of HCWs to be tested might have systems in place that can accurately determine the TST conversion rate every month (e.g., from among a group of HCWs tested annually), whereas smaller settings might have imprecise estimates of their TST conversion rate even with annual assessments.
The precision of the setting's TST conversion rate and any analysis assessing change from baseline TST results will depend on the number and frequency of HCWs tested. These factors should be considered when establishing a regular interval for TB screening for HCWs.
After a known exposure in a health-care setting, close HCW contacts who have TST results of ≥5 mm should be considered to have positive TST results, which should be interpreted as new infections only in HCWs whose previous TST result is 0 mm. However, HCWs 1) with a baseline or follow-up TST result of >0 mm but <10 mm with a health-care–associated exposure to M. tuberculosis and 2) who then have an increase of ≥10 mm should be considered to have a TST conversion because of a new infection (Box 3).
In a contact investigation, a follow-up TST should be administered 8–10 weeks after the end of exposure (rather than 1–3 weeks later, as in two-step testing). In this instance, a change from a negative TST result to a positive TST result should not be interpreted as a boosted reaction. The change in the TST result indicates a TST conversion, recent exposure, transmission, and infection.
All HCWs who are immunocompromised should be referred for a medical and diagnostic evaluation for any TST result of ≥5 mm on baseline or follow-up screening. Because infection-control staff will usually not know the immune status of the HCWs being tested, HCWs who have TST results of 5–9 mm should be advised that such results can be an indication for referral for medical evaluation for HCWs who have HIV infection or other causes of severe immunosuppression.
After an HCW has met criteria for a positive TST result, including HCWs who will not receive treatment for LTBI, repeat TSTs are not necessary because the results would not provide any additional information (30). This approach applies to HCWs who have positive TST results but who will not receive treatment for LTBI after medical evaluation. For future TB screening in settings that are medium risk, instead of participating in serial skin testing, the HCW should receive a medical evaluation and a symptom screen annually.
Interpreting the TST Result for Medical and Diagnostic Referral and Evaluation
HCWs who have positive TST results and who meet the criteria for referral should have a medical and diagnostic evaluation. For HCWs who are at low risk (e.g., those from low-incidence settings), a baseline result of ≥15 mm of induration (instead of ≥10 mm) might possibly be the cut point. The criteria used to determine the need for treatment of LTBI has been presented.
When making decisions for the diagnosis and treatment of LTBI, setting-based risk factors (e.g., the prevalence of TB disease and personal risk factors such as having an immunocompromising condition or known contact with a TB case) should be assessed when choosing the cut point for a positive TST result. The medical evaluation can occur in different settings, including an occupational health clinic, local or state health department, or private medical clinic.
When 15 mm is used as the cut point, TST results of 10–14 mm can be considered clinically negative (331). These HCWs should not have repeat TST, and the referring physician might not recommend treatment for LTBI. This issue of false-positive TST results might be especially true in areas of the country where the prevalence of infection with NTM is high.
HCWs who have TST results of 5–9 mm on baseline two-step testing should be advised that such results might be an indication for treatment of LTBI if the HCW is a contact of a person with infectious TB disease, has HIV infection, or has other causes of severe immunosuppression (e.g., organ transplant and receipt of the equivalent of ≥15 mg/day of prednisone for ≥1 month). The risk for TB disease in persons treated with corticosteroids increases with higher dose and longer duration of corticosteroid use. TNF-α antagonists also substantially increase the risk for progression to TB disease in persons with LTBI (332).
HCWs with negative baseline two-step TST results who are referred for medical evaluation for an increase of ≥10 mm induration on follow-up TST screening, including those who are otherwise at low risk for TB disease, probably acquired M. tuberculosis infection since receiving the previous TST and should be evaluated for TB disease. If disease is excluded, the HCW should be offered treatment for LTBI if they have no contraindication to treatment.
QC Program for Techniques for TST Administration and Reading TST Results
Random variation (i.e., differences in procedural techniques) in TST administration and reading TST results can cause false-positive or false-negative TST results. Many of the variations in administering and reading TST results can be avoided by conducting training and maintaining attention to details. HCWs who are responsible for TST procedures should be trained to reduce variation by following standardized operational procedures and should be observed by an expert TST trainer. All TST procedures (i.e., administering, reading, and recording the results) should be supervised and controlled to detect and correct variation. Corrective actions might include coaching and demonstration by the TST trainer. Annual re-training is recommended for HCWs responsible for administering and reading TST results.
One strategy to identify TST procedure variation is to use a QC tool (Appendix F). The expert TST trainer should observe the procedures and indicate procedural variation on the observation checklists. An expert trainer includes persons who have documented training experience.
QC for Administering TST by the Mantoux Method
Ideally, the TST trainer should participate in QC TST administrations with other TST trainers to maintain TST trainer certification. State regulations specify who is qualified to administer the test by injection. The TST trainer should first ensure antigen stability by maintaining the manufacturer's recommended cold chain (i.e., controlling antigen exposure to heat and light from the time it is out of refrigeration until the time it is placed back into refrigeration or until the vial is empty or expired). The TST trainer should prevent infection during an injection by preparing the skin and preventing contamination of solution, needle, and syringe.
The TST trainer should prevent antigen administration errors by controlling the five rights of administration: 1) right antigen; 2) right dose; 3) right patient; 4) right route; and 5) right time for TST administration, reading, and clinical evaluation (333). Finally, the TST trainer should observe and coach the HCW trainee in administering multiple intradermal injections by the Mantoux method. The TST trainer should record procedural variation on the observation checklist (Appendix F). TST training and coaching should continue until more than 10 correct skin test placements (i.e., ≥6 mm wheal) are achieved.
For training purposes, normal saline for injection can be used instead of PPD for intradermal injections. Volunteers are usually other HCWs who agree to be tested. Attempt to recruit volunteers who have known positive TST results so the trainees can practice reading positive TST results. A previous TST is not a contraindication to a subsequent TST unless the test was associated with severe ulceration or anaphylactic shock, which are substantially rare adverse events (30,237,238).
Model TST Training Program
A model TST training program for placing TST and reading TST results has been produced by NHANES (326). The number of hours, sessions, and blinded independent duplicate reading (BIDR) readings should be determined by the setting's TB risk assessment. The following information can be useful for a model TST training program. The suggested TST training recommendations are not mandatory.
Initial training for a TST placer ideally consists of three components.
Introductory lecture and demonstration by an expert TST placer or trainer. An expert TST trainer is a qualified HCW who has received training on administering multiple TST and reading multiple TST results (consider 3 hours of lecture).
Supervised practical work using procedural checklists observed and coached by the expert TST trainer (Appendix F) (consider 9 hours of practical work).
Administration of more than 10 total skin tests on volunteers by using injectable saline and producing more than 10 wheals that measure 6–10 mm.
TST training should include supervised TST administration, which is a procedure in which an expert TST trainer supervises a TST trainee during all steps on the procedural observation checklist for TST administration (Appendix F). Wheal size should be checked for all supervised TST administrations, and skin tests should be repeated if wheal size is inadequate (i.e., <6 mm). TST training and coaching should continue until more than10 correct skin test placements (i.e., ≥6 mm wheal) are achieved.
QC for Reading TST Results by the Palpation Method
The TST trainer should participate in QC readings with other TST trainers to maintain TST trainer certification. When training HCWs to read TST results, providing measurable TST responses is helpful (i.e., attempt to recruit volunteers who have known positive TST results so that the trainees can practice reading positive TST results).
TST readers should correctly read both measurable (>0 mm) and nonmeasurable responses (0 mm) (e.g., consider reading more than 20 TST results [at least 10 measurable and at least 10 nonmeasurable], if possible). The TST trainer should observe and coach the HCW in reading multiple TST results by the Palpation method and should record procedure variation on the observation checklist (Appendix F).
The TST trainer should conduct BIDRs for comparison with the HCW's reading. BIDRs are performed when two or more consecutive TST readers immediately measure the same TST result by standard procedures, without consulting or observing one another's readings, and record results independently (may use recommended procedural observation checklist;
Appendix F). BIDRs help ensure that TST readers continue to read TST results correctly.
Initial training for a TST reader ideally should consist of multiple components.
Receiving an introductory lecture and demonstration by an expert TST reader. Training materials are available from CDC (223,318) and CDC-sponsored Regional Model and Training Centers and should also be available at the local or state health department (consider 6 hours for lecture and demonstration).
Receiving four sessions of supervised practical work using procedural checklists (observed and coached by an expert TST reader) (consider 16 hours of practical work).
Performing BIDR readings (consider more than 80, if possible). TST trainers should attempt to organize the sessions so that at least 50% of the TST results read have a result of >0 mm according to the expert TST reader.
Performing BIDR readings on the last day of TST training (consider more than 30 BIDR readings out of the total 80 readings, if possible). TST trainers should attempt to ensure that at least 25% of persons tested have a TST result of >0 mm, according to the expert TST reader.
Missing no more than two items on the procedural observation checklist (Appendix F) for three random observations by an expert TST reader.
Performing all procedures on the checklist correctly during the final observation.
TST training and coaching should continue until the HCW is able to perform all procedures correctly and until a satisfactory measurement is achieved (i.e., the trainer and the trainee read the TST results within 2 mm of each other). For example, if the trainer reads the TST result as 11 mm (this might be considered the gold standard reading), the trainee's reading should be between 9–13 mm to be considered correct. Only a single measurement in millimeters should be recorded (not 11 mm x 11 mm or 11 mm x 15 mm). QC Procedural Observation Checklists (Appendix F) are recommended by CDC as a tool for use during TST training.
Special Considerations in TST
Anergy. The absence of a reaction to a TST does not exclude a diagnosis of TB disease or infection with M. tuberculosis. In immunocompromised persons, delayed-type hypersensitivity (DTH) responses (e.g., tuberculin reactions) can decrease or disappear more rapidly, and a limited number of otherwise healthy persons apparently are incapable of reacting to tuberculin even after diagnosed infection with M. tuberculosis. This condition, called anergy, can be caused by multiple factors (e.g., advanced HIV infection, measles infection, sarcoidosis, poor nutrition, certain medications, vaccinations, TB disease itself, and other factors) (307,334–338). However, anergy testing in conjunction with TB skin testing is no longer recommended routinely for screening for M. tuberculosis infection (336).
Reconstitution of DTH in HIV-infected persons taking antiretroviral therapy (ART). In one prospective study (340), TB patients who initially had negative TST results had positive TST results after initiation of HAART. HCWs must be aware of the potential public health and clinical implications of restored TST reactivity among persons who have not been diagnosed with TB disease but who might have LTBI. After the initiation of HAART repeat testing for infection with M. tuberculosis is recommended for HIV-infected persons previously known to have negative TST results (58). Recommendations on the prevention and treatment of TB in HIV-infected persons have been published (39,53,240).
Pregnancy. Tens of thousands of pregnant women have received TST since the test was developed, and no documented episodes of TST-related fetal harm have been reported (341). No evidence exists that the TST has adverse effects on the pregnant mother or fetus (39). Pregnant HCWs should be included in serial skin testing as part of an infection-control program or a contact investigation because no contraindication for skin testing exists (342). Guidelines issued by the American College of Obstetricians and Gynecologists (ACOG) emphasize that postponement of the diagnosis of infection with M. tuberculosis during pregnancy is unacceptable (343).
Booster phenomenon and two-step testing. In certain persons with LTBI, the DTH responsible for TST reactions wanes over time. Repeated TST can elicit a reaction called boosting in which an initial TST result is negative, but a subsequent TST result is positive. For example, a TST administered years after infection with M. tuberculosis can produce a false-negative result. This TST might stimulate (or boost) the person's ability to react to tuberculin, resulting in a positive result to a subsequent test (including the second step of a two-step procedure) (36,74,316,342,343). With serial testing, a boosted reaction on a subsequent TST might be misinterpreted as a newly acquired infection, compared with the false-negative result from the initial TST. Misinterpretation of a boosted reaction as a new infection with M. tuberculosis or TST conversion might prompt unnecessary investigations to find the source case, unnecessary treatment for the person tested, and unnecessary testing of other HCWs. The booster phenomenon can occur in anyone, but it is more likely to occur in older persons, persons with remote infection with M. tuberculosis (i.e., infected years ago), persons infected with NTM, and persons with previous BCG vaccination (39,229,234,344,345).
All newly employed HCWs who will be screened with TST should receive baseline two-step TST upon hire, unless they have documentation of either a positive TST result or treatment for LTBI or TB disease (39,224). Any setting might have HCWs at risk for boosting, and a rate of boosting even as low as 1% can result in unnecessary investigation of transmission. Therefore, two-step TSTs are needed to establish a baseline for persons who will receive serial TST (e.g., residents or staff of correctional facilities or LTCFs). This procedure is especially important for settings that are classified as low risk where testing is indicated only upon exposure. A reliable baseline test result is necessary to detect health-care–associated transmission of M. tuberculosis. Guidance for baseline TST for HCWs is included in this report (Box 3). To estimate the frequency of boosting in a particular setting, a four-appointment schedule of TST administration and reading (i.e., appointments for TST administration and reading both TST results) is necessary, rather than the three-appointment schedule (i.e., appointments for the administration of both tests, with reading of the second-step TST result only) (196).
Two-step testing should be used only for baseline screening, not in contact investigations. In a contact investigation, for persons with a negative TST, a follow-up test should be administered 8–10 weeks after the end of exposure (rather than 1–3 weeks later, as in a two-step TST). In this instance, a change from a negative to a positive TST result suggests that recent exposure, transmission, and infection occurred and should not be interpreted as a boosted response.
After a known exposure in a health-care setting (close contact to a patient or HCW with infectious TB disease), TST results of ≥5 mm should be considered positive and interpreted as a new infection in HCWs whose previous TST result is 0 mm. If an HCW has a baseline or follow-up TST result of >0 mm but ≤10 mm, a health-care–associated exposure to M. tuberculosis, and an increase in the TST size of ≥10 mm, the result should be interpreted as the HCW having a TST conversion because of new infection.
BCG vaccination. In the United States, vaccination with BCG is not recommended routinely for anyone, including HCWs or children (227). Previous BCG vaccination is not a contraindication to having a TST or two-step skin testing administered. HCWs with previous BCG vaccination should receive baseline and serial skin testing in the same manner as those without BCG vaccination (233) (Box 1).
Previous BCG vaccination can lead to boosting in baseline two-step testing in certain persons (74,231,344–346). Distinguishing a boosted TST reaction resulting from BCG vaccination (a false-positive TST result) and a TST result because of previous infection with M. tuberculosis (true positive TST result) is not possible (39). Infection-control programs should refer HCWs with positive TST results for medical evaluation as soon as possible (Box 3).
Previous BCG vaccination increases the probability of a boosted reaction that will probably be uncovered on initial two-step skin testing. For an HCW with a negative baseline two-step TST result who is a known contact of a patient who has suspected or confirmed infectious TB disease, treatment for LTBI should be considered if the follow-up TST result is ≥5 mm, regardless of BCG vaccination status.
PPD preparations for diagnosing infection with M. tuberculosis. Two PPD preparations are available in the United States: Tubersol(r) (Aventis Pasteur, Switftwater, Pennsylvania) (237) and APLISOL(r) (Parkdale Pharmaceuticals, Rochester, Michigan) (238). Compared with the U.S. reference PPD, no difference exists in TST interpretation between the two preparations (347). However, when Tubersol and Aplisol were compared with each other, a slight difference in reactivity was observed. Aplisol produced slightly larger reactions than Tubersol, but this difference was not statistically significant (347). The difference in specificity, 98% versus 99%, is limited. However, when applied in large institutional settings that test thousands of workers annually who are at low risk for infection with M. tuberculosis, this difference in specificity might affect the rate of positive TST results observed.
TB screening programs should use one antigen consistently and should realize that changes in products might make serial changes in TST results difficult to interpret. In one report, systematic changes in product use resulted in a cluster of pseudoconversions that were believed to have erroneously indicated a health-care–associated outbreak (348). Persons responsible for making decisions about the choice of pharmacy products should seek advice from the local or state health department's TB infection-control program before switching PPD preparations and should inform program staff of any changes.
Chest Radiography
Chest radiographic abnormalities can suggest pulmonary TB disease. Radiographic abnormalities that are consistent with pulmonary TB disease include upper-lobe infiltration, cavitation, and effusion. Infiltrates can be patchy or nodular and observed in the apical (in the top part of the lungs) or subapical posterior upper lobes or superior segment of the lower lobes in the lungs. HCWs who have positive test results for M. tuberculosis infection or symptoms or signs of TB disease, regardless of test results for M. tuberculosis infection, should have a chest radiograph performed to exclude a diagnosis of TB disease. However, a chest radiograph is not a substitute for tests for M. tuberculosis infection in a serial TB screening program for HCWs.
Persons who have LTBI or cured TB disease should not have repeat chest radiographs performed routinely (116). Repeat radiographs are not needed unless symptoms or signs of TB disease develop or a clinician recommends a repeat chest radiograph (39,116).
A chest radiograph to exclude pulmonary TB disease is indicated for all persons being considered for treatment of LTBI. If chest radiographs do not indicate pulmonary TB and if no symptoms or signs of TB disease are present, persons with a positive test result for infection with M. tuberculosis might be candidates for treatment of LTBI. In persons with LTBI, the chest radiograph is usually normal, although it might demonstrate abnormalities consistent with previous healed TB disease or other pulmonary conditions. In patients with symptoms or signs of TB disease, pulmonary infiltrates might only be apparent on a computed tomography (CT) scan. Previous, healed TB disease can produce radiographic findings that might differ from those associated with current TB disease, although a substantial overlap might exist. These findings include nodules, fibrotic scars, calcified granulomas, or basal pleural thickening. Nodules and fibrotic scars might contain slowly multiplying tubercle bacilli and pose a high risk for progression to TB disease. Calcified nodular lesions (calcified granulomas) and apical pleural thickening pose a lower risk for progression to TB disease (31).
Chest Radiography and Pregnancy
Because TB disease is dangerous to both mother and fetus, pregnant women who have a positive TST result or who are suspected of having TB disease, as indicated by symptoms or other concerns, should receive chest radiographs (with shielding consistent with safety guidelines) as soon as feasible, even during the first trimester of pregnancy (31,39,341).
Chest Radiography and HIV-Infected Persons
The radiographic presentation of pulmonary TB in persons infected with HIV might be apical; however, apical cavitary disease is less common among such patients. More common chest radiograph findings for HIV-infected persons are infiltrates in any lung zone, mediastinal or hilar adenopathy, or, occasionally, a normal chest radiograph. Typical and cavitary lesions are usually observed in patients with higher CD4 counts, and more atypical patterns are observed in patients with lower CD4 counts (31,49,94,142,349–354). In patients with symptoms and signs of TB, a negative chest radiograph result does not exclude TB. Such patients might be candidates for airborne precautions during medical evaluation.
Evaluation of Sputum Samples
Sputum examination is a critical diagnostic procedure for pulmonary TB disease (30) and is indicated for the following persons:
anyone suspected of having pulmonary or laryngeal TB disease;
persons with chest radiograph findings consistent with TB disease (current, previous, or healed TB);
persons with symptoms of infection in the lung, pleura, or airways, including larynx;
HIV-infected persons with any respiratory symptoms or signs, regardless of chest radiograph findings; and
persons suspected of having pulmonary TB disease for whom bronchoscopy is planned.
Sputum Specimen Collection
Persons requiring sputum collection for smear and culture should have at least three consecutive sputum specimens obtained, each collected in 8–24-hours intervals (124), with at least one being an early morning specimen (355). Specimens should be collected in a sputum induction booth or in an AII room. In resource-limited settings without environmental containment or when an AII room is not available, sputum collection can be performed safely outside of a building, away from other persons, windows, and ventilation intakes. Patients should be instructed on how to produce an adequate sputum specimen (containing little saliva) and should be supervised and observed by an HCW during the collection of sputum, if possible (30). If the patient's specimen is determined to be inadequate, it should still be sent for bacteriologic testing, although the inadequate nature of the specimen should be recorded. The HCW should wear an N95 disposable respirator during sputum collection.
Sputum Induction
For patients who are unable to produce an adequate sputum specimen, expectoration can be induced by inhalation of an aerosol of warm, hypertonic saline. Because sputum induction is a cough-inducing procedure, pre-treatment with a bronchodilator should be considered in patients with a history of asthma or other chronic obstructive airway diseases. Medical assistance and bronchodilator medication should be available during any sputum induction in the event of induced bronchospasm (109,356,357).
The patient should be seated in a small, well-ventilated sputum induction booth or in an AII room (see Environmental Controls; and Supplement, Environmental Controls). For best results, an ultrasonic nebulizer that generates an aerosol of approximately 5 mL/minute should be used. A 3% hypertonic saline is commercially available, and its safety has been demonstrated. At least 30 mL of 3% saline should be administered; administration of smaller volumes will have a lower yield. Higher concentrations can be used with an adjustment in the dose and closer monitoring for adverse effects.
Patients should be instructed to breathe deeply and cough intermittently. Sputum induction should be continued for up to 15 minutes or until an adequate specimen (containing little saliva) is produced. Induced sputum will often be clear and watery. Any expectorated material produced should be labeled as expectorated sputum and sent to the laboratory.
Laboratory Examination
Detection of AFB in stained smears by microscopy can provide the first bacteriologic indication of TB disease. Laboratories should report any positive smear results within 24 hours of receipt of the specimen (30). A positive result for AFB in a sputum smear is predictive of increased infectiousness. Smears allow presumptive detection of mycobacteria, but definitive identification, strain typing, and drug-susceptibility testing of M. tuberculosis require that a culture be performed (30). Negative AFB sputum smear results do not exclude a diagnosis of TB disease, especially if clinical suspicion of disease is high. In the United States, approximately 63% of patients with reported positive sputum culture results have positive AFB sputum smear results (26).
A culture of sputum or other clinical specimen that contains M. tuberculosis provides a definitive diagnosis of TB disease. In the majority of cases, identification of M. tuberculosis and drug-susceptibility results are available within 28 days (or 4–6 weeks) when recommended rapid methods such as liquid culture and DNA probes are used. Negative culture results are obtained in approximately 14% of patients with confirmed pulmonary TB disease (4,5). Testing sputum with rapid techniques (e.g., NAA) facilitates the rapid detection and identification of M. tuberculosis but should not replace culture and drug-susceptibility testing in patients with suspected TB disease (30,125,358). Mixed mycobacterial infection can obscure the identification of M. tuberculosis during the laboratory evaluation (e.g., because of cross-contamination or dual infections) and can be distinguished by the use of mycobacterial species-specific DNA probes (359). Examination of colony morphology on solid culture media can also be useful.
Drug-susceptibility tests should be performed on initial isolates from all patients to assist in identifying an effective antituberculosis treatment regimen. Drug-susceptibility tests should be repeated if sputum specimens continue to be culture-positive after 3 months of antituberculosis treatment or if culture results become positive for M. tuberculosis after a period of negative culture results (30,31).
Bronchoscopy
If possible, bronchoscopy should be avoided in patients with a clinical syndrome consistent with pulmonary or laryngeal TB disease because bronchoscopy substantially increases the risk for transmission either through an airborne route (63,80,81,162,360) or a contaminated bronchoscope (80,82,163–169), including in persons with negative AFB sputum smear results. Microscopic examination of three consecutive sputum specimens obtained in 8–24-hour intervals, with at least one obtained in the early morning, is recommended instead of bronchoscopy, if possible. In a patient who is intubated and mechanically ventilated, closed circuitry can reduce the risk for exposure.
If the suspicion for pulmonary TB disease is high or if the patient is seriously ill with a disorder, either pulmonary or extrapulmonary, that is believed to be TB disease, multidrug antituberculosis treatment using one of the recommended regimens should be initiated promptly, frequently before AFB smear results are known (31). Obtaining three sputum samples is safer than performing bronchoscopy. For AFB smear and culture results, three sputum samples have an increased yield compared with a single specimen (110,357), and induced specimens have better yield than specimens obtained without induction. Sputum induction is well-tolerated (90,109,132,133,357,361,362), even in children (134,356), and sputum specimens (either spontaneous or induced) should be obtained in all cases before a bronchoscopy (109,356,363,364).
In circumstances where a person who is suspected of having TB disease is not on a standard antituberculosis treatment regimen and the sputum smear results (possibly including induced specimens) are negative and a reasonably high suspicion for TB disease remains, additional consideration to initiate treatment for TB disease should be given. If the underlying cause of a radiographic abnormality remains unknown, additional evaluation with bronchoscopy might be indicated; however, in cases where TB disease remains a diagnostic possibility, initiation of a standard antituberculosis treatment regimen for a period before bronchoscopy might reduce the risk for transmission. Bronchoscopy might be valuable in establishing the diagnosis; in addition, a positive culture result can be both of clinical and public health importance to obtain drug-susceptibility results. Bronchoscopy in patients with suspected or confirmed TB disease should not be undertaken until after consideration of the risks for transmission of M. tuberculosis (30,63,81,162,360). If bronchoscopy is performed, because it is a cough-inducing procedure, additional sputum samples for AFB smear and culture should be collected after the procedure to increase the diagnostic yield.
Treatment Procedures for LTBI and TB Disease
Treatment for LTBI
Treatment for LTBI is essential to control and eliminate TB disease in the United States because it substantially reduces the risk that infection with M. tuberculosis will progress to TB disease (10,28). Certain groups of persons are at substantially high risk for developing TB disease after being infected, and every effort should be made to begin treatment for LTBI and to ensure that those persons complete the entire course of treatment (Table 3).
Before beginning treatment of LTBI, a diagnosis of TB disease should be excluded by history, medical examination, chest radiography, and, when indicated, bacteriologic studies. In addition, before offering treatment of LTBI, ensure that the patient has not experienced adverse reactions with previous isoniazid (INH) treatment (215).
Candidates for Treatment of LTBI
Persons in the following groups at high risk should be administered treatment for LTBI if their TST result is ≥5 mm or if their BAMT result is positive, regardless of age (31,39):
persons infected with HIV,
recent contacts with a person with TB disease,
persons with fibrotic changes on chest radiograph consistent with previous TB disease,
organ transplant recipients, and
other immunosuppressed persons (e.g., persons receiving ≥15 mg/day of prednisone for ≥1 month).
Persons in the following groups at high risk should be considered for treatment of LTBI if their TST result is ≥10 mm, or if the BAMT result is positive:
persons with TST or BAMT conversions;
persons born or who have lived in developing countries or countries with a high-incidence of TB disease;
persons who inject illicit drugs;
residents and employees in congregate settings that are at high risk (i.e., correctional facilities and LTCFs [e.g., hospices and skilled nursing facilities]), hospitals and other health-care facilities, residential settings for persons with HIV/AIDS or other immunocompromising conditions, and homeless shelters;
personnel from mycobacteriology laboratories;
persons with any of the following clinical conditions or other immunocompromising conditions that place them at high risk for TB disease:
— silicosis,
— diabetes mellitus,
— chronic renal failure,
— certain hematologic disorders (e.g., leukemias and lymphomas),
— other specific malignancies (e.g., carcinoma of the head, neck, or lung),
— unexplained weight loss of ≥10% of ideal body weight,
— gastrectomy, or
— jejunoileal bypass;
persons living in areas with high incidence of TB disease;
children aged <4 years; and
infants, children, and adolescents exposed to adults at high risk for developing TB disease.
Persons who use tobacco or alcohol (40,41), illegal drugs, including injection drugs and crack cocaine (43–48), might also be at increased risk for infection and disease, but because of the multiple other potential risk factors that commonly occur among such persons, use of these substances has been difficult to identify as separate risk factors.
Persons with no known risk factors for TB disease can be considered for treatment of LTBI if their TST result is ≥15 mm. However, programs to screen HCWs for infection with M. tuberculosis should only be conducted among groups at high risk. All testing activities should be accompanied by a plan for follow-up care for persons with LTBI or, if it is found, TB disease. A decision to test for infection with M. tuberculosis should be based on a commitment to treat LTBI after a medical examination (39).
Persons who might not be good candidates for treatment of LTBI include those with a previous history of liver injury or a history of excessive alcohol consumption. Active hepatitis and end-stage liver disease (ESLD) are relative contraindications to the use of INH for treatment of LTBI (39,240). If the decision is made to treat such patients, baseline and follow-up monitoring of serum aminotransaminases should be considered.
For persons who have previous positive TST or BAMT results and who completed treatment for LTBI previously, treating them again is not necessary. Documentation of completed therapy for LTBI is critical. Instead of participating in serial skin testing, the HCW should receive a medical evaluation and a symptom screen annually. A symptom screen is a procedure used during a clinical evaluation in which patients are asked if they have experienced any departure from normal in function, appearance, or sensation related to TB disease (e.g., cough).
Screening HCWs for infection with M. tuberculosis is an essential administrative measure for the control of transmission of M. tuberculosis in health-care settings. By conducting TB screening, ongoing transmission of M. tuberculosis can be detected, and future transmission can be prevented by identifying lapses in infection control and identifying persons infected with M. tuberculosis and TB disease. The majority of individual HCWs, however, do not have the risk factors for progression to disease that serve as the basis for the current recommendations for targeted testing and treatment of LTBI. The majority of HCWs in the United States do not provide care in areas in which the prevalence of TB is high. Therefore, HCWs should be tested, as determined by risk classification for the health-care setting, and can be categorized as having a positive test result or conversion for M. tuberculosis infection. HCWS can be categorized as part of the TB infection-control program for the purpose of surveillance and referral, but they might not necessarily be candidates for treatment of LTBI.
HCWs should receive serial screening for infection with M. tuberculosis (either TST or BAMT), as determined by the health-care setting's risk classification (Appendix B). For infection-control purposes, the results of the testing should be recorded and interpreted as part of the TB infection-control program as either a 1) negative TST result, 2) previously documented positive TST or BAMT result, or 3) TST or BAMT conversion. All recordings of TST results should also document the size of the induration in millimeters, not simply as negative or positive. BAMT results should be recorded in detail. The details should include date of blood draw, result in specific units, and the laboratory interpretation (positive, negative, or indeterminate) and the concentration of cytokine measured (e.g., IFN-γ).
To determine whether treatment for LTBI should be indicated, HCWs should be referred for medical and diagnostic evaluation according to the TST result criteria (Box 5). In conjunction with a medical and diagnostic evaluation, HCWs with positive test results for M. tuberculosis should be considered for treatment of LTBI (Box 5) after TB disease has been excluded by further medical evaluation. HCWs cannot be compelled to take treatment for LTBI, but they should be encouraged to do so if they are eligible for treatment.
HCWs' TST or BAMT results might be considered positive as part of the TB infection-control program for the purposes of surveillance and referral (i.e., meet the criterion for a conversion), and this occurrence is important to note. However, not all of these HCWs may be considered candidates for treatment of LTBI, according to the individual medical and diagnostic evaluation. After an HCW has been classified as having a positive result or conversion for M. tuberculosis infection, additional testing for M. tuberculosis infection is not necessary.
Treatment Regimens for LTBI
For persons suspected of having LTBI, treatment of LTBI should not begin until TB disease has been excluded. Persons highly suspected of having TB disease should receive the standard multidrug antituberculosis treatment regimen for TB disease until the diagnosis is excluded. Standard drug regimens for the treatment of LTBI have been presented (Table 3); however, modifications to those regimens should be considered under certain circumstances, including HIV infection, suspected drug resistance, and pregnancy (47,365).
Reports of severe liver injury and death associated with the combination of rifampin and pyrazinamide (RZ) for treatment of LTBI (366–368) prompted the American Thoracic Society and CDC to revise previous recommendations (39,53) to indicate that RZ generally should not be offered for the treatment of LTBI (240). If the potential benefits substantially outweigh the demonstrated risk for severe liver injury and death associated with this regimen and the patient has no contraindications, a physician with experience treating LTBI and TB disease should be consulted before using this regimen (246). Clinicians should continue the appropriate use of rifampin and pyrazinamide in standard multidrug antituberculosis treatment regimens for the treatment of TB disease (31). Collaborate with the local or state health department on decisions regarding DOT arrangements.
For all regimens for treatment of LTBI, nonadherence to intermittent dosing (i.e., once or twice weekly) results in a larger proportion of total doses missed than daily dosing. DOT should be used for all doses during the course of treatment of LTBI whenever feasible (31). Collaborate with the local or state health department on decisions regarding DOT arrangements.
Contacts of patients with drug-susceptible TB disease. Persons with a previously negative TST or BAMT result who are contacts of patients with drug-susceptible TB disease and who subsequently have a positive TST result (≥5 mm) or positive BAMT result should be evaluated for treatment of LTBI, regardless of age. The majority of persons who are infected with M. tuberculosis will have a positive TST result within 6 weeks of exposure (74,228,369–371). Therefore, contacts of patients with drug-susceptible TB disease with negative TST (or BAMT) results should be retested 8–10 weeks after the end of exposure to a patient with suspected or confirmed TB disease. Persons infected with M. tuberculosis should be advised that they possibly can be reinfected with M. tuberculosis if re-exposed (246,372–375). Persons infected with HIV, persons receiving immunosuppressive therapy, regardless of TST result, and persons with a previous positive TST or BAMT result who are close contacts of a person with suspected or confirmed TB disease should be considered for treatment of LTBI.
The interpretation of TST results is more complicated in a contact investigation among HCWs who have negative baseline TST results from two-step testing but where the induration was >0 mm on the baseline TST or subsequent serial testing. Differences in the TST results between the contact investigation and previous baseline and serial TST could be a result of 1) inter-test variability in reaction size; 2) intervening exposure to NTM, BCG, or M. tuberculosis; and 3) reversion. In practice, for TST, only inter-test variability and exposure to or infection with NTM or M. tuberculosis are likely.
Treatment of LTBI should not be started until a diagnosis of TB disease has been excluded. If uncertainty exists concerning the presence of TB disease because of an ambiguous chest radiograph, a standard multidrug antituberculosis treatment regimen can be started and adjusted as necessary based on the results of sputum cultures and the patient's clinical response (31). If cultures are obtained without initiating therapy, treatment for LTBI should not be initiated until all culture results are reported as negative.
Contacts of patients with drug-resistant TB disease. Treatment for LTBI caused by drug-resistant or MDR TB disease is complex and should be conducted in consultation with the local or state health department's infection-control program and experts in the medical management of drug-resistant TB. In certain instances, medical decision making for the person with LTBI will benefit from the results of drug susceptibility testing of the isolate of the index TB case. Treatment should be guided by susceptibility test results from the isolate to which the patient was exposed and presumed to be infected (31,376,377).
Pretreatment Evaluation and Monitoring of Treatment
The pretreatment evaluation of persons who are targeted for treatment of LTBI provides an opportunity for health-care providers to 1) establish rapport with patients; 2) discuss details of the patient's risk for progression from LTBI to TB disease; 3) explain the benefits of treatment and the importance of adhering to the drug regimen; 4) review possible adverse effects of the regimen, including interactions with other medications; and 5) establish an optimal follow-up plan.
Monitoring for adverse effects of antituberculosis medications must be individualized. Persons receiving treatment for LTBI should be specifically instructed to look for symptoms associated with the most common reactions to the medications they are taking (39). Laboratory testing should be performed to evaluate possible adverse effects (31,39). Routine laboratory monitoring during treatment of LTBI is indicated for patients with abnormal baseline test results and for persons with a risk for hepatic disease. Baseline laboratory testing is indicated for persons infected with HIV, pregnant women, women in the immediate postpartum period (usually within 3 months of delivery), persons with a history of liver disease, persons who use alcohol regularly, and those who have or are at risk for chronic liver disease.
All patients being treated for LTBI should be clinically monitored at least monthly, including a brief clinical assessment conducted in the person's primary language for signs of hepatitis (e.g., nausea, vomiting, abdominal pain, jaundice, and yellow or brown urine). Patients receiving treatment for LTBI should be advised about the adverse effects of the drugs and the need for prompt cessation of treatment and clinical evaluation if adverse effects occur.
Because of the risk for serious hepatic toxicity and death, the use of the combination of RZ for the treatment of LTBI generally should not be offered. If RZ is used, a physician with experience treating LTBI and TB disease should be consulted before the use of this regimen. In addition, more extensive biochemical and clinical monitoring is recommended (240).
Treatment for TB Disease
Suspected or confirmed TB cases must be reported to the local or state health department in accordance with laws and regulations. Case management for TB disease should be coordinated with officials of the local or state health department. Regimens for treatment of TB disease must contain multiple drugs to which the organisms are susceptible. For persons with TB disease, treatment with a single drug can lead to the development of mycobacterial resistance to that drug. Similarly, adding a single drug to a failing antituberculosis treatment regimen can lead to resistance to the added drug (31).
For the majority of patients, the preferred regimen for treating TB disease consists of an initiation 2-month phase of four drugs (INH, rifampin, pyrazinamide, and ethambutol) and at least a 4-month continuation phase of INH and rifampin (for a minimum total treatment of 6 months). Ethambutol may be discontinued if supporting drug susceptibility results are available. Completion of therapy is based on the number of doses taken within a maximal period and not simply 6 months (31). Persons with cavitary pulmonary TB disease and positive culture results of sputum specimens at the completion of 2 months of therapy should receive a longer (7-month continuation) phase because of the significantly higher rate of relapse (31).
TB treatment regimens might need to be altered for persons infected with HIV who are on ART (49). Whenever feasible, the care of persons with both TB disease and HIV infection should be provided by or in consultation with experts in the management of both TB and HIV-related disease (31). To prevent the emergence of rifampin-resistant organisms, persons with TB disease, HIV infection, and CD4 cell counts of <100 cells/mm3 should not be treated with highly intermittent (i.e., once or twice weekly) regimens. These patients should receive daily treatment during the intensive phase by DOT (if feasible) and daily or three times weekly by DOT during the continuation phase (378). Detailed information on TB treatment for persons infected with HIV has been published and is available (http://www.dhfs.state.wi.us/AIDS-HIV/Resources/Overviews/AIDS_HIV.htm, http://www.hiv-druginteractions.org, and http://www.cdc.gov/nchstp/tb/TB_HIV_Drugs/TOC.htm) and published (31,53).
Drug-susceptibility testing should be performed on all initial isolates from patients with TB disease. When results from drug-susceptibility tests become available, the antituberculosis treatment regimen should be reassessed, and the drugs used in combination should be adjusted accordingly (376,377,379–381). If drug resistance is present, clinicians who are not experts in the management of patients with drug-resistant TB disease should seek expert consultation (31) and collaborate with the local or state health department for treatment decisions.
The major determinant of the outcome of treatment is adherence to the drug regimen. Therefore, careful attention should be paid to measures designed to enable and foster adherence (31,319,382). DOT is an adherence-enhancing strategy in which a trained HCW or other specially trained person watches a patient swallow each dose of medication and records the dates that the DOT was observed. DOT is the standard of care for all patients with TB disease and should be used for all doses during the course of therapy for TB disease and for LTBI, whenever feasible. Plans for DOT should be coordinated with the local or state health department (31).
Reporting Serious Adverse Events
HCWs should report serious adverse events associated with the administration of tuberculin antigen or treatment of LTBI or TB disease to the FDA MedWatch, Adverse Event Reporting System (AERS), telephone: 800-FDA-1088, fax: 800-FDA-0178, http://www.fda.gov/medwatch. Report Form 3500, Physicians' Desk Reference. Specific instructions for the types of adverse events that should be reported are included in MedWatch report forms.
Surveillance and Detection of M. tuberculosis Infections in Health-Care Settings
TB disease should be considered for any patient who has symptoms or signs of disease, including coughing for ≥3 weeks, loss of appetite, unexplained weight loss, night sweats, bloody sputum or hemoptysis, hoarseness, fever, fatigue, or chest pain. The index of suspicion for TB disease will vary by individual risk factors, geographic area, and prevalence of TB disease in the population served by the health-care setting. Persons exposed to patients with infectious TB disease might acquire LTBI, depending on host immunity and the degree and duration of exposure. Diagnostic tests for TB disease include chest radiography and laboratory tests of sputum (examination for AFB and culture). The treatment of persons with TB disease involves vital aspects of TB control by stopping transmission of M. tuberculosis and preventing persons with LTBI from developing infectious TB disease (36).
In the majority of the U.S. population, targeted testing for LTBI and TB disease is performed to identify persons with LTBI and TB disease who would benefit from treatment. Therefore, all testing activities should be accompanied by a plan for follow-up care of persons with LTBI or TB disease. A decision to test for infection with M. tuberculosis should be based on a commitment to treat LTBI after a medical examination (39). Health-care agencies or other settings should consult with the local or state health department before starting a program to test HCWs for M. tuberculosis infection. This step ensures that adequate provisions are in place for the evaluation and treatment of persons whose test results are positive, including the medical supervision of the course of treatment for those who are treated for LTBI or TB disease.
Groups that are not at high risk for LTBI or TB disease should not be tested routinely because testing in populations at low risk diverts resources from other priority activities. In addition, testing persons at low risk for M. tuberculosis infection is discouraged because a substantial proportion of persons from populations at low risk who have positive TST results might actually have false-positive TST results and might not represent true infection with M. tuberculosis (39,316). Testing for infection with M. tuberculosis should be performed for well-defined groups at high risk. These groups can be divided into two categories: 1) persons at higher risk for exposure to and infection with M. tuberculosis and 2) persons at higher risk for progression from LTBI to TB disease (see TB Infection-Control Program for Settings in Which Patients with Suspected or Confirmed TB Disease Are Expected To Be Encountered; and TB Infection-Control Program for Settings in Which Patients with Suspected or Confirmed TB Disease Are Not Expected To Be Encountered).
Flexibility is needed in defining high-priority groups for TB screening. The changing epidemiology of TB indicates that the risk for TB among groups currently considered as high priority might decrease over time, and groups currently not identified originally as being at high risk might be considered as high priority.
Baseline Testing with BAMT
For the purposes of establishing a baseline, a single negative BAMT result is sufficient evidence that the HCW is probably not infected with M. tuberculosis (Box 2). However, cautions regarding making medical care decisions for persons whose conditions are at increased risk for progressing to TB disease from M. tuberculosis infection have been presented (Box 4).
If BAMT is used for baseline testing of HCWs, including those in settings that are low risk, one negative BAMT result is sufficient to demonstrate that the HCW is not infected with M. tuberculosis (Box 2). Perform and document the baseline BAMT result preferably within 10 days of starting employment. HCWs with positive baseline results should be referred for a medical and diagnostic evaluation to exclude TB disease and then treatment for LTBI should be considered in accordance with CDC guidelines. Persons with a positive BAMT result do not need to be tested again for surveillance. For HCWs who have indeterminate test results, providers should consult the responsible laboratorian for advice on interpreting the result and making additional decisions (383).
Serial Testing with BAMT for Infection-Control Surveillance
When using BAMT for serial testing, a conversion for administrative purposes is a change from a negative to a positive result (Box 3). For HCWs who have indeterminate test results, providers should consult the responsible laboratorian for advice on interpreting the result and making additional decisions (383). Persons with indeterminate results should not be counted for administrative calculations of conversion rates.
Exposure of HCWs and Patients to M. tuberculosis
Known and Presumed Exposure
For HCWs with known and presumed exposure to M. tuberculosis, administer a symptom screen and obtain the BAMT result. A BAMT conversion probably indicates recent M. tuberculosis infection; therefore, TB disease must be excluded. Experience with BAMT in contact investigations is limited. Specific attention is needed in the management of certain populations (e.g., infants and children aged <4 years and immunocompromised persons, including those who are HIV-infected) (Box 4).
If the symptom screen or the BAMT result is positive, the exposed person should be evaluated for TB disease promptly, which includes a chest radiograph. If TB disease is excluded, additional medical and diagnostic evaluation for LTBI is needed, which includes a judgment regarding the extent of exposure.
Performing QFT-G
The QFT-G should be performed as described in the product insert provided with the BAMT kit. This insert is also available from the manufacturer's website (http://www.cellestis.com).
Interpretation of BAMT Results and Referral for Evaluation
HCWs who meet the criteria for referral should have a medical and diagnostic evaluation (see Supplements, Estimating the Infectiousness of a TB Patient; Diagnostic Procedures for LTBI and TB Disease; and Treatment Procedures for LTBI and TB Disease). The factors affecting treatment decisions during medical and diagnostic evaluation by risk for infection with M. tuberculosis have been presented (Box 5). In addition, because BAMT and other indirect tests for M. tuberculosis infection are diagnostic aids, the test results must be interpreted in the context of epidemiologic, historical, physical, and diagnostic findings. A higher likelihood of infection, as estimated from historical or epidemiologic details (e.g., exposure to M. tuberculosis) or because of the presence of an illness consistent with TB disease, increases the predictive value of a positive result. Setting-based risk factors (e.g., the prevalence of TB disease in the setting) should be considered when making decisions regarding the diagnosis and treatment of LTBI.
Medical conditions that impair or alter immune function (Box 4) decrease the predictive value of a negative result, and additional diagnostic methods (e.g., bacteriology, radiography, and histology) are required as evidence before excluding M. tuberculosis infection when the BAMT result is negative. Medical evaluations can occur in different settings, including an occupational health clinic, local or state health department, hospital, or private medical clinic.
Indeterminate QFT-G results are reported for either of two test conditions.
The IFN-γ responses to all antigens (ESAT-6, CFP-10, and mitogen) are below a cut-off threshold. The weak response to mitogen could be caused by nonstandard storage or transportation of the blood sample, by laboratory errors, or by lymphocytic insensitivity caused by immune dysfunction.
OR,
The IFN-γ response to the Nil exceeds a specified threshold, and the responses to both ESAT-6 and CFP-10 do not exceed the response to Nil by at least 50%. This response could be caused by nonstandard storage or transportation, laboratory errors, or circulating IFN-γ, which can be increased in ill HCWs or patients. For HCWs who have indeterminate test results, providers should consult the responsible laboratorian for advice on interpreting the result and making further decisions (383).
Interpreting the BAMT Result for Infection Control and Surveillance
BAMT conversion rates should be determined routinely. The precision of the BAMT conversion rate will depend, in part, on the number of HCWs tested, which should be considered when establishing a regular interval for evaluation and monitoring of HCWs with BAMT. Health-care settings with a substantial number of HCWs might have testing schedules that can accurately determine the BAMT conversion rate each month (i.e., from annual results of an HCW cohort tested within the given month), if testing is staggered throughout the year. BAMT conversion rates are more difficult to calculate in settings with fewer test results.
QC Program for the BAMT
Multiple processes are necessary to assure quality BAMT results: specimen collection, transport and handling, and conducting the test in the laboratory. BAMT must meet performance parameters for a valid test result to be achieved. QC is an ongoing laboratory issue. The infection-control team should assist the laboratory in assuring that all requisite conditions are present. The laboratory performing the BAMT will be required to validate its performance of the test before processing clinical samples. State and federal laboratory requirements regulate laboratory-testing procedures.
Additional Considerations
An indeterminate QFT-G result does not mean that the test has failed; it indicates that the specimen has inadequate responsiveness for the test to be performed. This result might reflect the condition of the HCW or patient, who, for example, might be immunosuppressed. Alternatively, the specimen might have been handled incorrectly. For HCWs who have indeterminate test results, providers should consult the responsible laboratorian for advice on interpreting the result and making further decisions (383). Skin testing for cutaneous anergy is not useful in screening for asymptomatic LTBI or for diagnosing TB disease (339).
QFT-G use with HIV-infected persons taking ART. The effect of HIV infection and of ART on the performance of the QFT-G have not been fully evaluated.
Persons aged <17 years or pregnant women. The use of the QFT-G has not been evaluated in persons aged <17 years or pregnant women (35).
Booster phenomenon and BAMT. BAMT does not involve the injection of any substance into the persons being tested and is not affected by the booster phenomenon.
BCG vaccination. In the United States, vaccination with BCG is not routinely recommended (227). However, BCG is the most commonly used vaccine in the world. Foreign-born persons are commonly employed in the United States as HCWs. Previous BCG vaccination is not a contraindication to having a BAMT performed. BCG does not influence BAMT results with the version of the test approved in 2005 (i.e., QFT-G). HCWs who have received BCG vaccination should receive a baseline BAMT in the same manner as those without BCG vaccination, and the test result should be interpreted without reference to BCG.
Environmental Controls
Overview
Environmental controls include the following technologies to remove or inactivate M. tuberculosis: local exhaust ventilation, general ventilation, HEPA filtration, and UVGI. These controls help to prevent the spread and reduce the concentration of airborne infectious droplet nuclei. Environmental controls are the second line of defense in the TB infection-control program, and they work in harmony with administrative controls.
The reduction of exposures to M. tuberculosis can be facilitated through the effective use of environmental controls at the source of exposure (e.g., coughing patient or laboratory specimen) or in the general workplace environment. Source control is amenable to situations where the source has been identified and the generation of the contaminant is localized. Source-control techniques can prevent or reduce the spread of infectious droplet nuclei into the air by collecting infectious particles as they are released. These techniques are especially critical during procedures that will probably generate infectious aerosols (e.g., bronchoscopy, sputum induction, endotracheal intubation, suctioning, irrigating TB abscesses, aerosol treatments, autopsies on cadavers with untreated TB disease, and certain laboratory specimen manipulations) and when patients with infectious TB disease are coughing or sneezing.
Unsuspected and undiagnosed cases of infectious TB disease are believed to represent a substantial proportion of the current risk to HCWs (10,85). In such situations, source control is not a feasible option. Instead, general ventilation and air cleaning must be relied upon for control. General ventilation can be used to dilute the air and remove air contaminants and to control airflow patterns in rooms or in a health-care setting. Air-cleaning technologies include HEPA filtration to reduce the concentration of M. tuberculosis droplet nuclei and UVGI to kill or inactivate the microorganisms so that they no longer pose a risk for infection.
Ventilation systems for health-care settings should be designed, and modified when necessary, by ventilation engineers in collaboration with infection-control practitioners and occupational health staff. Recommendations for designing and operating ventilation systems have been published (117,118,178). The multiple types and conditions for use of ventilation systems in health-care settings and the needs of persons in these settings preclude the provision of extensive guidance in this document.
The information in this section is conceptual and intended to educate HCWs regarding environmental controls and how these controls can be used in the TB infection-control program. This information should not be used in place of consultation with experts who can give advice on ventilation system design, selection, installation, and maintenance. Because environmental controls will fail if they are not properly operated and maintained, routine training and education of staff are key components to a successful TB infection-control program. These guidelines do not specifically address mechanical ventilators in detail (see Intensive Care Units [ICUs]).
Local Exhaust Ventilation
Local exhaust ventilation captures airborne contaminants at or near their source and removes the contaminants without exposing persons in the area to infectious agents. This method is considered the most efficient way to remove airborne contaminants because it captures them before they can disperse. In local exhaust devices, hoods are typically used. Two types of hoods are 1) enclosing devices, in which the hood either partially or fully encloses the infectious source; and 2) exterior devices, in which the infectious source is near but outside the hood. Fully enclosed hoods, booths, or tents are always preferable to exterior devices because of their superior ability to prevent contaminants from escaping into the HCW's breathing space. Descriptions of both enclosing and exterior devices have been published (178).
Enclosing Devices
Enclosing devices for local exhaust ventilation include 1) booths for sputum induction or administration of aerosolized medications (Figure 2), 2) tents or hoods for enclosing and isolating a patient, and 3) BSCs (165). These devices are available in various configurations. The simplest device is a tent placed over the patient; the tent has an exhaust connection to the room-discharge exhaust system. The most complex device is an enclosure with a self-contained airflow and recirculation system (Figure 2).
Tents and booths should have sufficient airflow to remove at least 99% of airborne particles during the interval between the departure of one patient and the arrival of the next (Table 1). The time required to remove 99% or 99.9% of airborne particles from an enclosed space depends on 1) the number of ACH, which is a function of the volume (number of cubic feet of air) in the room or booth and the rate at which air is exiting the room or booth at the intake source; 2) the location of the ventilation inlet and outlet; and 3) the configuration of the room or booth. The surfaces of tents and booths should be periodically cleaned in accordance with recommendations and guidance from the manufacturers (see Supplement, Cleaning, Disinfecting, and Sterilizing Patient-Care Equipment and Rooms).
Exterior Devices
Exterior devices for local exhaust ventilation are usually hoods that are near to but not enclosing an infectious patient. The airflow produced by these devices should be sufficient to prevent cross-currents of air near the patient's face from allowing droplet nuclei to escape. Whenever possible, the patient should face directly into the opening of the hood to direct any coughing or sneezing into the hood. The device should maintain an air velocity of 200 feet per minute (fpm) at the patient's breathing zone to ensure the capture of droplet nuclei. Smoke tubes should be used to verify that the control velocity at the typical location of the patient's breathing zone is adequate to provide capture for the condition of highest expected cross-drafts and then the patient's breathing zone should be maintained at this location for the duration of the treatment.
Discharge of Exhaust from Booths, Tents, and Hoods
Air from booths, tents, and hoods is either discharged into the room in which the device is located or to the outside. If the exhaust air is discharged into the room, a HEPA filter should be incorporated at the discharge duct or vent of the device. The exhaust fan should be located on the discharge side of the HEPA filter to ensure that the air pressure in the filter housing and booth is negative compared with adjacent areas. Uncontaminated air from the room will flow into the booth through all openings, preventing infectious droplet nuclei in the booth from escaping into the room. Additional information on the installation, maintenance, and monitoring of HEPA filters is included in this report (Appendix A).
The majority of commercially available booths, tents, and hoods are fitted with HEPA filters; additional HEPA filtration is not needed with these devices. If a device does not incorporate a HEPA filter, the air from the device should be exhausted directly to the outside and away from air-intake vents, persons, and animals, in accordance with applicable federal, state, and local regulations on environmental discharges.
General Ventilation
General ventilation is used to 1) dilute and remove contaminated air, 2) control the direction of airflow in a health-care setting, and 3) control airflow patterns in rooms.
Dilution and Removal of Contaminated Air
General ventilation maintains air quality by both air dilution and removal of airborne contaminants. Uncontaminated supply air mixes with contaminated room air (dilution), and air is subsequently removed from the room by the exhaust system (removal). These processes reduce the concentration of droplet nuclei in the room air.
Ventilation systems for air dilution and removal. Two types of general ventilation systems are used to dilute and remove contaminated air: single-pass air systems and recirculating air systems.
In a single-pass air system, the supply air is either outside air that has been heated or cooled or air that is uncontaminated from a central system that supplies multiple areas. After air passes through the room or area, 100% of the air is exhausted to the outside. A single-pass system is the preferred choice for an AII room because the system prevents contaminated air from being recirculated to other areas of the health-care setting. In a recirculating air system, a limited portion of the exhaust air is discharged directly to the outside and replaced with fresh outside air, which mixes with the portion of exhaust air that was not discharged. If the resulting air mixture is not treated, it can contain a substantial proportion of contaminated air when it is recirculated to areas serviced by the system. This air mixture can be recirculated into the general ventilation, and infectious particles can be carried from contaminated areas to uncontaminated areas. Alternatively, the air mixture could be recirculated in a specific room or area so that other areas are not affected. The use of air-cleaning technologies for removing or inactivating infectious particles in recirculated air systems has been discussed (Appendix A).
Delivery of general ventilation. General ventilation is delivered by either constant air volume (CAV) systems or VAV systems. In general, CAV systems are best for AII rooms and other negative-pressure rooms because the negative-pressure differential is easier to maintain. VAV systems are acceptable if provisions are made to maintain the minimum mechanical and outside ACH and a negative pressure ≥0.01 inch of water gauge compared with adjacent areas at all times.
Ventilation rates. Recommended ventilation rates (air change rates) for health-care settings are usually expressed in numbers of ACH, which is the ratio of the volume of air entering the room per hour to the room volume. ACH equals the exhaust airflow (Q cubic feet per minute [cfm]) divided by the room volume (V cubic feet) multiplied by 60.
ACH = (Q ÷ V) x 60
Ventilation recommendations for selected areas in new or renovated health-care settings have been presented (Table 2). These recommendations have been adapted from those published by AIA (118). The feasibility of achieving a specific ventilation rate depends on the construction and operational requirements of the ventilation system and might differ for retrofitted and newly constructed facilities. The expense and effort of achieving a high ventilation rate might be reasonable for new construction but less reasonable when retrofitting an existing setting.
In existing settings, air-cleaning technologies (e.g., fixed or portable room-air recirculation units [also called portable air cleaners] or UVGI) can be used to increase the equivalent ACH. This equivalent ventilation concept has been used to compare microbial inactivation by UVGI with particle-removal by mechanical ventilation (384,385) and to compare particle removal by HEPA filtration of recirculated air with particle removal by mechanical ventilation. The equivalent ventilation approach does not, however, negate the requirement to provide sufficient fresh outside air for occupant comfort (Table 2).
To dilute the concentration of normal room-air contaminants and minimize odors, a portion of the supply air should come from the outdoors (Table 2). Health-care settings should consult the American Society of Heating, Refrigerating, and Air-Conditioning Engineers, Inc. (ASHRAE), Standard 62.1, Ventilation for Acceptable Indoor Air Quality, for outside air recommendations in areas not listed in this report (386).
Control of Airflow Direction in a Health-Care Setting
Airflow direction is controlled in health-care settings to contain contaminated air and prevent its spread to uncontaminated areas.
Directional airflow. The general ventilation system should be designed and balanced so that air flows from less contaminated (more clean) to more contaminated (less clean) areas (118,117). For example, air should flow from corridors (cleaner areas) into AII rooms (less clean areas) to prevent the spread of contaminants. In certain rooms in which surgical and invasive procedures are performed and in protective environment (PE) rooms, the direction of airflow should be from the room to the hallway. Environmental control recommendations for situations involving the care and treatment of patients with TB disease in ORs and PE rooms have been presented (see Other Selected Settings). Cough-inducing or aerosol-generating procedures should not be performed on patients with suspected or confirmed TB disease in rooms where air flows from the room to the hallway.
Negative pressure for achieving directional airflow. The direction of airflow is controlled by creating a lower (negative) pressure in the area into which the flow of air is desired. Negative pressure is the approximate air-pressure difference between two areas in a health-care setting. For air to flow from one area to another, the air pressure in the two areas must be different. Air will flow from a higher pressure area to a lower pressure area. A room that is under negative pressure has a lower pressure than adjacent areas, which keeps air flowing from the adjacent rooms or areas into the room. Negative pressure is achieved by exhausting air at a higher volumetric rate than the rate that the air is being supplied.
Control of Airflow Patterns in Rooms
General ventilation systems should be designed to provide controlled patterns of airflow in rooms and to prevent air stagnation or short-circuiting of air from the supply to the exhaust (i.e., passage of air directly from the air supply to the exhaust). To provide controlled airflow patterns, the air supply and exhaust should be located so that clean air flows first to parts of the room where HCWs probably work and then across the infectious source and into the exhaust. Therefore, HCWs are not positioned between the infectious source and the exhaust. This configuration is not always possible but should be used whenever feasible.
One way to achieve a controlled airflow pattern is to supply air at the side of the room opposite the patient and exhaust it from the side where the patient is located (Figure 3). Another method, which is most effective when the supply air is cooler than the room air, is to supply air near the ceiling and exhaust it near the floor (Figure 3). Care must be taken to ensure that furniture or moveable equipment does not block the low exhausts. Airflow patterns are affected by air temperature differentials, location of the supply diffusers and exhaust grilles, location of furniture, movement of HCWs and patients, and the configuration of the space.
If the room ventilation is not designed for a plug-flow type of airflow pattern (Figure 3), then adequate mixing must be maintained to minimize air stagnation. The majority of rooms with properly installed supply diffusers and exhaust grilles will have adequate mixing. A qualitative measure of mixing is the visualization of air movement with smoke tubes at multiple locations in the room. Smoke movement in all areas of the room indicates good mixing. Additional sophisticated studies can be conducted by using a tracer gas to quantify air-mixing and air-exchange rates.
If areas of air stagnation are present, air mixing can be improved by adding a circulating fan or repositioning the supply and exhaust vents. Room-air recirculation units positioned in the room or installed above the ceiling can also improve air mixing. If supply or exhaust vents, circulating fans, or room-air recirculation units are placed incorrectly, HCWs might not be adequately protected.
Achieving Negative Pressure in Rooms
Negative pressure is needed to control the direction of airflow between selected rooms in a health-care setting and their adjacent spaces to prevent contaminated air from escaping from the room into other areas (118) (Figure 4). Control of a room's differential airflow and total leakage area is critical to achieving and maintaining negative pressure. Differential airflow, differential pressure, and leakage area are interrelated. This relation is illustrated (Figure 4) and is expressed in an empirical equation (387).
AE = 0.01138 * (∆Q 1.170/∆P0.602)
In the equation, AE is the leakage area in square inches; ∆Q is the differential airflow rate in cfm; and ∆P is the differential pressure drop in inches of water gauge. This empirical equation was used (Figure 4), which indicates that changing one parameter will influence one or both of the other parameters. For example, the control of differential pressure can frequently be improved by increasing the air tightness or seal of a room, maintaining the HVAC system, and ensuring continuous monitoring. In a room that is already substantially tight (e.g., with 10 square inches of leakage), however, a small change in differential pressure will have a substantial effect on differential airflow. Similarly, a room with a more substantial leakage area (e.g., 300 square inches of leakage) requires a higher differential airflow rate to achieve a pressure differential of 0.01 inch of water gauge. Reducing the leakage in a room with 300 square inches of leakage can help achieve a pressure differential of 0.01 inch of water gauge (Figure 4). If the leakage area is reduced to approximately 40 square inches, a pressure differential of 0.01 inch of water gauge can be achieved by exhausting approximately 100 cubic feet per minute (cfm) more air from the room than is supplied to the room.
Room leakage can occur through cracks or spaces near doors, windows, ceiling, and utility connections. Steps should be taken to minimize these leaks. Changes in the performance of the HVAC system will affect the pressure differential in a room and can potentially cause a negative-pressure room to become positive-pressure. Therefore, each of these parameters requires close monitoring to ensure that minor changes in the performance of the HVAC system do not adversely affect the entire system (388,389).
Pressure differential. To achieve negative pressure in a room that has a normally functioning ventilation system, first measure and balance the supply and exhaust airflows to achieve an exhaust flow higher than the supply flow. Next, measure the pressure differential across the closed door. Although the minimum pressure difference needed for airflow into a room is substantially small (approximately 0.001 inch of water gauge), a pressure differential of ≥0.01 inch of water gauge (≥2.5 Pascals [Pa]) is recommended. This higher pressure differential is easier to measure and offers a margin of safety for maintaining negative pressure as the pressure in surrounding areas changes because of the opening and closing of doors, operation of elevators, stack effect (rising of warm air, similar to a chimney), ventilation system fluctuations, and other factors. The higher pressurization value is consistent with the most recent AIA recommendations for airborne precautions in health-care settings (118) and is the generally accepted level of negative pressurization for microbiology and biomedical laboratories (390).
Opening doors and windows can substantially affect the negative pressure in an AII room. Infection-control criteria requires AII room windows and doors to remain closed, except when doors must be opened for persons to enter or leave the room. Keeping certain doors in the corridor outside the AII rooms closed might be necessary to maintain the negative-pressure differential between an AII room and the corridor. Pressurization cannot be maintained in rooms or spaces that are not enclosed.
If ≥0.01 inch of water gauge is not achieved and cannot be achieved by increasing the flow differential (within the limits of the ventilation system), the room should be inspected for leakage. The total room leakage is based on the previously measured pressure, and air flow differentials can be estimated (Figure 4). If the room leakage is too substantial (e.g., 300 square inches), maintaining a negative-pressure differential as high as 0.01 inch of water gauge might be difficult. A lower value is acceptable if air-pressure monitoring indicates that negative pressure is always maintained (or airflow indicators consistently demonstrate that air is flowing in the desired direction). If negative pressure cannot be maintained, the leakage area might need to be reduced by sealing cracks around windows or replacing porous suspended ceiling panels with gasketed or sealed solid panels.
Because negative pressure in an AII room can be affected by even minimal changes in the operation of the ventilation system, negative pressure can be difficult to maintain with a VAV ventilation system. To maintain negative pressure, a VAV supply system should be coupled with a compensating exhaust system that increases when the supply flow rate increases. Alternatively, the exhaust can be set at a fixed rate that ensures negative pressure throughout the VAV supply cycle. The VAV minimum flow rate must also be adequate to maintain the recommended minimum mechanical and outdoor ACH (Table 2).
Alternate methods for achieving negative pressure. An anteroom is not a substitute for negative pressure in an AII room. However, an anteroom can reduce the escape of droplet nuclei during the opening and closing of the door to an AII room and can buffer an AII room from pressure fluctuations in the corridor. To function properly, an anteroom must have more air exhausted from the room than supplied to remove M. tuberculosis that can enter from the AII room. An anteroom can also have its own supply diffuser, if needed, to balance the pressure with the corridor. If an anteroom is unventilated or not properly ventilated, it will function only as a lesser contaminated vestibule between the AII room and the corridor and might not prevent the escape of droplet nuclei into the corridor. To adjust airflow and pressure differentials, health-care settings should consult a ventilation engineer who is knowledgeable regarding all applicable regulations, including building fire codes.
If the desired negative pressure cannot be achieved because a room does not have a separate ventilation system or a system that can provide the proper airflow, steps should be taken to provide a method to discharge air from an AII room. One method to achieve negative pressure in a room is to add a supplemental exhaust unit. If an AII room has a window or an outside wall, a small exhaust fan can be used. An engineer should be consulted to evaluate the potential for negative effects on surrounding areas (e.g., disruption of exhaust airflow in adjoining bathrooms) and to ensure the provision of the recommended amounts of outdoor air. The exhaust must not be discharged where it can immediately re-enter the building or pose a hazard to persons outside.
Fixed room-air recirculation systems (i.e., systems that recirculate the air in an entire AII room) can be designed to achieve negative pressure by discharging a portion of the air to the outside. Some portable room-air recirculation units are also designed to discharge air to the outside to achieve negative pressure. These air cleaners must be designed specifically for this purpose.
Monitoring negative pressure. Negative pressure must be monitored to ensure that air is always flowing from the corridor (or surrounding area) into the AII room. Negative pressure can be monitored either continuously or periodically. Monitoring methods include chemical aerosols (e.g., smoke tube), differential pressure-sensing devices (e.g., manometer), and physical indicators (e.g., flutter strips).
A chemical aerosol resembling smoke can be used to observe airflow between a room and the surrounding area, or within a room. Devices called smoke tubes generate the chemical aerosol resembling smoke, which follows the local air currents wherever it is released. To check the negative pressure in a room, hold a smoke tube approximately 2 inches in front of the base of the closed door of the AII room or in front of the air transfer grille, if the door has such a feature. Hold the smoke tube parallel to the door. A small amount of smoke should be generated slowly to ensure that the velocity of smoke emanating from the tube does not overpower the air velocity (Figure 5). If the room is under negative pressure, the smoke will travel into the room (from higher to lower pressure). If the room is not under negative pressure, the smoke will be blown outward or stay in front of the door. Room air cleaners in the room should be operating. Persons using smoke tubes should avoid inhaling the smoke, because direct inhalation of high concentrations of the smoke can be irritating (391) (Figure 5).
Manometers are used to monitor negative pressure. They provide either periodic (noncontinuous) pressure measurements or continuous pressure monitoring. A continuous monitoring indicator can simply be a visible or audible warning signal indicating that air pressure is positive. Both periodic and continuous pressure detectors generate a digital or analog signal that can be recorded for later verification or used to automatically adjust the room's ventilation control system.
Physical indicators (e.g., flutter strips) are occasionally used to provide a continuous visual sign that a room is under negative pressure. These simple and inexpensive devices are placed directly in the door and can be useful in identifying a pressure differential problem.
Pressure-measuring devices should sense the pressure just inside the airflow path into the AII room (e.g., at the base of the door). Unusual airflow patterns can cause pressure variations. For example, the air can be under negative pressure at the middle of a door and under positive pressure at the base of the same door. The ideal location of a pressure-measuring device has been illustrated (Figure 6). If the pressure-sensing ports of the device cannot be located directly across the airflow path, validating that the negative pressure at the sensing point is and remains the same as the negative pressure across the flow path might be necessary.
Pressure-sensing devices should incorporate an audible warning with a time delay to indicate an open door. When a door is open, the negative pressure cannot be maintained, but this situation should not generate an alarm unless the door is left open. Therefore, the time delay should allow adequate time for persons to enter or leave an AII room without activating the alarm.
The pressure differentials used to achieve low negative pressure (<0.005 inch) require the use of substantially sensitive mechanical devices, electronic devices, or pressure gauges to ensure accurate measurements. Pressure-measuring and monitoring devices can give false readings if the calibration has drifted. For example, a sensor might indicate that the room pressure is slightly negative compared with the corridor, but, because air current momentum effects or "drift" of the electrical signal, air might actually be flowing out of the AII room through the opening at the base of the door. In one study of 38 AII rooms with electrical or mechanical devices to continuously monitor air pressurization, one half had airflow at the door in the opposite direction of that indicated by the continuous monitors (392). The investigators attributed this problem to instrument limitations and device malfunction. A negative pressure differential of ≥0.01 inch of water gauge (compared with the previously recommended 0.001 inch of water gauge) might help to minimize this problem.
Periodic checks are required to maintain the desired negative pressure and the optimal operation of monitoring devices.
AII rooms should be checked for negative pressure before occupancy.
When occupied by a patient, an AII room should be checked daily with smoke tubes or other visual checks for negative pressure.
If pressure-sensing devices are used in AII rooms occupied by patients with suspected or confirmed TB disease, negative pressure should be checked daily by using smoke tubes or other visual checks.
If the AII rooms are not being used for patients who have suspected or confirmed TB disease but potentially could be used for such patients, the negative pressure should be checked monthly.
Laboratories should be checked daily for negative pressure.
AII Rooms and Other Negative-Pressure Rooms
AII rooms are used to 1) separate patients who probably have infectious TB from other persons, 2) provide an environment in which environmental factors are controlled to reduce the concentration of droplet nuclei, and 3) prevent the escape of droplet nuclei from such rooms into adjacent areas using directional airflow. Other negative-pressure rooms include bronchoscopy suites, sputum induction rooms, selected examination and treatment rooms, autopsy suites, and clinical laboratories.
Preventing the escape of droplet nuclei. AII rooms used for TB isolation should be single-patient rooms with negative pressure, compared with the corridor or other areas connected to the room. Opening doors and windows can substantially affect the negative pressure in an AII room. Infection-control criteria require AII room windows and doors to remain closed, except when doors must be opened for persons to enter or leave the room. It might also be necessary to keep certain doors in the corridor outside the AII rooms closed to maintain the negative-pressure differential between an AII room and the corridor. The use of self-closing doors is recommended. The openings in the room (e.g., windows, and electrical and plumbing entries) should be sealed as much as possible, with the exception of a small gap (1/8–1/2 inch) at the base of the door to provide a controlled airflow path. Proper use of negative pressure will prevent contaminated air from escaping the room (393,394).
Reducing the concentration of droplet nuclei. AII rooms in existing health-care settings should have an air change rate of ≥6 mechanical ACH. Whenever feasible, this airflow rate should be increased to ≥12 mechanical ACH by adjusting or modifying the ventilation system or should be increased to ≥12 equivalent ACH by supplementing with air-cleaning technologies (e.g., fixed or portable room-air recirculation systems or UVGI systems). New construction or renovation of existing health-care settings should be designed so that AII rooms achieve a total air change rate of ≥12 mechanical ACH. These recommendations are consistent with guidelines by ASHRAE and AIA that recommend ≥12 mechanical ACH for AII rooms (117,118). Ventilation recommendations for other negative-pressure rooms in new or renovated health-care settings have been presented (see Risk Classification Examples).
To dilute the concentration of normal room air contaminants and minimize odors, a portion of the supply air should come from the outdoors. A minimum of 2 ACH of outdoor air should be provided to AII rooms and other negative-pressure rooms (117,118).
Exhaust from AII rooms and other negative-pressure rooms. Air from AII rooms and other negative-pressure rooms for patients with suspected or confirmed TB disease should be exhausted directly to the outside and away from air-intake vents, persons, and animals, in accordance with applicable federal, state, and local regulations on environmental discharges. Exhaust ducts should be located away from sidewalks or windows that can be opened. Ventilation system exhaust discharges and inlets should be designed to prevent the re-entry of exhausted air. Wind blowing over a building creates a substantially turbulent recirculation zone that can cause exhausted air to re-enter the building. Exhaust flow should be discharged above this zone. Design guidelines for proper placement of exhaust ducts have been published (395). If recirculation of air from such rooms into the general ventilation system is unavoidable, the air should be passed through a HEPA filter before recirculation.
Alternatives to negative-pressure rooms. AII can also be achieved by the use of negative-pressure enclosures (e.g., tents or booths). These enclosures can provide patient isolation in EDs and medical testing and treatment areas and can supplement AII in designated negative-pressure rooms.
Other Selected Settings
Operating rooms, autopsy suites, sputum-induction rooms, and aerosolized treatment rooms pose potential hazards from infectious aerosols generated during procedures on patients with TB disease (72,90,396–398). Recommended administrative, environmental, and respiratory-protection controls for these and other selected settings have been summarized (Appendix A). Additional or specialized TB infection controls that are applicable to special circumstances and types of health-care delivery settings have also been described (see Managing Patients Who Have Suspected or Confirmed TB Disease: Considerations for Special Circumstances and Settings). Ventilation recommendations for these settings in new or renovated health-care facilities have been included in this report (Table 2). Existing facilities might need to augment the current ventilation system or use the air-cleaning methods to increase the number of equivalent ACH.
Patients with TB disease who also require a PE room (e.g., severely immunocompromised patients) are special cases. These patients require protection from common airborne infectious microorganisms and must be placed in a room that has HEPA-filtered supply air and is under positive pressure compared with its surroundings (118). If an anteroom is not available, the use of other air-cleaning methods should be considered to increase the equivalent ACH. The air-cleaning systems can be placed in the room and in surrounding areas to minimize contamination of the surroundings. Similar controls can be used in ORs that are used for patients with TB disease because these rooms must be maintained under positive pressure, compared with their surroundings to maintain a sterile field.
Air-Cleaning Methods
HEPA Filtration
HEPA filtration can be used to supplement other recommended ventilation measures by providing a minimum removal efficiency of 99.97% of particles equal to 0.3 µm in diameter. This air-cleaning method is considered an adjunct to other ventilation measures. Used alone, this method neither provides outside air for occupant comfort nor satisfies other recommended ventilation measures (e.g., using source control whenever possible and minimizing the spread of contaminants in a setting through control of airflow patterns and pressure differentials).
HEPA filters have been demonstrated to reduce the concentration of Aspergillus spores (range in size: 5–6 µm) to below measurable levels (399–401). Because infective droplet nuclei generated by TB patients are believed to range from 1–5 µm in diameter (300) (comparable in size to Aspergillus spores) (402), HEPA filters will remove M. tuberculosis–containing infectious droplet nuclei from contaminated air. HEPA filters can be used to clean air before it is 1) exhausted to the outside, 2) recirculated to other areas of a health-care setting, or 3) recirculated in an AII room. Because electrostatic filters can degrade over time with exposure to humid environments and ambient aerosols (403), their use in systems that recirculate air back into the general ventilation system from AII rooms and treatment rooms should be avoided. If used, the filter manufacturer should be consulted regarding the performance of the filter to ensure that it maintains the desired filtration efficiency over time and with loading.
Use of HEPA filtration when exhausting air to the outside. HEPA filters can be used as an added safety measure to clean air from AII rooms and local exhaust devices (e.g., booths, tents, and hoods) before exhausting it to the outside. This added measure is not necessary, however, if the exhaust air cannot re-enter the ventilation system supply and does not pose a risk to persons and animals where it is exhausted.
Exhaust air frequently is not discharged directly to the outside; instead, the air is directed through heat-recovery devices (e.g., heat wheels or radiator-like devices). Heat wheels are frequently used to reduce the costs of operating ventilation systems (404). As the wheel rotates, energy is transferred into or removed from the supply inlet air stream. If a heat wheel is used with a system, a HEPA filter should also be used. The HEPA filter should be placed upstream from the heat wheel because of the potential for leakage across the seals separating the inlet and exhaust chambers and the theoretical possibility that droplet nuclei might be impacted on the wheel by the exhaust air and subsequently stripped off into the supply air.
Recirculation of HEPA-filtered air. Air from AII rooms and other negative-pressure rooms should be exhausted directly to the outside. In certain instances, however, recirculation of air into the general ventilation system from such rooms is unavoidable (e.g., settings in which the ventilation system or building configuration causes venting the exhaust to the outside impossible). In such cases, HEPA filters should be installed in the exhaust duct exiting the room to remove infectious organisms from the air before it is returned to the general ventilation system.
Individual room-air recirculation can be used in areas in which no general ventilation system exists, where an existing system is incapable of providing sufficient ACH, or where air-cleaning (particulate removal) is desired without affecting the fresh air supply or negative-pressure system. Recirculation of HEPA-filtered air in a room can be achieved by 1) exhausting air from the room into a duct, passing it through a HEPA filter installed in the duct, and returning it to the room (Figure 7); 2) filtering air through HEPA recirculation systems installed on the wall or ceiling of the room (Figure 8); or 3) filtering air through portable HEPA recirculation systems. In this report, the first two approaches are referred to as fixed room-air recirculation systems because the recirculation systems are not easily movable.
Fixed room-air recirculation systems. The preferred method of recirculating HEPA-filtered air is by using a built-in system in which air is exhausted from the room into a duct, filtered through a HEPA filter, and returned to the room (Figure 7). This technique can add equivalent ACH in areas in which the recommended minimum ACH is difficult to meet with general ventilation. This equivalent ventilation concept compares particle removal by HEPA filtration of the recirculated air with particle clearance from exhaust ventilation. Because the air does not have to be conditioned, airflow rates that are higher than those produced by the general ventilation system can usually be achieved. An alternative is to install HEPA filtration units on the wall or ceiling (Figure 8).
Fixed recirculation systems are preferred to portable (free-standing) units because they can be installed with a higher degree of reliability. In addition, certain fixed systems have a higher airflow capacity than portable systems, and the potential for short-circuiting of air is reduced as the distance between the air intake and exhaust is increased.
Portable room-air recirculation systems. Portable room-air recirculation units with HEPA filters (also called portable air cleaners) can be considered when 1) a room has no general ventilation system, 2) the system cannot provide adequate ACH, or 3) increased effectiveness in airflow is needed. Effectiveness depends on the ability of the portable room-air recirculation unit to circulate as much of the air in the room as possible through the HEPA filter. Effectiveness can vary depending on the room's configuration, the furniture and persons in the room, the placement of the HEPA filtration unit compared with the supply diffusers and exhaust grilles, and the degree of mixing of air within the room.
Portable room-air recirculation units have been demonstrated to be effective in removing bioaerosols and aerosolized particles from room air (405–410). Findings indicate that various commercially available units are useful in reducing the concentration of airborne particles and are therefore helpful in reducing airborne disease transmission. The performance of 14 units was evaluated for volumetric airflow, airborne particle reduction, noise level, and other parameters (406). The range of volumetric airflow rates was 110 cfm–1,152 cfm, and the equivalent ACH range was an average of 8–22 in a standard-sized, substantially well-mixed, single-patient room. Recommendations were provided to make subsequent models safer, more effective, quieter, and easier to use and service. Purchasers should be aware that the majority of manufacturer specifications indicated flow rates of free-wheeling fans and not the fan under the load of a filter.
Portable HEPA filtration units should be designed to 1) achieve ≥12 equivalent ACH, 2) ensure adequate air mixing in all areas of the rooms, and 3) be compatible with the ventilation system. An estimate of the ability of the unit to circulate the air in a room can be made by visualizing airflow patterns (estimating room air mixing [see Supplements, Environmental Controls; and General Ventilation]). If the air movement is adequate in all areas of the room, the unit should be effective.
If portable devices are used, units with high volumetric airflow rates that provide maximum flow through the HEPA filter are preferred. Placement should be selected to optimize the recirculation of AII room air through the HEPA filter. Careful consideration must be given to obstacles (e.g., furnishings, medical equipment, and walls) that could disrupt airflow and to system specifications (e.g., physical dimensions, airflow capacity, locations of air inlet and exhaust, and noise) to maximize performance of the units, minimize short-circuiting of air, and reduce the probability that the units will be switched off by room occupants.
Installing, maintaining, and monitoring HEPA filters. The performance of HEPA filters depends on proper installation, testing, and meticulous maintenance (411), especially if the system recirculates air to other parts of the health-care setting. Improper design, installation, or maintenance could allow infectious particles to circumvent filtration and escape into the general ventilation system (117). These failures also could impede proper ventilation performance.
HEPA filters should be installed to prevent leakage between filter segments and between the filter bed and its frame. A regularly scheduled maintenance program is required to monitor filters for possible leakage and filter loading. A quantitative filter performance test (e.g., the dioctyl phthalate penetration test [412,413]) should be performed at the initial installation and each time the filter is changed. Records should be maintained for all filter changes and testing. A leakage test using a particle counter or photometer should be performed every 6–12 months for filters in general-use areas and in areas with systems that will probably be contaminated with M. tuberculosis (e.g., AII rooms).
A manometer or other pressure-sensing device should be installed in the filter system to provide an accurate and objective means of determining the need for filter replacement. Pressure-drop characteristics of the filter are supplied by the manufacturer. Installation of the filter should allow for maintenance that will not contaminate the delivery system or the area served. For general infection-control purposes, special care should be taken to avoid jarring or dropping the filter element during or after removal.
The scheduled maintenance program should include procedures for installation, removal, and disposal of filter elements. HEPA filter maintenance should be performed only by adequately trained personnel and only while the ventilation system or room-air recirculation unit is not being operated.
Laboratory studies indicate that re-aerosolization of viable mycobacteria from filter material (HEPA filters and N95 disposable respirator filter media) is not probable under normal conditions (414–416). Although these studies indicate that M. tuberculosis becoming an airborne hazard is not probable after it is removed by a HEPA filter (or other high efficiency filter material), the risks associated with handling loaded HEPA filters in ventilation systems under field-use conditions have not been evaluated. Therefore, persons performing maintenance and replacing filters on any ventilation system that is probably contaminated with M. tuberculosis should wear a respirator (see Respiratory Protection) in addition to eye protection and gloves. When feasible, HEPA filters can be disinfected in 10% bleach solution or other appropriate mycobacteriacide before removal (417). In addition, filter housing and ducts leading to the housing should be labeled clearly with the words "TB-Contaminated Air" or other similar warnings. Disposal of filters and other potentially contaminated materials should be in accordance with applicable local or state regulations.
One or more lower-efficiency disposable pre-filters installed upstream can extend the life of a HEPA filter by at least 25%. If the disposable filter is replaced by a 90% extended surface filter, the life of the HEPA filter can be extended by approximately 900% (178). Pre-filters should be handled and disposed of in the same manner as the HEPA filter.
UVGI
Ultraviolet germicidal irradiation (UVGI) is a form of electromagnetic radiation with wavelengths between the blue region of the visible spectrum and the radiograph region. UV-C radiation (short wavelengths; range: 100–280 nm) (418) can be produced by various artificial sources (e.g., arc lamps and metal halide lamps). The majority of commercially available UV lamps used for germicidal purposes are low-pressure mercury vapor lamps that emit radiant energy in the UV-C range, predominantly at a wavelength of 253.7 nm (418).
Research has demonstrated that UVGI is effective in killing or inactivating M. tuberculosis under experimental conditions (292,385,419–423) and in reducing transmission of other infectious agents in hospitals (424), military housing (425), and classrooms (426–428). Because of the results of multiple studies (384,429–432) and the experiences of clinicians and mycobacteriologists during the preceding decades, UVGI has been recommended as a supplement or adjunct to other TB infection-control and ventilation measures in settings in which the need to kill or inactivate M. tuberculosis is essential (6,7,196,433,434). UVGI alone does not provide outside air or circulate interior air, both of which are essential in achieving acceptable air quality in occupied spaces.
Applications of UVGI. UVGI is considered a method of air cleaning because it can kill or inactivate microorganisms so that they are no longer able to replicate and form colonies. UVGI is not a substitute for HEPA filtration before exhausting the air from AII rooms back into the general circulation. UVGI lamps can be placed in ducts, fixed or portable room air-recirculation units, or upper-air irradiation systems. The use of this air-cleaning technique has increased, particularly in substantial open areas in which unsuspected or undiagnosed patients with TB disease might be present (e.g., ED waiting rooms, shelters, and correctional facilities), and the costs of conditioning substantial volumes of outdoor air are prohibitive.
For each UVGI system, guidelines should be followed to maximize effectiveness. Effectiveness can be expressed in terms of an equivalent air change rate (427,435–437), comparing the ability of UVGI to inactivate organisms with removal through general ventilation. Initially, understanding and characterizing the application for which UVGI will be used is vital. Because the effectiveness of UVGI systems will vary, the use of UVGI must be carefully evaluated and the level of efficacy clearly defined and monitored.
The effective use of UVGI is associated with exposure of M. tuberculosis, as contained in an infectious droplet, to a sufficient dose of UV-C radiation at 253.7 nm to ensure inactivation. Because dose is a function of irradiance and time, the effectiveness of any application is determined by its ability to deliver sufficient irradiance for enough time to result in inactivation of the organism within the infectious droplet. Achieving a sufficient dose can be difficult with airborne inactivation because the exposure time can be substantially limited; therefore, attaining sufficient irradiance is essential.
The number of persons who are properly trained in the design and installation of UVGI systems is limited. One critical recommendation is that health-care facility managers consult a UVGI system designer to address safety and efficacy considerations before such a system is procured and installed. Experts who can be consulted include industrial hygienists, engineers, and health physicists.
Duct irradiation. Duct irradiation is designed to kill or inactivate M. tuberculosis without exposing persons to UVGI. In duct irradiation systems, UVGI lamps are placed inside ducts to disinfect the exhaust air from AII rooms or other areas in which M. tuberculosis might be present before it is recirculated to the same room (desirable) or to other areas served by the system (less desirable). When UVGI duct systems are not properly designed, installed, and maintained, high levels of UVGI can be produced in the duct that can potentially cause high UVGI exposures during maintenance operations.
Duct-irradiation systems depend on the circulation of as much of the room air as possible through the duct. Velocity profiles and mixing are important factors in determining the UVGI dose received by airborne particles. Design velocity for a typical UVGI unit is approximately 400 fpm (438). The particle residence time must be sufficient for inactivation of the microorganisms.
Duct irradiation can be used in three ways.
Ventilation systems serving AII rooms to recirculate air from the room, through a duct containing UV lamps, and back into the same room. UVGI duct systems should not be used either in place of HEPA filters, if air from AII rooms must be recirculated to other areas of a setting, or as a substitute for HEPA filtration of air from booths, tents, or hoods used for cough-inducing or aerosol-generating procedures.
Return air ducts serving patient rooms, waiting rooms, EDs, and general-use areas in which patients with undiagnosed TB disease could potentially contaminate the recirculated air.
Recirculating ventilation systems serving rooms or areas in which ceiling heights are too low for the safe and effective use of upper-air UVGI.
Upper-air irradiation. In upper-air irradiation, UVGI lamp fixtures are suspended from the ceiling and installed on walls. The base of the lamps are shielded to direct the radiation upward and outward to create an intense zone of UVGI in the upper air while minimizing the levels of UVGI in the lower part of the room where the occupants are located. The system depends on air mixing to move the air from the lower part of the room to the upper part where microbial-contaminated air can be irradiated.
A major consideration is the placement of UVGI fixtures to achieve sufficient irradiance of the upper-air space. The ceiling should be high enough (≥8 feet) for a substantial volume of upper air to be irradiated without overexposing occupants in the lower part of the room to UVGI. System designers must consider the mechanical ventilation system, room geometry, and emission characteristics of the entire fixture.
Upper-air UVGI can be used in various settings.
AII rooms and rooms in which aerosol-generating or aerosol-producing procedures (e.g., bronchoscopy, sputum induction, and administration of aerosolized medications) are performed.
Patient rooms, waiting rooms, EDs, corridors, central areas, and other substantial areas in which patients with undiagnosed TB disease could potentially contaminate the air.
Operating rooms and adjacent corridors where procedures are performed on patients with TB disease.
Medical settings in correctional facilities.
Portable room air recirculation systems. In portable room air-recirculation units containing UVGI, a fan moves a volume of room air across UVGI lamps to disinfect the air before it is recirculated back to the room. Some portable units contain both a HEPA filter (or other high efficiency filter) and UVGI lamps.
In addition to the guidelines described for the use of portable room air-recirculation systems containing HEPA filtration, consideration must be given to the volume of room air that passes through the unit, the UVGI levels, particle residence time, and filtration efficiency (for devices with a filter). One study in which a bioaerosol chamber was used demonstrated that portable room air cleaners with UVGI lamps as the primary air-cleaning mechanism are effective (>99%) in inactivating or killing airborne vegetative bacteria (439). Additional studies need to be performed in rooms with portable air cleaners that rely only on UVGI for air cleaning.
Portable room air cleaners with UVGI can be used in 1) AII rooms as an adjunct method of air cleaning and 2) waiting rooms, EDs, corridors, central areas, or other substantial areas in which patients with undiagnosed TB disease could potentially contaminate the air.
Effectiveness of UVGI. Air mixing, air velocity, relative humidity, UVGI intensity, and lamp configuration affect the efficacy of all UVGI applications. For example, with upper-air systems, airborne microorganisms in the lower, occupied areas of the room must move to the upper part of the room to be killed or inactivated by upper-air UVGI. Air mixing can occur through convection caused by temperature differences, fans, location of supply and exhaust ducts, or movement of persons.
Air-mixing. UVGI has been demonstrated to be effective in killing bacteria in the upper-air applications under conditions in which air mixing was accomplished primarily by convection. In a 1976 study on aerosolization of M. bovis BCG (a surrogate for M. tuberculosis) in a room without mechanical ventilation that relied primarily on convection and infiltration resulted in 10–25 equivalent ACH, depending on the number of UVGI fixtures used (384). Other early studies examined the effect of air-mixing on UVGI efficacy (440,441). These studies indicated that the efficacy of UVGI was substantially increased if cold supply air relative to the lower portion of the room entered through diffusers in the ceiling. The findings indicated that substantial temperature gradients between the upper and lower portions of the room favored (cold air in the upper portion of the room) or inhibited (hot air in the upper portion of the room) vertical mixing of air between the two zones.
When large-bladed ceiling fans were used to promote mixing in the experimental room, the ability of UVGI to inactivate Serratia marcescens, an organism known to be highly sensitive to UVGI, was doubled (442,443). Similar effects were reported in studies conducted during 2000–2002 in which louvered UVGI fixtures were used. One study documented an increase in UVGI effectiveness of 16% at 2 ACH and 33% at 6 ACH when a mixing fan was used (444). Another study conducted in a simulated health-care room determined that 1) at 0 ACH, a high degree of efficacy of upper-air UVGI was achieved in the absence or presence of mixing fans when no temperature gradient was created; and 2) at 6 ACH, bringing in warm air at the ceiling resulted in a temperature gradient with cooler room air near the floor and a UVGI efficacy of only 9% (422). Turning on box fans under these winter conditions increased UVGI efficacy nearly 10-fold (to 89%) (445).
To reduce variability in upper-air UVGI efficacy caused by temperature gradients in the room, a fan should be routinely used to continually mix the air, unless the room has been determined to be well mixed under various conditions of operation. Use of a fan would also reduce or remove the variable winter versus summer ACH requirements for optimal upper-air UVGI efficacy (446).
Relative humidity. In studies conducted in bioaerosol chambers, the ability of UVGI to kill or inactivate microorganisms declined substantially when the relative humidity exceeded 60% (447–450). In room studies, declines in the ability of upper-air UVGI to kill or inactivate microorganisms at high relative humidity (65%, 75%, and 100%) (384,422) have also been reported. The exact mechanism responsible for the reduced effectiveness of UVGI at these higher levels of relative humidity is unknown but does not appear to be related to changes in UV irradiance levels. Relative humidity changes from 55%–90% resulted in no corresponding changes in measured UVGI levels (437). In another study, an increase in relative humidity from 25%–67% did not reduce UVGI levels (422). Bacteria have been demonstrated to absorb substantial amounts of water from the air as the relative humidity increases. At high humidity, the UV irradiance levels required to inactivate bacteria might approach the higher levels that are needed for liquid suspensions of bacteria (448). The ability of bacteria to repair UVGI damage to their DNA through photoreactivation has also been reported to increase as relative humidity increases (422,448).
For optimal efficacy of upper-air UVGI, relative humidity should be maintained at ≤60%, a level that is consistent with recommendations for providing acceptable indoor air quality and minimizing environmental microbial contamination in indoor environments (386,451).
Ventilation rates. The relation between ventilation and UVGI has also been evaluated. Certain predicted inactivation rates have been calculated and published for varying flow rates, UV intensity, and distances from the lamp, based on radiative heat transfer theory (438). In room studies with substantially well-mixed air, ventilation rates (0 ACH, 3 ACH, and 6 ACH) were combined with various irradiation levels of upper-air UVGI. All experiments were conducted at 50% relative humidity and 70º F (21.2° C). When M. parafortuitum was used as a surrogate for M. tuberculosis, ventilation rates usually had no adverse effect on the efficiency of upper-air UVGI. The combined effect of both environmental controls was primarily additive in this artificial environment, with possibly a small loss of upper-air UVGI efficiency at 6 ACH (422). Therefore, ventilation rates of up to 6 ACH in a substantially well-mixed room might achieve ≥12 ACH (mechanical ACH plus equivalent ACH) by combining these rates with the appropriate level of upper-air irradiation (422). Higher ventilation rates (>6 ACH) might, however, decrease the time the air is irradiated and, therefore, decrease the killing of bacteria (429,452).
Ventilation rates up to six mechanical ACH do not appear to adversely affect the performance of upper-air UVGI in a substantially well-mixed room. Additional studies are needed to examine the combined effects of mechanical ventilation and UVGI at higher room-air exchange rates.
UVGI intensity. UVGI intensity field plays a primary role in the performance of upper-air UVGI systems. The UVGI dose received by microorganisms is a function of UVGI times duration of exposure. Intensity is influenced by the lamp wattage, distance from the lamp, surface area, and presence of reflective surfaces. The number of lamps, location, and UVGI level needed in a room depends on the room's geometry, area, and volume, and the location of supply air diffusers (422,436). UVGI fixtures should be spaced to reduce overlap while maintaining an even irradiance zone in the upper air.
The emission profile of a fixture is a vital determinant of UVGI effectiveness. Information regarding total UVGI output for a given fixture (lamp plus housing and louvers) should be requested from the manufacturer and used for comparison when selecting UVGI systems. Information concerning only the UVGI output of the lamp is inadequate; the lamp output will be higher than the output for the fixture because of losses from reflectors and nonreflecting surfaces and the presence of louvers and other obstructions (436,437). In addition, information provided by the manufacturer reflects ideal laboratory conditions; damage to fixtures or improper installation will affect UV radiation output. Because old or dust-covered UVGI lamps are less effective, routine maintenance and cleaning of UVGI lamps and fixtures is essential. UVGI system designers should consider room geometry, fixture output, room ventilation, and the desired level of equivalent ACH in determining the types, numbers, and placement of UVGI fixtures in a room to achieve target irradiance levels in the upper air.
Health and safety issues. Short-term overexposure to UV radiation can cause erythema (i.e., abnormal redness of the skin), photokeratitis (inflammation of the cornea), and conjunctivitis (i.e., inflammation of the conjunctiva) (453). Symptoms of photokeratitis and conjunctivitis include a feeling of sand in the eyes, tearing, and sensitivity to light. Photokeratitis and conjunctivitis are reversible conditions, but they can be debilitating while they run their course. Because the health effects of UVGI are usually not evident until after exposure has ended (typically 6–12 hours later), HCWs might not recognize them as occupational injuries.
In 1992, UV-C (100–280 nm) radiation was classified by the International Agency for Research on Cancer as "probably carcinogenic to humans (Group 2A)" (454). This classification was based on studies indicating that UV-C radiation can induce skin cancers in animals and create DNA damage, chromosomal aberrations, and sister chromatid exchange and transformation in human cells in vitro. In addition, DNA damage in mammalian skin cells in vivo can be caused. In the animal studies, a contribution of UV-C radiation to the tumor effects could not be excluded, but the effects were higher than expected for UV-B radiation alone (454). Certain studies have demonstrated that UV radiation can activate HIV gene promoters (i.e., genes in HIV that prompt replication of the virus) in laboratory samples of human cells (455–460). The potential for UV-C radiation to cause cancer and promote HIV in humans is unknown, but skin penetration might be an important factor. According to certain reports, only 20% of incident 250 nm UV penetrates the stratum corneum, compared with approximately 30–60% of 300 nm UV (UV-B) radiation (461).
In upper-air UVGI systems, fixtures must be designed and installed to ensure that UVGI exposures to occupants are below current safe exposure levels. Health-hazard evaluations have identified potential problems at some settings using UVGI systems. These problems include overexposure of HCWs to UVGI and inadequate maintenance, training, labeling, and use of personal protective equipment (PPE) (398,462,463).
An improperly maintained (unshielded) germicidal lamp was believed to be the cause of dermatosis or photokeratitis in five HCWs in an ED (464) and three HCWs who were inadvertently exposed to an unshielded UVGI lamp in a room that had been converted from a sputum induction room to an office (465). These case reports highlight the importance of posting warning signs to identify the presence of UVGI (see Supplement, Labeling and Posting) and are reminders that shielding should be used to minimize UVGI exposures to occupants in the lower room. In the majority of applications, properly designed, installed, and maintained UVGI fixtures provide protection from the majority of, if not all, the direct UVGI in the lower room. However, radiation reflected from glass, polished metal, and high-gloss ceramic paints can be harmful to persons in the room, particularly if more than one UVGI fixture is in use. Surfaces in irradiated rooms that can reflect UVGI into occupied areas of the room should be covered with non-UV–reflecting material.
Although more studies need to be conducted, lightweight clothing made of tightly woven fabric and UV-absorbing sunscreens with solar-protection factors (SPFs) of ≥15 might help protect photosensitive persons. Plastic eyewear containing a UV inhibitor that prevents the transmission of ≥95% of UV radiation in the 210–405 nm range is commercially available. HCWs should be advised that any eye or skin irritation that develops after UVGI exposure should be evaluated by an occupational health professional.
Exposure criteria. In 1972, CDC published a recommended exposure limit (REL) for occupational exposure to UV radiation (453). REL is intended to protect HCWs from the acute effects of UV light exposure. Photosensitive persons and those exposed concomitantly to photoactive chemicals might not be protected by the recommended standard.
The CDC/NIOSH REL for UV radiation is wavelength dependent because different wavelengths have different adverse effects on the skin and eyes (453). At 254 nm, the predominant wavelength for germicidal UV lamps, the CDC/NIOSH REL is 0.006 joules per square centimeter (J/cm2) for a daily 8-hour work shift. ACGIH has a Threshold Limit Value(r) for UV radiation that is identical to the REL for this spectral region (466). HCWs frequently do not stay in one place in the setting during the course of their work and, therefore, are not exposed to UV irradiance levels for 8 hours. Permissible exposure times (PET) for HCWs with unprotected eyes and skin can be calculated for various irradiance levels as follows:
PET (seconds) = 0.006 J/cm2 (CDC/NIOSH REL at 254 nm)
Measured irradiance level (at 254 nm) in W/cm2
Exposures exceeding the CDC/NIOSH REL require the use of PPE to protect the skin and eyes.
Labeling, Maintenance, and Monitoring
Labeling and posting. Health-care settings should post warning signs on UV lamps and wherever high-intensity (i.e., UVGI exposure greater than the REL) UVGI irradiation is present to alert maintenance staff, HCWs, and the general public of the hazard. The warning signs should be written in the languages of the affected persons (Box 6).
Maintenance. Because the UVGI output of the lamps declines with age, a schedule for replacing the lamps should be developed in accordance with manufacturer recommendations. The schedule can be determined from a time-use log, a system based on cumulative time, or routinely (e.g., at least annually). UVGI lamps should be checked monthly for dust build-up, which lessens radiation output. A dirty UVGI lamp should be allowed to cool and then should be cleaned in accordance with the manufacturer recommendations so that no residue remains.
UVGI lamps should be replaced if they stop glowing, if they flicker, or if the measured irradiance (see Supplement, Environmental Controls) drops below the performance criteria or minimum design criterion set forth by the design engineers. Maintenance personnel must switch off all UVGI lamps before entering the upper part of the room or before accessing ducts for any purpose. Only limited seconds of direct exposure to the intense UVGI in the upper-air space or in ducts can cause dermatosis or photokeratitis. Protective clothing and equipment (e.g., gloves, goggles, face shield, and sunscreen) should be worn if exposure greater than the recommended levels is possible or if UVGI radiation levels are unknown.
Banks of UVGI lamps can be installed in ventilation system ducts. Safety devices and lock-out or tag-out protocols should be used on access doors to eliminate exposures of maintenance personnel. For duct irradiation systems, the access door for servicing the lamps should have an inspection window through which the lamps are checked periodically for dust build-up and to ensure that they are functioning properly. The access door should have a warning sign written in appropriate languages to alert maintenance personnel to the health hazard of looking directly at bare UV lamps. The lock for this door should have an automatic electric switch or other device that turns off the lamps when the door is opened.
Types of fixtures used in upper-air irradiation include wall-mounted, corner-mounted, and ceiling-mounted fixtures that have louvers or baffles to block downward radiation and ceiling-mounted fixtures that have baffles to block radiation below the horizontal plane of the fixtures. If possible, light switches that can be locked should be used to prevent injury to persons who might unintentionally turn the lamps on during maintenance procedures. Because lamps must be discarded after use, consideration should be given to selecting germicidal lamps that are manufactured with relatively low amounts (i.e., ≤5 mg) of mercury. UVGI products should be listed with the Underwriters Laboratories (UL) or Electrical Testing Laboratories (ETL) for their specific application and installed in accordance with the National Electric Code.
Monitoring. UVGI intensity should be measured by an industrial hygienist or other person knowledgeable in the use of UV radiometers with a detector designed to be most sensitive at 254 nm. Equipment used to measure UVGI should be maintained and calibrated on a regular schedule, as recommended by the manufacturer.
UVGI should be measured in the lower room to ensure that exposures to occupants are below levels that could result in acute skin and eye effects. The monitoring should consider typical duties and locations of the HCWs and should be done at eye level. At a minimum, UVGI levels should be measured at the time of initial installation and whenever fixtures are moved or other changes are made to the system that could affect UVGI. Changes to the room include those that might result in higher exposures to occupants (e.g., addition of UV-reflecting materials or painting of walls and ceiling). UVGI monitoring information, lamp maintenance, meter calibration, and lamp and fixture change-outs should be recorded.
UVGI measurements should also be made in the upper air to define the area that is being irradiated and determine if target irradiance levels are met (467). Measurements can be made using UVGI radiometers or other techniques (e.g., spherical actinometry), which measures the UVGI in an omnidirectional manner to estimate the energy to which microorganisms would be exposed (468). Because high levels of UVGI can be measured in the upper air, persons making the measurements should use adequate skin and eye protection. UVGI radiation levels close to the fixture source can have permissible exposure times on the order of seconds or minutes for HCWs with unprotected eyes and skin. Therefore, overexposures can occur with brief UVGI exposures in the upper air (or in ventilation system ducts where banks of unshielded UV lamps are placed) in HCWs who are not adequately protected.
Upper-air UVGI systems and portable room-air recirculation units. A study in 2002 examined the relation between three portable room-air recirculation units with different capture or inactivation mechanisms and an upper-air UVGI system in a simulated health-care room (409). The study determined that the equivalent ACH produced by the recirculation units and produced by the upper-air UVGI system were approximately additive. For example, one test using aerosolized M. parafortuitum provided an equivalent ACH for UVGI of 17 and an equivalent ACH for the recirculation unit of 11; the total experimentally measured equivalent ACH for the two systems was 27. Therefore, the use of portable room-air recirculation units in conjunction with upper-air UVGI systems might increase the overall removal of M. tuberculosis droplet nuclei from room air.
Environmental Controls: Program Concerns
To be most effective, environmental controls must be installed, operated, and maintained correctly. Ongoing maintenance is a critical part of infection control that should be addressed in the written TB infection-control plan. The plan should outline the responsibility and authority for maintenance and address staff training needs. At one hospital, improperly functioning ventilation controls were believed to be an important factor in the transmission of MDR TB disease to three patients and a correctional officer, three of whom died (469). In three other multihospital studies evaluating the performance of AII rooms, failure to routinely monitor air-pressure differentials or a failure of the continuous monitoring devices installed in the AII rooms resulted in a substantial percentage of the rooms being under positive pressure (57,392,470,471).
Routine preventive maintenance should be scheduled and should include all components of the ventilation systems (e.g., fans, filters, ducts, supply diffusers, and exhaust grilles) and any air-cleaning devices in use. Performance monitoring should be conducted to verify that environmental controls are operating as designed. Performance monitoring can include 1) directional airflow assessments using smoke tubes and use of pressure monitoring devices that are sensitive to pressures as low as approximately 0.005 inch of water gauge and 2) measurement of supply and exhaust airflows to compare with recommended air change rates for the respective areas of the setting. Records should be kept to document all preventive maintenance and repairs.
Standard procedures should be established to ensure that maintenance staff notifies infection-control personnel before performing maintenance on ventilation systems servicing patient-care areas. Similarly, infection-control staff should request assistance from maintenance personnel in checking the operational status of AII rooms and local exhaust devices (e.g., booths, hoods, and tents) before use. A protocol that is well-written and followed will help to prevent unnecessary exposures of HCWs and patients to infectious aerosols. Proper labeling of ventilation system components (e.g., ducts, fans, and filters) will help identify air-flow paths. Clearly labeling which fan services a given area will help to prevent accidental shutdowns (472).
In addition, provisions should be made for emergency power to avoid interruptions in the performance of essential environmental controls during a power failure.
Respiratory Protection
Considerations for Selection of Respirators
The overall effectiveness of respiratory protection is affected by 1) the level of respiratory protection selected (e.g., the assigned protection factor), 2) the fit characteristics of the respirator model, 3) the care in donning the respirator, and 4) the adequacy of the fit-testing program. Although data on the effectiveness of respiratory protection from various hazardous airborne materials have been collected, the precise level of effectiveness in protecting HCWs from M. tuberculosis transmission in health-care settings has not been determined.
Information on the transmission parameters of M. tuberculosis is also incomplete. Neither the smallest infectious dose of M. tuberculosis nor the highest level of exposure to M. tuberculosis at which transmission will not occur has been defined conclusively (159,473,474). In addition, the size distribution of droplet nuclei and the number of particles containing viable M. tuberculosis organisms that are expelled by patients with infectious TB disease have not been adequately defined, and accurate methods of measuring the concentration of infectious droplet nuclei in a room have not been developed. Nonetheless, in certain settings (e.g., AII rooms and ambulances during the transport of persons with suspected or confirmed infectious TB disease), administrative and environmental controls alone might not adequately protect HCWs from infectious airborne droplet nuclei.
On October 17, 1997, OSHA published a proposed standard for occupational exposure to M. tuberculosis (267). On December 31, 2003, OSHA announced the termination of rulemaking for a TB standard (268). Previous OSHA policy permitted the use of any Part 84 particulate filter respirator for protection against infection with M. tuberculosis (269). Respirator usage for TB had been regulated by OSHA under CFR Title 29, Part 1910.139 (29 CFR 1910.139) (270) and compliance policy directive (CPL) 2.106 (Enforcement Procedures and Scheduling for Occupational Exposure to Tuberculosis). Respirator usage for TB is now regulated under the general industry standard for respiratory protection (29 CFR 1910.134) (271). General information on respiratory protection for aerosols, including M. tuberculosis, has been published (272–274).
Performance Criteria for Respirators
Performance criteria for respirators are derived from data on 1) effectiveness of respiratory protection against noninfectious hazardous materials in workplaces other than health-care settings and an interpretation of how these data can be applied to respiratory protection against M. tuberculosis, 2) efficiency of respirator filters in filtering biologic aerosols, 3) face-seal leakage, and 4) characteristics of respirators used in conjunction with administrative and environmental controls in outbreak settings to stop transmission of M. tuberculosis to HCWs and patients.
Particulate filter respirators certified by CDC/NIOSH, either nonpowered respirators with N95, N99, N100, R95, R99, R100, P95, P99, and P100 filters (including disposable respirators), or PAPRs with high efficiency filters can be used for protection against airborne M. tuberculosis.
The most essential attribute of a respirator is the ability to fit the different facial sizes and characteristics of HCWs. Studies have demonstrated that fitting characteristics vary substantially among respirator models. The fit of filtering facepiece respirators varies because of different facial types and respirator characteristics (10,280–289). Selection of respirators can be done through consultation with respirator fit-testing experts, CDC, occupational health and infection-control professional organizations, peer-reviewed research, respirator manufacturers, and from advanced respirator training courses. Data have determined that fit characteristics cannot be determined solely by physical appearance of the respirator (282).
Types of Respiratory Protection for TB
Respirators encompass a range of devices that vary in complexity from flexible masks covering only the nose and mouth, to units that cover the user's head (e.g., loose-fitting or hooded PAPRs), and to those that have independent air supplies (e.g., airline respirators). Respirators must be selected from those approved by CDC/NIOSH under the provisions of 42 CFR, Part 84 (475).
Nonpowered air-purifying respirators. Nine classes of nonpowered, air-purifying, particulate-filter respirators are certified under 42 CFR 84. These include N-, R-, and P-series respirators of 95%, 99%, and 100% (99.7%) filtration efficiency when challenged with 0.3 µm particles (filters are generally least efficient at this size) (Table 4). The N, R, and P classifications are based on the capacity of the filter to withstand exposure to oil. All of these respirators meet or exceed CDC's filtration efficiency performance criteria during the service life of the filter (1,272,273).
Nonpowered air-purifying respirators work by drawing ambient air through the filter during inhalation. Inhalation causes negative pressure to develop in the tight-fitting facepiece and allows air to enter while the particles are captured on the filter. Air leaves the facepiece during exhalation because positive pressure develops in the facepiece and forces air out of the mask through the filter (disposable) or through an exhalation valve (replaceable and certain ones are disposable).
The classes of certified nonpowered air-purifying respirators include both filtering facepiece (disposable) respirators and elastomeric (rubber-like) respirators with filter cartridges. The certification test for filtering facepieces and filter cartridges consists only of a filter performance test. It does not address respirator fit. Although all N-, R-, and P-series respirators are recommended for protection against M. tuberculosis infection in health-care settings and other workplaces that are usually free of oil aerosols that could degrade filter efficiency, well-fitting N-series respirators are usually less expensive than R- and P-series respirators (272,273). All respirators should be replaced as needed, based on hygiene considerations, increased breathing resistance, time-use limitations specified in the CDC/NIOSH approval guidelines, respirator damage, and in accordance with manufacturer user's instructions.
PAPRs. PAPRs use a blower that draws air through the filters into the facepiece. PAPRs can be equipped with a tight-fitting or loose-fitting facepiece, a helmet, or a hood. PAPR filters are classified as high efficiency and are different from those presented in this report (Table 4). A PAPR high efficiency filter meets the N100, R100, and P100 criteria at the beginning of their service life. No loading tests using 0.3 µm particles are conducted as part of certification. PAPRs can be useful for persons with facial hair or other conditions that prevent an adequate face to facepiece seal (476).
Atmosphere-supplying respirators. Positive-pressure airline (supplied-air) respirators are provided with air from a stationary source (compressor) or an air tank.
Effectiveness of Respiratory-Protection Devices
Data on the effectiveness of respiratory protection against hazardous airborne materials are based on experience in the industrial setting; data on protection against transmission of M. tuberculosis in health-care settings are not available. The parameters used to determine the effectiveness of a respiratory protective device are face-seal efficacy and filter efficiency.
Face-seal leakage. Face-seal leakage is the weak link that limits a respirator's protective ability. Excessive face-seal leakage compromises the ability of particulate respirators to protect HCWs from airborne materials (477). A proper seal between the respirator's sealing surface and the face of the person wearing the respirator is essential for the effective and reliable performance of any tight-fitting, negative-pressure respirator.
For tight-fitting, negative-pressure respirators (e.g., N95 disposable respirators), the amount of face-seal leakage is determined by 1) the fit characteristics of the respirator, 2) the care in donning the respirator, and 3) the adequacy of the fit-testing program. Studies indicate that a well-fitting respirator and a fit test produces better results than a well-fitting respirator without a fit test or a poor-fitting respirator with a fit test. Increased face-seal leakage can result from additional factors, including incorrect facepiece size, failure to follow the manufacturer's instructions at each use, beard growth, perspiration or facial oils that can cause facepiece slippage, improper maintenance, physiological changes of the HCW, and respirator damage.
Face-seal leakage is inherent in tight-fitting negative-pressure respirators. Each time a person wearing a nonpowered particulate respirator inhales, negative pressure (relative to the workplace air) is created inside the facepiece. Because of this negative pressure, air containing contaminants can leak into the respirator through openings at the face-seal interface and avoid the higher-resistance filter material. A half-facepiece respirator, including an N95 disposable respirator, should have <10% leakage. Full facepiece, nonpowered respirators have the same leakage (<2%) as PAPRs with tight-fitting full-facepieces.
The more complex PAPRs and positive-pressure airline respirators reduce or eliminate this negative facepiece pressure and, therefore, reduce leakage into the respirator and enhance protection. A PAPR is equipped with a blower that forcibly draws ambient air through high efficiency filters and then delivers the filtered air to the facepiece. This air is blown into the facepiece at flow rates that generally exceed the expected inhalation flow rates. The pressure inside the facepiece reduces face-seal leakage to low levels, particularly during the relatively low inhalation rates expected in health-care settings. PAPRs with a tight-fitting facepiece have <2% face-seal leakage under routine conditions (278). PAPRs with loose-fitting facepieces, hoods, or helmets have <4% inward leakage under routine conditions (278). Therefore, a PAPR might offer lower levels of face-seal leakage than nonpowered, half-mask respirators.
Filter penetration. Aerosol penetration through respirator filters depends on at least five independent variables: 1) filtration characteristics for each type of filter, 2) size distribution of the droplets in the aerosol, 3) linear velocity through the filtering material, 4) filter loading (i.e., amount of contaminant deposited on the filter), and 5) electrostatic charges on the filter and on the droplets in the aerosol (284).
When N95 disposable respirators are used, filter penetration might approach 5% (50% of the allowable leakage of 10% for an N95 disposable respirator). When high efficiency filters are used in PAPRs or for half-facepiece respirators, filter efficiency is high (effectively 100%), and filter penetration is less of a consideration. Therefore, for high efficiency or 100-series filter respirators, the majority of inward leakage of droplet nuclei occurs at the respirator's faceseal or exhalation valve.
Implementing a Respiratory-Protection Program
If respirators are used in a health-care setting, OSHA requires the development, implementation, administration, and periodic reevaluation of a respiratory-protection program (271,277,278). The most critical elements of a respiratory- protection program include 1) assigning of responsibility, 2) training, and 3) fit testing (1). All HCWs who use respirators for protection against infection with M. tuberculosis should be included in the respiratory-protection program.
Visitors to AII rooms and other areas with patients who have suspected or confirmed infectious TB disease may be offered respirators (e.g., N95 disposable respirators) and should be instructed by an HCW on the use of the respirator before entering an AII room (see Respiratory Protection section for User-Seal Check FAQs). The health-care setting should develop a policy on use of respirators by visitors.
The number of HCWs included in the respiratory- protection program will vary depending on the 1) number of persons who have suspected or confirmed TB disease examined in a setting, 2) number of rooms or areas in which patients with suspected or confirmed infectious TB disease stay or are encountered, and 3) number of HCWs needed to staff these rooms or areas. In settings in which respiratory-protection programs are required, enough HCWs should be included to provide adequate care for patients with suspected or confirmed TB disease. However, administrative measures should be used to limit the number of HCWs exposed to M. tuberculosis (see Prompt Triage).
Information on the development and management of a respiratory-protection program is available in technical training courses that cover the basics of respiratory protection. Such courses are offered by OSHA, the American Industrial Hygiene Association, universities, manufacturers, and private contractors. To be effective and reliable, respiratory-protection programs must include at least the following elements (274,277,278).
Assignment of Responsibility
One person (the program administrator) must be in charge of the respiratory-protection program and be given the authority and responsibility to manage all aspects of the program. The administrator must have sufficient knowledge (obtained by training or experience) to develop and implement a respiratory-protection program. Preferably, the administrator should have a background in industrial hygiene, safety, health care, or engineering. The administrator should report to the highest official possible (e.g., manager of the safety department, supervisor of nurses, HCWs' health manager, or infection-control manager) and should be allocated sufficient time to administer the respiratory-protection program in addition to other assigned duties.
Standard Operating Procedures
The effectiveness of a respiratory-protection program requires the development of written standard procedures. These procedures should include information and guidance for the proper selection, use, and care of respirators (274).
Screening
HCWs should not be assigned a task requiring use of respirators unless they are physically able to perform job duties while wearing the respirator. HCWs who might need to use a respirator should be screened by a physician or other licensed health-care professional for pertinent medical conditions at the time they are hired and then re-screened periodically (274). The screening process should begin with a screening questionnaire for pertinent medical conditions, the results of which should be used to identify HCWs who need further evaluation (Appendix G). Unless prescribed by the screening physician, serial physical examination or testing with chest radiographs or spirometry is neither necessary nor required (287).
Training
HCWs should be provided annual training on multiple topics.
Nature, extent, and hazards of TB disease in the health-care setting. This training can be conducted in conjunction with other related training on infectious disease associated with airborne transmission (e.g., severe acute respiratory syndrome [SARS]-coronavirus [CoV] and measles) and with serial TB screening.
The risk assessment process and its relation to the respirator program.
Signs and symbols used to demonstrate that respirators are required in an area.
Reasons for using respirators.
Environmental controls used to prevent the spread and reduce the concentration of infectious droplet nuclei.
Reasons for selecting a particular respirator for a given hazard (see Selection of Respirators; and Respirator Options: Special Circumstances).
Operation, capabilities, and limitations of respirators.
Respirator care.
Cautions regarding facial hair and respirator use.
Applicable federal, state, and local regulations regarding respirators, including assessment of employees' knowledge.
Trainees should be provided resources as an adjunct to the respiratory-protection program.
Opportunities to handle and wear a respirator until they are proficient (see Supplement, Fit Testing).
Educational material for use as references.
Instructions to refer all respirator problems immediately to the respirator program administrator.
Selection
Filtering facepiece respirators used for protection against M. tuberculosis must be selected from those approved by CDC/NIOSH under the provisions of 42 CFR 84 (http://www.cdc.gov/niosh/celintro.html). A listing of CDC/NIOSH-approved disposable particulate respirators (filtering facepieces) is available at http://www.cdc.gov/niosh/npptl/topics/respirators/disp_part. If a health-care setting uses respirators for protection against other regulated hazards (e.g., formaldehyde and ethylene oxide), then these potential exposures should be specifically addressed in the program. Combination product surgical mask/N95 disposable respirators (respirator portion certified by CDC/NIOSH and surgical mask portion listed by FDA) are available that provide both respiratory protection and bloodborne pathogen protection. Selection of respirators can be chosen through consultation with respirator fit-testing experts, CDC, occupational health and infection-control professional organizations, peer-reviewed research, respirator manufacturers, and advanced respirator training courses (10,280–289).
Fit Testing
A fit test is used to determine which respirator fits the user adequately and to ensure that the user knows when the respirator fits properly. After a risk assessment is conducted to validate the need for respiratory protection, perform fit testing during the initial respiratory-protection program training and periodically thereafter, in accordance with federal, state, and local regulations.
Fit testing provides a method to determine which respirator model and size fits the wearer best and to confirm that the wearer can properly fit the respirator. Periodic fit testing for respirators used in environments where a risk for M. tuberculosis transmission exists can serve as an effective training tool in conjunction with the content included in employee training and retraining. The frequency of periodic fit testing should be determined by the occurrence of 1) a risk for transmission of M. tuberculosis, 2) a change in facial features of the wearer, 3) a medical condition that would affect respiratory function, 4) physical characteristics of respirator (despite the same model number), or 5) a change in the model or size of the assigned respirator (281).
Inspection and Maintenance
Respirator maintenance should be an integral part of an overall respirator program. Maintenance applies both to respirators with replaceable filters and to respirators that are classified as disposable but are reused. Manufacturer instructions for inspecting, cleaning, maintaining, and using (or reuse) respirators should be followed to ensure that the respirator continues to function properly (278).
When respirators are used for protection against noninfectious aerosols (e.g., wood dust) that might be present in the air in heavy concentrations, the filter can become obstructed with airborne material. This obstruction in the filter material can result in increased resistance, causing breathing to be uncomfortable. In health-care settings in which respirators are used for protection against biologic aerosols, the concentration of infectious particles in the air is probably low. Thus, the filter in a respirator is unlikely to become obstructed with airborne material. In addition, no evidence exists to indicate that particles that affect the filter material in a respirator are reaerosolized easily. Therefore, the filter material used in respirators in health-care settings might remain functional for weeks. Because electrostatic filter media can degrade, the manufacturer should be contacted for the product's established service life to confirm filter performance.
Respirators with replaceable filters are reusable, and a respirator classified as disposable can be reused by the same HCW as long as it remains functional and is used in accordance with local infection-control procedures. Respirators with replaceable filters and filtering facepiece respirators can be reused by HCWs as long as they have been inspected before each use and are within the specified service life of the manufacturer. If the filter material is physically damaged or soiled or if the manufacturer's service life criterion has been exceeded, the filter (in respirators with replaceable filters) should be changed or the disposable respirator should be discarded according to local regulations. Infection-control personnel should develop standard procedures for storing, reusing, and disposing of respirators that have been designated for disposal.
Evaluation
The respirator program must be evaluated periodically to ensure its continued effectiveness.
Cleaning, Disinfecting, and Sterilizing Patient-Care Equipment and Rooms
General
Medical instruments and equipment, including medical waste, used on patients who have TB disease are usually not involved in the transmission of M. tuberculosis (478–480). However, transmission of M. tuberculosis and pseudo-outbreaks (e.g., contamination of clinical specimens) have been linked to inadequately disinfected bronchoscopes contaminated with M. tuberculosis (80,81,160,163,164,166). Guidelines for cleaning, disinfecting, and sterilizing flexible endoscopic instruments have been published (481–485).
The rationale for cleaning, disinfecting, or sterilizing patient-care instruments and equipment can be understood more readily if medical devices, equipment, and surgical materials are divided into three general categories (486). The categories are critical, semicritical, and noncritical and are based on the potential risk for infection if an item remains contaminated at the time of use.
Critical Medical Instruments
Instruments that are introduced directly into the bloodstream or other normally sterile areas of the body (e.g., needles, surgical instruments, cardiac catheters, and implants) are critical medical instruments. These items should be sterile at the time of use.
Semicritical Medical Instruments
Instruments that might come into contact with mucous membranes but do not ordinarily penetrate body surfaces (e.g., noninvasive flexible and rigid fiberoptic endoscopes or bronchoscopes, endotracheal tubes, and anesthesia breathing circuits) are semicritical medical instruments. Although sterilization is preferred for these instruments, high-level disinfection that destroys vegetative microorganisms, the majority of fungal spores, mycobacteria (including tubercle bacilli), and small nonlipid viruses can be used. Meticulous cleaning of such items before sterilization or high-level disinfection is essential (481). When an automated washer is used to clean endoscopes and bronchoscopes, the washer must be compatible with the instruments to be cleaned (481,487). High-level disinfection can be accomplished with either manual procedures alone or use of an automated endoscope reprocessor with manual cleaning (80,481). In all cases, manual cleaning is an essential first-step in the process to remove debris from the instrument.
Noncritical Medical Instruments or Devices
Instruments or devices that either do not ordinarily touch the patient or touch only the patient's intact skin (e.g., crutches, bed boards, and blood pressure cuffs) are noncritical medical instruments. These items are not associated with transmission of M. tuberculosis. When noncritical instruments or equipment are contaminated with blood or body substances, they should be cleaned and then disinfected with a hospital-grade, Environmental Protection Agency (EPA)-registered germicide disinfectant with a label claim for tuberculocidal activity (i.e., an intermediate-level disinfectant). Tuberculocidal activity is not necessary for cleaning agents or low-level disinfectants that are used to clean or disinfect minimally soiled noncritical items and environmental surfaces (e.g., floors, walls, tabletops, and surfaces with minimal hand contact).
Disinfection
The rationale for use of a disinfectant with tuberculocidal activity is to ensure that other potential pathogens with less intrinsic resistance than that of mycobacteria are killed. A common misconception in the use of surface disinfectants in health care relates to the underlying purpose of products labeled as tuberculocidal germicides. Such products will not interrupt and prevent transmission of M. tuberculosis in health-care settings, because TB is not acquired from environmental surfaces. The tuberculocidal claim is used as a benchmark by which to measure germicidal potency. Because mycobacteria have the highest intrinsic level of resistance among the vegetative bacteria, viruses, and fungi, any germicide with a tuberculocidal claim on the label (i.e., an intermediate-level disinfectant) is considered capable of inactivating many pathogens, including much less resistant organisms such as the bloodborne pathogens (e.g., hepatitis B virus, hepatitis C virus, and HIV). Rather than the product's specific potency against mycobacteria, a germicide that can inactivate many pathogens is the basis for protocols and regulations indicating the appropriateness of tuberculocidal chemicals for surface disinfection.
Policies of health-care settings should specify whether cleaning, disinfecting, or sterilizing an item is necessary to decrease the risk for infection. Decisions regarding decontamination processes should be based on the intended use of the item, not on the diagnosis of the condition of the patient for whom the item is used. Selection of chemical disinfectants depends on the intended use, the level of disinfection required, and the structure and material of the item to be disinfected.
The same cleaning procedures used in other rooms in the health-care setting should be used to clean AII rooms. However, personnel should follow airborne precautions while cleaning these rooms when they are still in use. Personal protective equipment is not necessary during the final cleaning of an AII room after a patient has been discharged if the room has been ventilated for the appropriate amount of time (Table 1).
Frequently Asked Questions (FAQs)
The following are FAQs regarding TST, QFT-G, BAMT, treatment for LTBI, risk assessment, environmental controls, respiratory protection, and cough-inducing and aerosol-generating procedures.
TST and QFT-G
Does having more than one TST placed in 1 year pose any risk? No risk exists for having TSTs placed multiple times per year.
Can repeated TSTs, by themselves, cause the TST result to convert from negative to positive? No, the TST itself does not cause false-positive results. Exposure to other mycobacteria or BCG vaccination can cause false-positive TST results.
What defines a negative TST result? A TST result of 0 mm or a measurement below the defined cut point for each criteria category is considered a negative TST result (Box 3).
What defines a positive TST result? A TST result of any millimeter reading above or at the defined cut point for each criteria category is considered a positive TST result (Box 3). The cut point (5 mm, 10 mm, and 15 mm) varies according to the purpose of the test (e.g., infection-control surveillance or medical and diagnostic evaluation, or contact investigation versus baseline testing).
What defines a false-negative result? A false-negative TST or QFT-G result is one that is interpreted as negative for a particular purpose (i.e., infection-control surveillance versus medical and diagnostic evaluation) in a person who is actually infected with M. tuberculosis. False-negative TST results might be caused by incorrect TST placement (too deeply or too shallow), incorrect reading of the TST result, use of an incorrect antigen, or if the person being tested is anergic (i.e., unable to respond to the TST because of an immunocompromising condition) or sick with TB disease.
What defines a false-positive result? A false-positive TST or QFT-G result is one that is interpreted as positive for a particular purpose (i.e., infection-control surveillance versus medical and diagnostic evaluation) in a person who is actually not infected with M. tuberculosis. False-positive TST results are more likely to occur in persons who have been vaccinated with BCG or who are infected with NTM, also known as mycobacteria other than TB (MOTT). A false-positive TST result might also be caused by incorrect reading of the TST result (reading erythema rather than induration) or use of incorrect antigen (e.g., tetanus toxoid).
Is placing a TST on a nursing mother safe? Yes, placing a TST on a nursing mother is safe.
A pregnant HCW in a setting is reluctant to get a TST. Should she be encouraged to have the test administered? Yes, placing a TST on a pregnant woman is safe. The HCW should be encouraged to have a TST or offered BAMT. The HCW should receive education that 1) pregnancy is not a contraindication to having a TST administered and 2) skin testing does not affect the fetus or the mother. Tens of thousands of pregnant women have received TST since the test was developed, and no documented episodes of TST-related fetal harm have been reported. Guidelines issued by ACOG emphasize that postponement of the application of a TST as indicated and postponement of the diagnosis of infection with M. tuberculosis during pregnancy is unacceptable.
A pregnant HCW in a setting has a positive TST result and is reluctant to get a chest radiograph. Should she be encouraged to have the chest radiograph performed? Pregnant women with positive TST results or who are suspected of having TB disease should not be exempted from recommended medical evaluations and radiography. Shielding consistent with safety guidelines should be used even during the first trimester of pregnancy.
Are periodic chest radiographs recommended for HCWs (or staff or residents of LTCFs) who have positive TST or BAMT results? No, persons with positive TST or BAMT results should receive one baseline chest radiograph to exclude a diagnosis of TB disease. Further chest radiographs are not needed unless the patient has symptoms or signs of TB disease or unless ordered by a physician for a specific diagnostic examination. Instead of participating in serial skin testing, HCWs with positive TST results should receive a medical evaluation and a symptom screen. The frequency of this medical evaluation should be determined by the risk assessment for the setting. HCWs who have a previously positive TST result and who change jobs should carry documentation of the TST result and the results of the baseline chest radiograph (and documentation of treatment history for LTBI or TB disease, if applicable) to their new employers.
What is boosting? Boosting is a phenomenon in which a person has a negative TST (i.e., false-negative) result years after infection with M. tuberculosis and then a positive subsequent TST result. The positive TST result is caused by a boosted immune response of previous sensitivity rather than by a new infection (false-positive TST conversion). Two-step testing reduces the likelihood of mistaking a boosted reaction for a new infection.
What procedure should be followed for a newly hired HCW who had a documented negative TST result 3 months ago at their previous job? This person should receive one baseline TST upon hire (ideally before the HCW begins assigned duties). The negative TST result from the 3 months preceding new employment (or a documented negative TST result anytime within the previous 12 months) should be considered the first step of the baseline two-step TST. If the HCW does not have documentation of any TST result, the HCW should be tested with baseline two-step TST (one TST upon hire and one TST placed 1–3 weeks after the first TST result was read).
Why are two-step TSTs important for the baseline (the beginning of an HCW's employment)? If TST is used for TB screening (rather than BAMT), performing two-step TST at baseline minimizes the possibility that boosting will lead to suspicion of transmission of M. tuberculosis in the setting during a later contact investigation or during serial testing (false-positive TST conversions). HCWs who do not have documentation of a positive TST result or who have not been previously treated for LTBI or TB disease should receive baseline two-step TST.
If a person does not return for a TST reading within 48–72 hours, when can a TST be placed on them again? A TST can be administered again as soon as possible. If the second step of a two-step TST is not read within 48–72 hours, administer a third test as soon as possible (even if several months have elapsed), and ensure that the result is read within 48–72 hours.
Should a TST reading of ≥10 mm be accepted 7 days after the TST was placed? If the TST was not read between 48–72 hours, another TST should be placed as soon as possible and read within 48–72 hours. However, certain studies indicate that positive TST reactions might still be measurable 4–7 days after the TST was placed. If the TST reaction is read as ≥15 mm 7 days after placement, the millimeter result can be recorded and considered to be a positive result.
Do health-care settings or areas in the United States exist for which baseline two-step TST for newly hired HCWs is not needed? Ideally, all newly hired HCWs who might share air space with patients should receive baseline two-step TST (or one-step BAMT) before starting duties. In certain settings, a choice might be offered not to perform baseline TST on HCWs who will never be in contact with or share air space with patients who have TB disease, or who will never be in contact with clinical specimens (e.g., telephone operators in a separate building from patients).
In our setting, workers are hired to provide health care in homes, and they are not medically trained. Two-step skin testing is difficult because of the requirement to return for testing and reading multiple times. Can the two-step TST be omitted? No, ideally, all HCWs who do not have a previously documented positive TST result or treated LTBI or TB disease should receive two-step baseline skin testing in settings that have elected to use TST for screening. BAMT is a single test procedure. Baseline testing for M. tuberculosis infection will ensure that TB disease or LTBI is detected before employment begins and treatment for LTBI or TB disease is offered, if indicated.
When performing two-step skin testing, what should be done if the second-step TST is not placed in 1–3 weeks? Perform the second-step TST as soon as possible, even if several months have passed.
Should gloves be worn when placing TST? Specific CDC recommendations do not exist regarding this topic. If your local area indicates that universal precautions should be practiced with skin testing, the local areas should determine what precautions should be followed in their setting.
Is TST QC important? Yes, performing QC for HCWs during training and retraining of placing and reading TST is important to avoid false-negative and false-positive TST results, and to ensure appropriate treatment decisions.
If the longitudinal reading of the induration of the TST result is 12 mm and the horizontal reading is 8 mm, what should be recorded? The correct TST reading should be recorded as 8 mm (not 12 mm or 8 x 12 mm). For purposes of standardization, only record the millimeters of induration, which should be measured transversely (i.e., perpendicular), to the long axis of the forearm. Erythema (redness) around the TST site should not be read as part of the TST result. Consideration should be given to retesting if the selected area for placement was on or near a muscle margin, scar, heavy hair, veins, or tattoos, which could be barriers to reading the TST result, or consider offering a BAMT. BAMT results should be recorded in detail. The details should include date of blood draw, result in specific units, and the laboratory interpretation (positive, negative, or indeterminate—and the concentration of cytokine measured, e.g., IFN-γ).
Should HCWs who report upon hire that they have had a positive TST result or have been previously treated for LTBI or TB disease receive baseline two-step TST when beginning work at a new health-care setting? Unless the HCW has documentation of a positive TST result or previously treated LTBI or TB disease, they should usually receive baseline two-step testing before starting duties. If documentation is available of a positive TST result, that result can be considered as the baseline TST result for the HCW at the new setting, and additional testing is not needed. Recommendations for testing HCWs who transfer from one setting to another where the risk assessment might be different are presented (see Use of Risk Classification to Determine Need for TB Screening and Frequency of Screening HCWs).
If an HCW has a baseline first-step TST result between 0–9 mm, does a second-step TST need to be placed? Yes, if the baseline first-step TST result is <10 mm, a second-step TST should be applied 1–3 weeks after the first TST result was read. HCWs who are immunocompromised are still subject to the 10 mm cutoff for baseline two-step testing for surveillance purposes but would be referred for medical evaluation for LTBI using the 5 mm cutoff.
An HCW in a medium-risk setting who had a two-step baseline TST result of 8 mm is retested 1 year later for serial TB screening and had a TST result of 16 mm. No known exposure to M. tuberculosis had occurred. Although the TST is now >10 mm, a ≥10 mm increase did not occur in the TST result to meet the criteria for a TST conversion. How should this reading be interpreted? The TST result needs to be interpreted from two perspectives: 1) administrative and 2) individual medical interpretation. Because an increase by ≥10 mm did not occur, the result would not be classified as a TST conversion for administrative purposes. However, this HCW should be referred for a medical evaluation. The following criteria are used to determine whether a TST result is positive or negative, considering individual clinical grounds: 1) absolute measured induration (i.e., ≥5, ≥10, or ≥15 mm induration, depending on the level of risk and purpose of testing); 2) the change in the size of the TST result; 3) time frame of the change; 4) risk for exposure, if any; and 5) occurrence of other documented TST conversions in the setting. For HCWs at low risk for LTBI, TST results of 10–14 mm can be considered negative from a clinical standpoint, and these HCWs should not have repeat TST, because an additional increase in induration of ≥10 mm will not be useful in determining the likelihood of LTBI.
Are baseline two-step TSTs needed for HCWs who begin jobs that involve limited contact with patients (e.g., medical records staff)? Yes, all HCWs who might share air space with patients should receive baseline two-step TST (or one-time BAMT) before starting duties. However, in certain settings, a choice might be offered not to perform baseline TST on HCWs who will never be in contact with or share air space with patients who have TB disease, or who will never be in contact with clinical specimens (e.g., telephone operators in a separate building from patients).
A setting conducts skin testing annually on the anniversary of each HCW's employment. Last year, multiple TST conversions occurred in April; therefore, all HCWs received a TST during that month. In the future, do all HCWs need to be tested annually in April? No, after a contact investigation is performed, the best and preferred schedule for annual TB screening is on the anniversary of the HCW's employment date or on their birthday (rather than testing all HCWs at the same time each year), because it increases the opportunity for early recognition of infection-control problems that can lead to TST conversions.
An HCW who has been vaccinated with BCG is being hired. She states that BCG will make her TST result positive and that she should not have a TST. Should this HCW be exempted from baseline two-step TST? Unless she has documentation of a positive TST result or previously treated LTBI or TB disease, she should receive baseline two-step TST or one BAMT. Some persons who received BCG never have a positive TST result. For others, the positive reaction wanes after 5 years. U.S. guidelines state that a positive TST result in a person who received BCG should be interpreted as indicating LTBI.
Does BCG affect TST results and interpretations? BCG is the most commonly used vaccine in the world. BCG might cause a positive TST (i.e., false-positive) result initially; however, tuberculin reactivity caused by BCG vaccination typically wanes after 5 years but can be boosted by subsequent TST. No reliable skin test method has been developed to distinguish tuberculin reactions caused by vaccination with BCG from reactions caused by natural mycobacterial infections, although TST reactions of ≥20 mm of induration are not usually caused by BCG.
What steps should be taken when an HCW has had a recent BCG vaccination? When should the TST be placed? A TST may be placed anytime after a BCG vaccination, but a positive TST result after a recent BCG vaccination can be a false-positive result. QFT-G should be used, because the assay test avoids cross reactivity with BCG.
A hospital HCW has not had a TST in 18 months because she was on maternity leave and missed her annual TST. She has been employed at the hospital for the previous 5 years. Is two-step testing necessary on her next skin test date? No, two-step TSTs are needed only to establish a baseline for a specific setting for newly hired HCWs and others who will receive serial TST (e.g., residents or staff of correctional facilities or LTCFs). The HCW should have a single TST or BAMT upon returning to work and should then resume a routine testing schedule on the next normal TST anniversary date.
Should two-step testing be performed in a contact investigation for HCWs who have not had a TST within the preceding 12 months? No, two-step testing should only be used for baseline TST screening and has no role in a contact investigation. In a contact investigation, a follow-up TST should be placed 8–10 weeks after an initial negative TST result is read.
What length of time should a person who has had contact with someone with TB disease be included in a contact investigation? This decision can best be made in consultation with the local TB program, which frequently has experience responding to similar situations. A minimum exposure time has not been established, but the minimum length of contact time with a person who has TB disease necessary for transmission will depend on multiple factors. Begin by estimating the duration of the infectious period (see Supplement, Contact Investigations). The highest priority for evaluation should be given to 1) persons with a medical risk factor for TB disease (e.g., HIV infection or immunosuppressive therapy); 2) infants and children <4 years; 3) household or congregate setting contacts; and 4) persons present during medical procedures (e.g., bronchoscopies, sputum induction, or autopsies). In addition, offer TB screening to all persons named by the patient as work or social contacts during the infectious period. Determining whether to broaden the investigation will depend on whether evidence of transmission to any of the above contacts exists (positive TST or BAMT results or conversions), the duration of the potential exposure, and the intensity of the exposure (e.g., in a poorly ventilated environment versus outdoors). If the exposure was to pulmonary TB that was cavitary on chest radiograph or if the patient had positive AFB sputum smear results, usually the minimum exposure duration for a person to be considered a contact would be shorter. Nonetheless, infection with M. tuberculosis requires some degree of prolonged or regular exposure (i.e., days to weeks, not just a few hours).
If an HCW in a setting has a latex allergy, should this person receive a TST? A person with a latex allergy can receive a TST when latex-free products are used. Latex allergy can be a contraindication to skin testing if the allergy is severe and the products used to perform the test (e.g., syringe plungers, PPD antigen bottle stopper, and gloves) contain latex. Latex-free products are, however, usually available. If a person with a latex allergy does have a TST performed using products or equipment that contain latex, interpretation of the TST results can be difficult, because the TST reaction might be the result of the latex allergy, reaction to PPD, or a combination of both. Consider repeating the TST using latex-free products or use BAMT.
Should the TST site be covered with an adhesive bandage? No, avoid covering the TST site with anything that might interfere with reading the TST result (e.g., adhesive bandages, cream, ointment, lotion, liquids, and medication).
When can a TST be placed if other vaccines are also being administered (e.g., measles, varicella, yellow fever, and smallpox)? A TST should be administered either on the same day as vaccination with live virus or 4–6 weeks later. Vaccines that might cause a false-negative TST result are measles, varicella, yellow fever, smallpox, BCG, mumps, rubella, oral polio, oral typhoid, and live-attenuated influenza.
How frequently should persons in the general public receive TST? Testing for LTBI in the general public is not necessary unless the person is at risk for exposure to M. tuberculosis (e.g., someone who had contact with a person with TB disease) or at increased risk for progression to TB disease (e.g., someone infected with HIV).
Should we use a multiple puncture (Tine®) skin test to perform a TST? No, in the United States, the Mantoux method of skin testing is the preferred method because it is more accurate than Tine(r) skin tests. BAMT (currently QFT-G) is also now recommended as a test for M. tuberculosis infection.
What steps should be taken if an HCW has a baseline TST result of 16 mm and 1 year later the TST result was read as 0 mm? If documentation existed for the 16 mm result, administering another TST to the HCW subsequently was not necessary. One or both of these TST results could be false results. The first result might have been documented as 16 mm, but perhaps 16 mm of erythema was measured and no induration was present. The second result of 0 mm might have been caused by incorrect administration of the TST (i.e., too deeply or too shallow), or was read and recorded incorrectly (if it was actually positive). In this instance, another TST should be placed, or a BAMT should be offered, or if TB disease is suspected, a chest radiograph should be performed.
What steps should be taken if the TST is administered intramuscularly instead of intradermally? QC for administering TST is critical. If the TST is administered intramuscularly (too deeply), repeat the skin test immediately, or offer BAMT.
How are annual TST conversion rates for HCWs calculated? A TST conversion is a change in the result of a test for M. tuberculosis infection wherein the condition is interpreted as having progressed from uninfected to infected. Annual TST conversion rates are calculated for a given year by dividing the number of test conversions among HCWs in the setting that year (numerator) by the total number of HCWs who received tests in the setting that year (denominator) multiplied by 100. By calculating annual TST conversion rates, year-to-year comparisons can be used to identify transmission of M. tuberculosis that was not previously detected.
Where can PPD be obtained? Local and state health departments can provide PPD antigen for TST without charge to selected targeted testing and treatment programs. Purchase of the antigen and supplies is regulated by local and state laws related to professional licensure.
Where can millimeter rulers be obtained to measure TST results? A TST training kit, which includes a TST training video, guide for facilitators, and a TST millimeter ruler is available free of charge from CDC (https://www2.cdc.gov/nchstp_od/PIWeb/TBorderform.asp). In addition, check with your local or state health department and TST antigen manufacturers.
Where can materials be obtained for educating HCWs regarding TB? A list of TB websites and resources is available (Appendix E). Local or state health departments should have additional materials and access to resources and might be able to help develop a setting-specific TB education program.
Where can self-reading TST cards be obtained that allow HCWs to report their own results? HCWs and patients should not be allowed to read and report their own TST results; therefore, self-reading cards for reporting TST results are not recommended. All TST results should be read and recorded by a trained TST reader other than the person on whom the TST was placed.
Treatment for LTBI
Who should be treated for LTBI? Persons with LTBI who are at increased risk for developing TB disease should be offered treatment for LTBI regardless of age, if they have no contraindication to the medicine.
What are contraindications to treatment of LTBI? Active hepatitis and ESLD are contraindications to the use of INH for treatment of LTBI. Persons who have these conditions might be eligible for rifampin for 4 months for treatment of LTBI. Because of the substantial and complex drug-drug interactions between rifamycins and HIV protease inhibitors (PI) and nonnucleoside reverse transcriptase inhibitors (NNRTI), clinicians are encouraged to seek expert advice if the concurrent use of these drugs is being considered in persons infected with HIV. Information regarding use of these drugs is available at http://www.cdc.gov/nchstp/tb/tb_hiv_drugs/toc.htm.
Do persons need to be in a specific age range to be eligible for treatment of LTBI? No age restriction for eligibility of treatment for LTBI currently exists. Targeted TST programs should be conducted for persons at high risk, and these programs are discouraged for persons or settings considered to be low risk. However, for infection-control programs that conduct TB screening that includes HCWs who are frequently at low risk, proper medical evaluation needs to be conducted when an HCW with a positive TST result is identified. In this context, age might be a factor in the decision to administer treatment, because older persons are at increased risk for hepatic toxicity caused by INH.
What is the preferred regimen for treatment of LTBI? Nine months of daily INH is the preferred treatment regimen for patients who have LTBI. The 6-month regimen of INH or the 4-month regimen of rifampin are also acceptable alternatives.
Why is the 2-month regimen of RZ generally not offered for treatment of LTBI? Although the 2-month regimen of RZ was previously recommended as an option for the treatment of LTBI, reports of severe liver injury and death prompted the American Thoracic Society and CDC to revise recommendations to indicate that this regimen should generally not be offered for treatment of LTBI.
Can sputum specimens collected over a 2-day period that are reported as negative for AFB be used to exclude a diagnosis of TB disease? Yes, airborne precautions can be discontinued when infectious TB disease is considered unlikely and either 1) another diagnosis is made that explains the clinical syndrome or 2) the patient has three negative AFB sputum smear results (109–112). Each of the three consecutive sputum specimens should be collected 8–24 hours apart (124), and at least one specimen should be an early morning specimen, because respiratory secretions pool overnight. Generally, this method will allow patients with negative sputum smear results to be released from airborne precautions in 2 days.
When does an infectious TB patient become noninfectious? Historically, health-care professionals have believed that the effect of antituberculosis treatment to reduce infectiousness was virtually immediate; older texts state that patients on antituberculosis treatment are not infectious. Surrogates that are used for noninfectiousness include conversion of positive sputum AFB results to negative AFB results and clinical response to antituberculosis treatment (i.e., improvement of symptoms and chest radiograph result).
Risk Assessment
In certain health-care settings (e.g., outpatient clinics or emergency medical settings) where patients are evaluated before a hospitalization during which TB disease is diagnosed, determining the number of TB patients who were encountered can be difficult. How should the risk classification be assigned? These situations underscore the importance of obtaining an accurate patient history, completing contact investigations for all persons with suspected or confirmed TB disease, and ensuring effective communication to all settings in which persons with TB disease are encountered before diagnosis. Collaboration between infection-control personnel at the setting and the TB-control program staff at the local health department can help with this estimation.
At a pediatric hospital, the parents are normally with the child at the time of the TB diagnosis, and the parents can be diagnosed with TB disease at the same time as the child. To determine the number of patients diagnosed at the health-care setting, should the parents with TB disease who are visiting also be included in the total TB patient count? Only patients with TB disease who were evaluated or treated in the health-care setting count, not visitors who have TB (unless they were diagnosed at the same setting).
In a 160-bed hospital, three HCWs have had TST conversions during a 2-month period, which is usually the number of TST conversions detected in the hospital in 1 year. Should the setting be classified as potential ongoing transmission? If the HCWs with TST conversions can be linked together in some way, either through a job type, location of work, or DNA fingerprinting, then the classification of potential ongoing transmission might apply to one group of HCWs or one part of the setting. Evidence of ongoing transmission in this setting appears to exist, and a problem evaluation should be conducted to ascertain the reason for the TST conversions (see Problem Evaluation). Reasons could range from an undiagnosed case of TB in the setting to incorrect placement or reading of TST. Early consultation with the local health department and an expert in TB infection control might be helpful in identifying and resolving the problem.
If a health-care setting has a risk classification of potential ongoing transmission, how long should that classification be applied? The classification of potential ongoing transmission should be assigned only on a temporary basis and always warrants a problem evaluation (see Problem Evaluation). After resolution of problems, settings with a classification of potential ongoing transmission should be reclassified as a medium-risk classification for at least 1 year.
Environmental Controls
What is the difference between environmental controls and engineering controls ? "Environmental controls" is a more inclusive term than "engineering controls". Examples of environmental controls are UVGI, HEPA filters and AII rooms. Examples of engineering controls are local exhaust ventilation (e.g., booths, hoods, and tents) and general ventilation (including directional airflow and negative pressure).
Is an AII room the same as a negative-pressure isolation room? "AII room" is an accepted term and is used in the AIA guidelines that describe the purpose for and details of ventilation of AII rooms. An AII room is a special negative-pressure room for the specific purpose of isolating persons who might have suspected or confirmed infectious TB disease from other parts of the setting. Not all negative-pressure rooms are AII rooms, because they might not have the required air flow or differential pressure of an AII room.
Our TB clinic only treats persons with LTBI. Do we need an AII room and a respiratory-protection program? Ideally, yes, because persons with LTBI are at risk for developing TB disease. TB clinics usually should have at least one AII room and a respiratory-protection program. An AII room and a respiratory-protection program might not be needed if 1) each person treated in the clinic will be adequately screened before admission and are determined to not have TB disease, 2) a system exists to promptly detect and triage persons who have symptoms or signs of TB disease, and 3) no cough-inducing procedures will ever be performed in the clinic.
Can airborne precautions be discontinued for a patient with suspected TB disease who has positive AFB sputum smear results but has a negative NAA for M. tuberculosis? Yes, if the NAA test result is negative and dual infection with M. tuberculosis and another mycobacterial species is not clinically suspected, the patient may be released from airborne precautions. An NAA test is highly sensitive and specific for the identification of M. tuberculosis when performed properly on a patient who has a positive AFB sputum smear result.
During the winter months at a hospital, inadequate numbers of AII rooms are available for all patients with suspected or confirmed infectious TB disease. Can only two negative sputum smear results be obtained for AFB before releasing patients from airborne precautions? In general, the criterion for the release of a patient with suspected infectious TB disease from airborne precautions is that infectious TB disease is considered unlikely and either 1) another diagnosis is made that explains the clinical syndrome or 2) the patient has three negative AFB sputum smear results (109–112). Each of the three consecutive sputum specimens should be collected 8–24 hours apart (124), and at least one specimen should be an early morning specimen. Generally, this method will allow patients with negative sputum smear results to be released from airborne precautions in 2 days. If the number of AII rooms in the setting is inadequate, consider adding one or more AII rooms. Before undertaking this expense, however, ensure that the criteria for placing patients in AII rooms are correct and that the available rooms are not being used for patients in whom infectious TB disease is not suspected. In addition, the following intervals should be reviewed to identify any delays that could be corrected and decrease time for patients in AII rooms: 1) time between admission and ordering of sputum specimens for AFB examination, 2) time between ordering and collecting specimens, and 3) time between collection of specimens and receipt of results from the laboratory.
How many AII rooms are required in a 120-bed hospital? For a hospital with 120 beds, a minimum of one AII room is needed. Although no available data exist to quantify the number of rooms needed for a given number of cases of suspected or confirmed TB disease, a reasonable choice is one additional AII room for every 200 patient-days of cases of suspected or confirmed TB disease. The setting's risk assessment will help determine the number of AII rooms needed.
Who is responsible for ensuring that negative pressure is achieved in AII rooms? Ensuring that negative pressure is achieved in AII rooms is a function of the infection-control program at each health-care setting. This responsibility may be delegated to engineering, maintenance, or other appropriate staff to perform the actual negative pressure tests. AII rooms should be checked for negative pressure before occupation by a patient with suspected or confirmed infectious TB disease, and when in use by a person with TB disease, negative pressure should be checked daily with smoke tubes or other visual checks.
What is the difference between VAV and CAV? How do I determine which settings need them? VAV is variable air volume, and CAV is constant air volume. These terms refer to how the ventilation system is designed to deliver air to and maintain temperature and relative humidity control within a room. CAV systems usually are best for AII rooms and other negative-pressure rooms, because the negative-pressure differential is easier to maintain. VAV systems are acceptable if provisions are made to maintain the minimum total and outside ACH and a negative pressure ≥0.01 inch of water gauge relative to adjacent areas at all times.
Why was the differential pressure requirement for an AII room increased from 0.001 inch of water gauge to ≥0.01 inch of water gauge? In an ideal, controlled environment, 0.001 inches of water gauge has been demonstrated to ensure negative pressure in AII rooms. However, AIA and other organizations have demonstrated that a minimum of 0.01 inches of water gauge is needed in certain installations to ensure that negative pressure is consistently achieved.
How can a portable HEPA filter unit help control TB? Portable HEPA filtration units recirculate room air, and the HEPA filters effectively remove all particles from the air in the size range of droplet nuclei, resulting in a dilution of the concentration of infectious particles in the room.
Respiratory Protection
What is the difference between a CDC/NIOSH-certified respirator and a surgical or procedure mask? Respirators are designed to help reduce the wearer's (i.e., HCW's) exposure to airborne particles. The primary purpose of a surgical or procedure mask is to help prevent biologic particles from being expelled into the air by the wearer (i.e., patient).
How important is the fit of the respirator? This step is critical. The fit of a respirator is substantially important. If a respirator does not fit tightly on the face, airborne hazards can penetrate or enter underneath the facepiece seal and into the breathing zone. Before each use, the wearer of a respirator should perform a user-seal check on themselves to minimize contaminant leakage into the facepiece (http://www.cdc.gov/niosh/topics/respirators).
How do I perform a respirator user-seal check? Performing a user-seal check (formerly called "fit check") after redonning the respirator each time is critical to ensure adequate respiratory protection. The seal checks for respirators are described in the respirator user instructions and should be consulted before the respirator is used. The two types of user-seal checks usually are positive-pressure and negative-pressure checks.
To check positive pressure seal after donning the respirator, the wearer should cover the surface of the respirator with their hands or with a piece of household plastic film and exhale gently. If air is felt escaping around the facepiece, the respirator should be repositioned, and the user-seal check should be performed again. If the wearer does not feel air escaping around the facepiece, the positive pressure user-seal check was successful.
To check the negative pressure seal after donning the respirator, the wearer should cover the surface of the respirator and gently inhale, which should create a vacuum, causing the respirator to be drawn in toward the face. If the respirator is not drawn in toward the face or if the wearer feels air leaking around the face seal, the respirator should be removed and examined for any defects (e.g., a small hole or poor molding of the respirator to the face [especially around the nose area]). If no holes are found, the respirator should be repositioned and readjusted, and a second attempt at negative pressure user-seal check should be made. If the check is not successful, try a new respirator.
Is performing a user-seal check (formerly called "fit check") on a respirator before each use always necessary? Yes, performing a user-seal check on respirators before each use is essential to minimize contaminant leakage into the facepiece. Each respirator manufacturer has a recommended user-seal check procedure that should be followed by the user each time the respirator is worn.
What is a respirator fit test and who does fit testing? A fit test is used to determine which respirator does or does not fit the user adequately and to ensure that the user knows when the respirator fits properly. Fit testing must be performed by a qualified health professional. Fit testing should be performed during the initial respiratory-protection program training and periodically thereafter, based on the risk assessment for the setting and in accordance with applicable federal, state, or local regulations.
Periodic fit testing for respirators used in TB environments can serve as an effective training tool in conjunction with the content included in employee training and retraining. The frequency of fit testing should be determined by a change in the 1) risk for transmission of M. tuberculosis, 2) facial features of the wearer, 3) medical condition that would affect respiratory function, 4) physical characteristics of the respirator (despite the same model number), or 5) model or size of the assigned respirator.
What kind of respiratory protection should HCWs use when providing care to persons with suspected or confirmed infectious TB disease in the home? The recommended respiratory protection for HCWs who provide care in the homes of patients with suspected or confirmed infectious TB disease is at least an N95 respirator.
What kind of respiratory protection should HCWs use when transporting patients with suspected or confirmed infectious TB disease? The risk assessment for the setting should consider the potential for shared air. Drivers, HCWs and other staff who are transporting patients with suspected or confirmed infectious TB disease in an enclosed vehicle should consider wearing an N95 disposable respirator. If the patient has symptoms or signs of infectious TB disease (e.g., productive cough or positive AFB sputum smear result), the patient should wear a surgical or procedure mask, if possible, during transport, in waiting areas, or when other persons are present. Patients who cannot tolerate masks because of medical conditions should observe strict respiratory hygiene and cough etiquette procedures.
What type of respiratory protection should be used in the operating room (OR) by HCWs with facial hair or other factors that preclude proper fitting of an N95 respirator? Will wearing a surgical or procedure mask underneath a PAPR solve this problem? HCWs with facial hair should not wear negative pressure respirators (e.g., N95 disposable respirators that require a tight faceseal). In the OR, HCWs with facial hair who are caring for a person with suspected or confirmed infectious TB disease should consult their infection-control committee and respirator manufactures regarding optimal respiratory protection and adequate infection-control measures. The HCW in this case might wear a surgical or procedure mask to protect the surgical field underneath a loose-fitting PAPR. However, the user cannot be assured of proper operation unless the PAPR's manufacturer tested the PAPR over a surgical or procedure mask or N95 respirator. All respiratory-protection equipment should be used in accordance with the manufacturer's instructions.
Should bacterial filters be used routinely on the breathing circuits of all ventilators and anesthesia equipment on patients with suspected or confirmed infectious TB disease? Yes, bacterial filters should be used routinely on the exhalation breathing circuits of patients with suspected or confirmed infectious TB disease to prevent exhaled air containing infectious droplet nuclei from contaminating the room air. Filters should be used on mechanical ventilators and also on hand-held ventilating bags (i.e., manual resuscitators [e.g., ambu-bags®]). The bacterial filter should be specified by the manufacturer to filter particles 0.3 µm in both the unloaded and the loaded states, with a filter efficiency of ≥95% (i.e., filter penetration of <5%) at the maximum design flow rates of the ventilator.
Who should not wear an N95 respirator? Any HCW who is restricted from using a respirator because of medical reasons should not wear one nor should persons who cannot pass a fit test because of the presence of facial hair or other condition that interferes with the seal of the respirator to the face.
How long can I use my respirator for TB exposures before I discard it? Disposable respirators can be functional for weeks to months and reused by the same HCW. Reuse is limited by hygiene, damage, and breathing resistance, and manufacturer instructions should be considered.
Should persons who perform maintenance on and replace filters on any ventilation system that is likely to be contaminated with M. tuberculosis wear a respirator? Laboratory studies indicate that re-aerosolization of viable mycobacteria from HEPA filters and N95 disposable respirator filter media is unlikely under normal conditions; however, the risks associated with handling loaded HEPA filters in ventilation systems under field-use conditions have not been evaluated. Therefore, persons performing maintenance and replacing filters on any ventilation system that is likely to be contaminated with M. tuberculosis should wear a respirator (see Respiratory Protection) and adhere to local recommendations for eye protection and gloves.
Cough-Inducing and Aerosol-Generating Procedures
Should a bronchoscopic procedure be performed on a patient with TB disease? If possible, bronchoscopic procedures should be avoided for patients with 1) a clinical syndrome consistent with infectious pulmonary or laryngeal TB disease and 2) in persons with positive AFB sputum smear results, because bronchoscopic procedures substantially increase the risk for transmission either through an airborne route or a contaminated bronchoscope. If the diagnosis of TB is suspected, consideration should be given to empiric antituberculosis treatment, but a bronchoscopic procedure might have the advantage of confirmation of the diagnosis with histologic specimens; collection of additional specimens, including post bronchoscopy sputum, can increase the diagnostic yield and increase the opportunity to confirm an alternate diagnosis. Microscopic examination of three consecutive sputum specimens obtained at least 8 hours apart is recommended instead of bronchoscopy.
For ORs without an AII room, postoperative recovery is usually in the OR suite. Is this location acceptable? If the OR has an anteroom, this location is acceptable. Reversible flow rooms (OR or isolation) are not recommended by CDC, AIA, or ASHRAE.
Acknowledgments
The authors acknowledge contributions from leaders of substantial medical, scientific, public health and labor organizations, and other experts in the fields of TB, HIV/AIDS, infection control, hospital epidemiology, microbiology, ventilation, industrial hygiene, nursing, dental practice, and emergency medical services.
Bennett CL, Schwartz DN, Parada JP, et al. Delays in tuberculosis isolation and suspicion among persons hospitalized with HIV-related pneumonia. Chest 2000;117:110–6.
Greenaway C, Menzies D, Fanning A, et al. Delay in diagnosis among hospitalized patients with active tuberculosis—predictors and outcomes. Am J Respir Crit Care Med 2002;165:927–33.
CDC. Guidelines for prevention of TB transmission in hospitals. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 1982.
Fridkin SK, Manangan L, Bolyard E, Jarvis WR. Society for Healthcare Epidemiology of America. SHEA-CDC TB survey, part I: status of TB infection control programs at member hospitals, 1989–1992. Infect Control Hosp Epidemiol 1995;16:129–34.
Fridkin SK, Manangan L, Bolyard E, Jarvis WR. Society for Healthcare Epidemiology of America. SHEA-CDC TB survey, part II: efficacy of TB infection control programs at member hospitals, 1992. Society for Healthcare Epidemiology of America. Infect Control Hosp Epidemiol 1995;16:135–40.
Institute of Medicine. Tuberculosis in the workplace. Washington, DC: National Academy Press; 2001.
Kellerman SE, Simonds D, Banerjee S, Towsley J, Stover BH, Jarvis W. APIC and CDC survey of Mycobacterium tuberculosis isolation and control practices in hospitals caring for children. Part 1: patient and family isolation policies and procedures. Am J Infect Control 1998;26:478–82.
Kellerman SE, Simonds D, Banerjee S, Towsley J, Stover BH, Jarvis W. APIC and CDC survey of Mycobacterium tuberculosis isolation and control practices in hospitals caring for children. Part 2: environmental and administrative controls. Am J Infect Control 1998;26:483–7.
Manangan LP, Simonds DN, Pugliese G, et al. Are US hospitals making progress in implementing guidelines for prevention of Mycobacterium tuberculosis transmission? Arch Intern Med 1998;158:1440–4.
Manangan LP, Collazo ER, Tokars J, Paul S, Jarvis WR. Trends in compliance with the guidelines for preventing the transmission of Mycobacterium tuberculosis among New Jersey hospitals, 1989 to 1996. Infect Control Hosp Epidemiol 1999;20:337–40.
Manangan LP, Bennett CL, Tablan N, et al. Nosocomial tuberculosis prevention measures among two groups of US hospitals, 1992 to 1996. Chest 2000;117:380–4.
Fella P, Rivera P, Hale M, Squires K, Sepkowitz K. Dramatic decrease in tuberculin skin test conversion rate among employees at a hospital in New York City. Am J Infect Control 1995;23:352–6.
Louther J, Rivera P, Feldman J, Villa N, DeHovitz J, Sepkowitz KA. Risk of tuberculin conversion according to occupation among health care workers at a New York City hospital. Am J Respir Crit Care Med 1997;156:201–5.
Maloney SA, Pearson ML, Gordon MT, Del Castillo R, Boyle JF, Jarvis WR. Efficacy of control measures in preventing nosocomial transmission of multidrug-resistant tuberculosis to patients and health care workers. Ann Intern Med 1995;122:90–5.
Stroud LA, Tokars JI, Grieco MH, et al. Evaluation of infection control measures in preventing the nosocomial transmission of multidrug-resistant Mycobacterium tuberculosis in a New York City hospital. Infect Control Hosp Epidemiol 1995;16:141–7.
Wenger PN, Otten J, Breeden A, Orfas D, Beck-Sague CM, Jarvis WR. Control of nosocomial transmission of multidrug-resistant Mycobacterium tuberculosis among healthcare workers and HIV-infected patients. Lancet 1995;345:235–40.
Cook S, Maw KL, Munsiff SS, Fujiwara PI, Frieden TR. Prevalence of tuberculin skin test positivity and conversions among healthcare workers in New York City during 1994 to 2001. Infect Control Hosp Epidemiol 2003;24:807–13.
McCray E, Weinbaum CM, Braden CR, Onorato IM. The epidemiology of tuberculosis in the United States. Clin Chest Med 1997;18:99–113.
Blumberg HM, Watkins DL, Berschling JD, et al. Preventing the nosocomial transmission of tuberculosis. Ann Intern Med 1995;122:658–63.
Tokars JI, McKinley GF, Otten J, et al. Use and efficacy of tuberculosis infection control practices at hospitals with previous outbreaks of multidrug-resistant tuberculosis. Infect Control Hosp Epidemiol 2001;22:449–55.
CDC. Reported tuberculosis in the United States, 2004. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2005.
Horsburgh CR, Moore M, Castro KG. Epidemiology of tuberculosis in the United States. In: Rom WN, Garay SM, eds. Tuberculosis. 2 ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2004:31–45.
Institute of Medicine. Ending neglect: the elimination of tuberculosis in the United States. Washington, DC: National Academy Press; 2000.
Culver DA, Gordon SM, Mehta AC. Infection control in the bronchoscopy suite: a review of outbreaks and guidelines for prevention. Am J Respir Crit Care Med 2003;167:1050–6.
American Thoracic Society, CDC, Infectious Disease Society of America. Diagnostic standards and classification of tuberculosis in adults and children. Am J Respir Crit Care Med 2000;161:1376–95.
Wells WF. Aerodynamics of droplet nuclei [Chapter 3]. In: Airborne contagion and air hygiene. Cambridge, MA: Harvard University Press; 1955:13–9.
Canetti G. The Tubercle bacillus in the pulmonary lesion of man: Histobacteriology and its bearing on the therapy of pulmonary tuberculosis. New York, NY: Springer Publishing Company, Inc.; 1955.
US Department of Health and Human Services. The health consequences of smoking: a report of the Surgeon General. Atlanta, GA: US Department of Health and Human Services, CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2004.
Buskin SE, Gale JL, Weiss NS, Nolan CM. tuberculosis risk factors in adults in King County, Washington, 1988 through 1990. Am J Public Health 1994;84:1750–6.
CDC. Core curriculum on tuberculosis: what every clinician should know. 4 ed. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2000.
Leonhardt KK, Gentile F, Gilbert BP, Aiken M. A cluster of tuberculosis among crack house contacts in San Mateo County, California. Am J Public Health 1994;84:1834–6.
McElroy PD, Southwick KL, Fortenberry ER, et al. Outbreak of tuberculosis among homeless persons coinfected with human immunodeficiency virus. Clin Infect Dis 2003;36:1305–12.
McElroy PD, Rothenberg RB, Varghese R, et al. A network-informed approach to investigating a tuberculosis outbreak: implications for enhancing contact investigations. Int J Tuberc Lung Dis 2003;7:S486–S493.
Reyes JC, Robles RR, Colon HM, Marrero CA, Castillo X, Melendez M. Mycobacterium tuberculosis infection among crack and injection drug users in San Juan, Puerto Rico. PR Health Sci J 1996;15:233–6.
Taubes T, Galanter M, Dermatis H, Westreich L. Crack cocaine and schizophrenia as risk factors for PPD reactivity in the dually diagnosed. Journal of Addictive Diseases 1998;17:63–74.
Howard TP, Solomon DA. Reading the tuberculin skin test: who, when, and how? Arch Intern Med 1988;148:2457–9.
Daley CL, Small PM, Schecter GF, et al. An outbreak of tuberculosis with accelerated progression among persons infected with the human immunodeficiency virus. An analysis using restriction-fragment-length polymorphisms. N Engl J Med 1992;326:231–5.
Dooley SW, Villarino ME, Lawrence M, et al. Nosocomial transmission of tuberculosis in a hospital unit for HIV-infected patients. JAMA 1992;267:2632–4.
Edlin BR, Tokars JI, Grieco MH, et al. An outbreak of multidrug-resistant tuberculosis among hospitalized patients with the acquired immunodeficiency syndrome. N Engl J Med 1992;326:1514–21.
Kenyon TA, Ridzon R, Luskin-Hawk R, et al. A nosocomial outbreak of multidrug-resistant tuberculosis. Ann Intern Med 1997;127:32–6.
Colditz GA, Brewer TF, Berkey CS, et al. Efficacy of BCG vaccine in the prevention of tuberculosis: meta-analysis of the published literature. JAMA 1994;271:698–702.
Rodrigues LC, Diwan VK, Wheeler JG. Protective effect of BCG against tuberculous meningitis and miliary tuberculosis: a meta-analysis. Int J Epidemiol 1993;22:1154–8.
Barrett-Connor E. The epidemiology of tuberculosis in physicians. JAMA 1979;241:33–8.
Styblo K. Epidemiology of tuberculosis. The Hague, Netherlands: Royal Netherlands Tuberculosis Association (KNCV); 1991.
Catanzaro A. Nosocomial tuberculosis. Am Rev Respir Dis 1982;125:559–62.
Di Perri G, Cruciani M, Danzi MC, et al. Nosocomial epidemic of active tuberculosis among HIV-infected patients. Lancet 1989;2:1502–4.
Koppaka VR, Ridzon R. Prevention and control of the nosocomial transmission of Mycobacterium tuberculosis. In: Wenzel RP, ed. Prevention and control of nosocomial infections. 4 ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003:229–52.
Ehrenkranz NJ, Kicklighter JL. Tuberculosis outbreak in a general hospital: evidence for airborne spread of infection. Ann Intern Med 1972;77:377–82.
Goldman KP. Tuberculosis in hospital doctors. Tubercle 1988;69:237–40.
Haley CE, McDonald RC, Rossi L, Jones WD Jr, Haley RW, Luby JP. Tuberculosis epidemic among hospital personnel. Infect Control Hosp Epidemiol 1989;10:204–10.
Hutton MD, Stead WW, Cauthen GM, Bloch AB, Ewing WM. Nosocomial transmission of tuberculosis associated with a draining abscess. J Infect Dis 1990;161:286–95.
Jereb JA, Klevens RM, Privett TD, et al. Tuberculosis in health care workers at a hospital with an outbreak of multidrug-resistant Mycobacterium tuberculosis. Arch Intern Med 1995;155:854–9.
Kantor HS, Poblete R, Pusateri SL. Nosocomial transmission of tuberculosis from unsuspected disease. Am J Med 1988;84:833–8.
Lundgren R, Norrman E, Asberg I. Tuberculosis infection transmitted at autopsy. Tubercle 1987;68:147–50.
McGowan JE Jr. Nosocomial tuberculosis: new progress in control and prevention. Clin Infect Dis 1995;21:489–505.
Menzies D, Fanning A, Yuan L, Fitzgerald M. tuberculosis among health care workers. N Engl J Med 1995;332:92–8.
Menzies D, Fanning A, Yuan L, FitzGerald JM, Canadian Collaborative Group in Nosocomial Transmission of Tuberculosis. Factors associated with tuberculin conversion in Canadian microbiology and pathology workers. Am J Respir Crit Care Med 2003;167:599–602.
Sepkowitz KA, Friedman CR, Hafner A, et al. Tuberculosis among urban health care workers: a study using restriction fragment length polymorphism typing. Clin Infect Dis 1995;21:1098–1012.
Templeton GL, Illing LA, Young L, Cave D, Stead WW, Bates JH. The risk for transmission of Mycobacterium tuberculosis at the bedside and during autopsy. Ann Intern Med 1995;122:922–5.
Zaza S, Blumberg HM, Beck-Sague C, et al. Nosocomial transmission of Mycobacterium tuberculosis: role of health care workers in outbreak propagation. J Infect Dis 1995;172:1542–9.
Anonymous. HazardAlert! Clusters of "positive PPD skin tests" due to intradermal injection of Td. NurseAdvice-ERR 2003;1:2.
Larson JL, Lambert L, Stricof RL, Driscoll J, McGarry MA, Ridzon R. Potential nosocomial exposure to Mycobacterium tuberculosis from a bronchoscope. Infect Control Hosp Epidemiol 2003;24:825–30.
Weber DJ, Rutala WA. Lessons from outbreaks associated with bronchoscopy. Infect Control Hosp Epidemiol 2001;22:403–8.
Srinivasan A, Wolfenden LL, Song X, Perl TM, Haponik EF. Bronchoscope reprocessing and infection prevention and control: bronchoscopy-specific guidelines are needed. Chest 2004;125:307–14.
D'Agata EM, Wise S, Stewart A, Lefkowitz LB Jr. Nosocomial transmission of Mycobacterium tuberculosis from an extrapulmonary site. Infect Control Hosp Epidemiol 2001;22:10–2.
Ball R, Van Wey M. tuberculosis skin test conversion among health care workers at a military medical center. Military Medicine 1997;162:338–43.
Menzies D, Fanning A, Yuan L, FitzGerald JM, Canadian Collaborative Group in Nosocomial Transmission of Tuberculosis. Hospital ventilation and risk for tuberculous infection in Canadian health care workers. Canadian Collaborative Group in Nosocomial Transmission of TB. Ann Intern Med 2000;133:779–89.
Williams J, Schneider N, Gilligan ME. Implementing a tuberculosis control program. Am J Infect Control 1995;23:152–5.
Beck-Sague C, Dooley SW, Hutton MD, et al. Hospital outbreak of multidrug-resistant Mycobacterium tuberculosis infections. Factors in transmission to staff and HIV-infected patients. JAMA 1992;268:1280–6.
Dooley SW, Jarvis WR, Martone WJ, Snider DE Jr. Multidrug-resistant tuberculosis. Ann Intern Med 1992;117:257–9.
Pearson ML, Jereb JA, Frieden TR, et al. Nosocomial transmission of multidrug-resistant Mycobacterium tuberculosis. A risk to patients and health care workers. Ann Intern Med 1992;117:191–6.
Larsen NM, Biddle CL, Sotir MJ, White N, Parrott P, Blumberg HM. Risk for tuberculin skin test conversion among health care workers: occupational versus community exposure and infection. Clin Infect Dis 2002;35:796–801.
Moro ML, Errante I, Infuso A, et al. Effectiveness of infection control measures in controlling a nosocomial outbreak of multidrug-resistant tuberculosis among HIV patients in Italy. Int J Tuberc Lung Dis 2000;4:61–8.
Panlilio AL, Burwen DR, Curtis AB, et al. Tuberculin skin testing surveillance of health care personnel. Clin Infect Dis 2002;35:219–27.
Fuss EP, Israel E, Baruch N, Roghmann MC. Improved tuberculosis infection control practices in Maryland acute care hospitals. Am J Infect Control 2000;28:133–7.
Stricof RL, DiFerdinando GT Jr, Osten WM, Novick LF. Tuberculosis control in New York City hospitals. Am J Infect Control 1998;26:270–6.
Lambert L, Rajbhandary S, Qualls N, et al. Costs of implementing and maintaining a tuberculin skin test program in hospitals and health departments. Infect Control Hosp Epidemiol 2003;24:814–20.
Askew GL, Finelli L, Hutton M, et al. Mycobacterium tuberculosis transmission from a pediatrician to patients. Pediatrics 1997;100:19–23.
Moore M, Schulte J, Valway SE, et al. Evaluation of transmission of Mycobacterium tuberculosis in a pediatric setting. J Pediatr 1998;133:108–12.
Schulte JM, Moore M, Kistler V, et al. Tuberculosis screening in private physicians' offices, Pennsylvania, 1996. Am J Prev Med 1999;16:178–81.
Lobato MN, Roberts CA, Bazerman LB, Hammett TM. Public health and correctional collaboration in tuberculosis control. Am J Prev Med 2004;27:112–7.
Reichard AA, Lobato MN, Roberts CA, Bazerman LB, Hammett TM. Assessment of tuberculosis screening and management practices of large jail systems. Public Health Rep 2003;118:500–7.
Fennelly KP, Nardell EA. The relative efficacy of respirators and room ventilation in preventing occupational tuberculosis. Infect Control Hosp Epidemiol 1998;19:754–9.
Joint Commission on Accreditation of Healthcare Organizations. 2005 Critical access hospitals: surveillance, prevention, and control of infection. Oak Brook, IL: Joint Commission Resources; 2005.
Al Zahrani K, Al Jahdali H, Poirier L, Rene P, Menzies D. Yield of smear, culture and amplification tests from repeated sputum induction for the diagnosis of pulmonary tuberculosis. Int J Tuberc Lung Dis 2001;5:855–60.
Conde MB, Soares SL, Mello FC, et al. Comparison of sputum induction with fiberoptic bronchoscopy in the diagnosis of tuberculosis: experience at an acquired immune deficiency syndrome reference center in Rio de Janeiro, Brazil. Am J Respir Crit Care Med 2000;162:2238–40.
Bell D, Leckie V, McKendrick M. The role of induced sputum in the diagnosis of pulmonary tuberculosis. J Infect 2003;47:317–21.
Merrick ST, Sepkowitz KA, Walsh J, Damson L, McKinley P, Jacobs JL. Comparison of induced versus expectorated sputum for diagnosis of pulmonary tuberculosis by acid-fast smear. Am J Infect Control 1997;25:463–6.
CDC. Effective TB interviewing for contact investigation. Atlanta, GA: US Department of Health and Human Services, CDC; 2004.
Food and Drug Administration. The selection of patients for x-ray examinations: chest x-ray screening examinations. Rockville, MD: US Department of Health and Human Services, Public Health Service, Food and Drug Administration; August 1983:26–9.
American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. Health care facilities [Chapter 7]. 2003 ASHRAE handbook: HVAC applications. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.; 2003:7.1–7.14.
American Institute of Architects. Guidelines for design and construction of hospital and health care facilities. Washington, DC: American Institute of Architects; 2001.
Francis J. Curry National Tuberculosis Center. Making the connection: an introduction to interpretation skills for TB control. San Francisco, CA: Francis J. Curry National Tuberculosis Center; 2003.
Piotrowski J. Respiratory etiquette. CDC's SARS draft plan suggests masks for patients. Mod Healthc 2003;33:13.
CDC. Key facts about the flu and flu vaccine. Atlanta, GA: US Department of Health and Human Services, CDC; 2004.
Leonard MK, Osterholt D, Kourbatova EV, Del Rio C, Wang W, Blumberg HM. How many sputum specimens are necessary to diagnose pulmonary tuberculosis? Am J Infect Control 2005;33:58–61.
Toman K. How many bacilli are present in a sputum specimen found positive by smear microscopy [Chapter 4]. In: Frieden T, ed. Toman's tuberculosis case detection, treatment, and monitoring: questions and answers. 2nd ed. Geneva, Switzerland: World Health Organization; 2004:11–3.
CDC. Update: nucleic acid amplification tests for tuberculosis. MMWR 2000;49:593–4.
Willcox PA, Potgieter PD, Bateman ED, Benatar SR. Rapid diagnosis of sputum negative miliary tuberculosis using the flexible fibreoptic bronchoscope. Thorax 1986;41:681–4.
Abadco DL, Steiner P. Gastric lavage is better than bronchoalveolar lavage for isolation of Mycobacterium tuberculosis in childhood pulmonary tuberculosis. Pediatr Infect Dis J 1992;11:735–8.
Abadco DL, Amaro-Galvez R, Rao M, Steiner P. Experience with flexible fiberoptic bronchoscopy with bronchoalveolar lavage as a diagnostic tool in children with AIDS. Am J Dis Child 1992;146:1056–9.
Chan S, Abadco DL, Steiner P. Role of flexible fiberoptic bronchoscopy in the diagnosis of childhood endobronchial tuberculosis. Pediatr Infect Dis J 1994;13:506–9.
Lillehei JP. Sputum induction with heated aerosol inhalations for the diagnosis of tuberculosis. Am Rev Respir Dis 1961;84:276–8.
Willcox PA, Benatar SR, Potgieter PD. Use of the flexible fibreoptic bronchoscope in diagnosis of sputum-negative pulmonary tuberculosis. Thorax 1982;37:598–601.
Djukanovic R, Sterk PJ, Fahy JV, Hargreave FE. Standardised methodology of sputum induction and processing. Eur Respir J 2002;37(Suppl):1S–2S.
Paggiaro PL, Chanez P, Holz O, Ind PW, Djukanovic R, Maestrelli P, Sterk PJ. Sputum induction. Eur Respir J 2002;37(Suppl):3S–8S.
Gibson PG, Grootendor DC, Henry RL, et al. Sputum induction in children. Eur Respir J 2002;20(Suppl 4):44S–46S.
Curtis AB, Ridzon R, Vogel R, et al. Extensive transmission of Mycobacterium tuberculosis from a child. N Engl J Med 1999;341:1491–5.
American Academy of Pediatrics. Tuberculosis. 26 ed. Elk Grove Village, IL: American Academy of Pediatrics; 2003:642–80.
Rabalais G, Adams G, Stover B. PPD skin test conversion in health-care workers after exposure to Mycobacterium tuberculosis infection in infants. Lancet 1991;338:826.
CDC, National Institutes of Health. Agent: Mycobacterium tuberculosis, M. bovis. In: Richmond JY, McKinley RW, eds. Biosafety in Microbiological and Biomedical Laboratories. 4 ed. Washington, DC: US Government Printing Office; 1999:105–6.
Association of State and Territorial Public Health Laboratory Directors, CDC. Mycobacterium tuberculosis: assessing your laboratory. Atlanta, GA: US Department of Health and Human Services, CDC; 1995.
Tenover FC, Crawford JT, Huebner RE, Geiter LJ, Horsburgh CR Jr, Good RC. The resurgence of tuberculosis: is your laboratory ready? J Clin Microbiol 1993;31:767–70.
Klein NC, Duncanson FP, Lenox TH III, Pitta A, Cohen SC, Wormser GP. Use of mycobacterial smears in the diagnosis of pulmonary tuberculosis in AIDS/ARC patients. Chest 1989;95:1190–2.
Pitchenik AE, Rubinson HA. The radiographic appearance of tuberculosis in patients with the acquired immune deficiency syndrome (AIDS) and pre-AIDS. Am Rev Respir Dis 1985;131:393–6.
Chaulk CP, Kazandjian VA. Directly observed therapy for treatment completion of pulmonary tuberculosis: consensus statement of the Public Health Tuberculosis Guidelines Panel. JAMA 1998;279:943–8. Erratum in: JAMA 1998;280:134.
Frieden TR, Fujiwara PI, Washko RM, Hamburg MA. Tuberculosis in New York City—turning the tide. N Engl J Med 1995;333:229–33.
Weis SE, Slocum PC, Blais FX, et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N Engl J Med 1994;330:1179–84.
Sokolove PE, Lee BS, Krawczyk JA, et al. Implementation of an emergency department triage procedure for the detection and isolation of patients with active pulmonary tuberculosis. Ann Emerg Med 2000;35:327–36.
Aranha-Creado H, Prince D, Greene K, Brandwein H. Removal of Mycobacterium species by breathing circuit filters. Infect Control Hosp Epidemiol 1997;18:252–4.
Berry AJ, Nolte FS. An alternative strategy for infection control of anesthesia breathing circuits: a laboratory assessment of the Pall HME Filter. Anesth Analg 1991;72:651–5.
Demers RR. Bacterial/viral filtration: let the breather beware! Chest 2001;120:1377–89.
Langevin PB, Rand KH, Layon AJ. The potential for dissemination of Mycobacterium tuberculosis through the anesthesia breathing circuit. Chest 1999;115:1107–14.
Tait AR. Occupational transmission of tuberculosis: implications for anesthesiologists. Anesth Analg 1997;85:444–51.
Teo DT, Lim TW. Transmission of tuberculosis from patient to healthcare workers in the anaesthesia context. Ann Acad Med Singapore 2004;33:95–9.
Kao AS, Ashford DA, McNeil MM, Warren NG, Good RC. Descriptive profile of tuberculin skin testing programs and laboratory-acquired tuberculosis infections in public health laboratories. J Clin Microbiol 1997;35:1847–51.
Peerbooms PG, van Doornum GJ, van Deutekom H, Coutinho RA, van Soolingen D. Laboratory-acquired tuberculosis. Lancet 1995;345:1311–2.
Garber E, San Gabriel P, Lambert L, Saiman L. A survey of latent tuberculosis infection among laboratory healthcare workers in New York City. Infect Control Hosp Epidemiol 2003;24:801–6.
Metchock BG, Nolte FS, Wallace RJ. Mycobacterium. In: Murray PR, Barron EJ, Pfaller MA, Tenover FC, Yolken RH, eds. Manual of Clinical Microbiology. 7 ed. Washington, DC: American Society for Microbiology; 1999:399–437.
Richmond JY. Anthology of biosafety: IV. Issues in public health. American Biological Safety Association; 2001.
CDC, National Institutes of Health. Primary containment for biohazards: selection, installation and use of biological safety cabinets. 2nd ed. Washington, DC: US Government Printing Office; 2000.
CDC, National Institutes of Health. Biosafety in microbiological and biomedical laboratories. 4th ed. Washington, DC: US Government Printing Office; 1999.
Mehta AC, Minai OA. Infection control in the bronchoscopy suite. A review. Clin Chest Med 1999;20:19–32.
Wang KP, Mehta AC. Flexible bronchoscopy. Blackwell Science, Inc.; 1995.
Jereb JA, Burwen DR, Dooley SW, et al. Nosocomial outbreak of tuberculosis in a renal transplant unit: application of a new technique for restriction fragment length polymorphism analysis of Mycobacterium tuberculosis isolates. J Infect Dis 1993;168:1219–24.
Agerton T, Valway S, Gore B, et al. Transmission of a highly drug-resistant strain (strain W1) of Mycobacterium tuberculosis. Community outbreak and nosocomial transmission via a contaminated bronchoscope. JAMA 1997;278:1073–7.
Leers WD. Disinfecting endoscopes: how not to transmit Mycobacterium tuberculosis by bronchoscopy. Can Med Assoc J 1980;123:275–80.
Michele TM, Cronin WA, Graham NM, et al. Transmission of Mycobacterium tuberculosis by a fiberoptic bronchoscope. Identification by DNA fingerprinting. JAMA 1997;278:1093–5.
Nelson KE, Larson PA, Schraufnagel DE, Jackson J. Transmission of tuberculosis by flexible fiberbronchoscopes. Am Rev Respir Dis 1983;127:97–100.
Ramsey AH, Oemig TV, Davis JP, Massey JP, Torok TJ. An outbreak of bronchoscopy-related Mycobacterium tuberculosis infections due to lack of bronchoscope leak testing. Chest 2002;121:976–81.
Spach DH, Silverstein FE, Stamm WE. Transmission of infection by gastrointestinal endoscopy and bronchoscopy. Ann Intern Med 1993;118:117–28.
Bar W, Marquez de Bar G, Naumann A, Rusch-Gerdes S. Contamination of bronchoscopes with Mycobacterium tuberculosis and successful sterilization by low-temperature hydrogen peroxide plasma sterilization. Am J Infect Control 2001;29:306–11.
Gershon RR, Vlahov D, Escamilla-Cejudo JA, et al. Tuberculosis risk in funeral home employees. J Occup Environ Med 1998;40:497–503.
Lauzardo M, Lee P, Duncan H, Hale Y. Transmission of Mycobacterium tuberculosis to a funeral director during routine embalming. Chest 2001;119:640–2.
McKenna MT, Hutton M, Cauthen G, Onorato IM. The association between occupation and tuberculosis. A population-based survey. Am J Respir Crit Care Med 1996;154:587–93.
Sterling TR, Pope DS, Bishai WR, Harrington S, Gershon RR, Chaisson RE. Transmission of Mycobacterium tuberculosis from a cadaver to an embalmer. N Engl J Med 2000;342:246–48.
Sugita M, Tsutsumi Y, Suchi M, Kasuga H, Ishiko T. Pulmonary tuberculosis. An occupational hazard for pathologists and pathology technicians in Japan. Acta Pathol Jpn 1990;40:116–27.
Ussery XT, Bierman JA, Valway SE, Seitz TA, DiFerdinando GT Jr, Ostroff SM. Transmission of multidrug-resistant Mycobacterium tuberculosis among persons exposed in a medical examiner's office, New York. Infect Control Hosp Epidemiol 1995;16:160–5.
Burton JL. Health and safety at necropsy. J Clin Pathol 2003;56:254–60.
American Conference of Governmental Industrial Hygienists. Industrial ventilation: a manual of recommended practice. 24 ed. Cincinnati, OH: American Conference of Governmental Industrial Hygienists; 2001.
Murthy BV, Pereira BJ. A 1990s perspective of hepatitis C, human immunodeficiency virus, and tuberculosis infections in dialysis patients. Semin Nephrol 1997;17:346–63.
Tokars JI, Miller B. Tuberculin skin testing of ESRD patients. Am J Kidney Dis 1997;30:456–7.
Ahmed AT, Karter AJ. Tuberculosis in California dialysis patients. Int J Tuberc Lung Dis 2004;8:341–5.
Simon TA, Paul S, Wartenberg D, Tokars JI. Tuberculosis in hemodialysis patients in New Jersey: a statewide study. Infect Control Hosp Epidemiol 1999;20:607–9.
Fang HC, Chou KJ, Chen CL, et al. Tuberculin skin test and anergy in dialysis patients of a tuberculosis-endemic area. Nephron 2002;91:682–7.
Duell RC, Madden RM. Droplet nuclei produced during dental treatment of tubercular patients. A preliminary study. Oral Surg Oral Med Oral Pathol 1970;30:711–6.
Naidoo S, Mahommed A. Knowledge, attitudes, behaviour and prevalence of TB infection among dentists in the western Cape. SADJ 2002;57:476–8.
Cleveland JL, Kent J, Gooch BF, et al. Multidrug-resistant Mycobacterium tuberculosis in an HIV dental clinic. Infect Control Hosp Epidemiol 1995;16:7–11.
Kohn WG, Harte JA, Malvitz DM, et al. Guidelines for infection control in dental health care settings—2003. J Am Dent Assoc 2004;135:33–47.
Asch S, Leake B, Knowles L, Gelberg L. Tuberculosis in homeless patients: potential for case finding in public emergency departments. Ann Emerg Med 1998;32:144–7.
Prezant DJ, Kelly KJ, Mineo FP, et al. Tuberculin skin test conversion rates in New York City Emergency Medical Service health care workers. Ann Emerg Med 1998;32:208–13.
Seitz TA, Decker J, Jensen PA. Health Hazard Evaluation Report: University of Medicine and Dentistry of New Jersey, University Hospital, Newark, NJ. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1996. Publication no. HETA 95-0031-2601.
Dickinson E. Exposures in EMS. An EMS medical director's 3-step plan to protect providers from TB exposure. EMS 1999;24:S6–7.
McLaughlin SI, Spradling P, Drociuk D, Ridzon R, Pozsik CJ, Onorato I. Extensive transmission of Mycobacterium tuberculosis among congregated, HIV-infected prison inmates in South Carolina, United States. Int J Tuberc Lung Dis 2003;7:665–72.
Mohle-Boetani JC, Miguelino V, Dewsnup DH, et al. Tuberculosis outbreak in a housing unit for human immunodeficiency virus–infected patients in a correctional facility: transmission risk factors and effective outbreak control. Clin Infect Dis 2002;34:668–76.
Valway SE, Richards SB, Kovacovich J, Greifinger RB, Crawford JT, Dooley SW. Outbreak of multi-drug-resistant tuberculosis in a New York State prison, 1991. Am J Epidemiol 1994;140:113–22.
Valway SE, Greifinger RB, Papania M, et al. Multidrug-resistant tuberculosis in the New York State prison system, 1990–1991. J Infect Dis 1994;170:151–6.
Cone JE, Harrison R, Katz E, Chan J, Dewsnup D, Osorio AM. tuberculosis transmission to prison employees during an outbreak among prisoners at two California prisons. Journal of Healthcare Safety, Compliance & Infection Control 2004;4:75–9.
Ijaz K, Yang Z, Templeton G, Stead WW, Bates JH, Cave MD. Persistence of a strain of Mycobacterium tuberculosis in a prison system. Int J Tuberc Lung Dis 2004;8:994–1000.
Steenland K, Levine AJ, Sieber K, Schulte P, Aziz D. Incidence of tuberculosis infection among New York State prison employees. Am J Public Health 1997;87:2012–4.
March F, Coll P, Guerrero RA, Busquets E, Cayla JA, Prats G. Predictors of tuberculosis transmission in prisons: an analysis using conventional and molecular methods. AIDS 2000;14:525–35.
Stead WW. Undetected tuberculosis in prison. Source of infection for community at large. JAMA 1978;240:2544–7.
Jones TF, Craig AS, Valway SE, Woodley CL, Schaffner W. Transmission of tuberculosis in a jail. Ann Intern Med 1999;131:557–63.
Hammett TM, Harmon MP, Rhodes W. The burden of infectious disease among inmates of and releasees from US correctional facilities, 1997. Am J Public Health 2002;92:1789–94.
MacIntyre CR, Kendig N, Kummer L, Birago S, Graham NM. Impact of tuberculosis control measures and crowding on the incidence of tuberculous infection in Maryland prisons. Clin Infect Dis 1997;24:1060–7.
Tulsky JP, White MC, Dawson C, Hoynes TM, Goldenson J, Schecter G. Screening for tuberculosis in jail and clinic follow-up after release. Am J Public Health 1998;88:223–6.
Reyes H, Coninx R. Pitfalls of tuberculosis programmes in prisons. BMJ 1997;315:1447–50.
Ismeurt RL, Long CO. Tuberculosis. A new threat from an old nemesis. Home Healthcare Nurse 1993;11:16–23.
Stamp D, Arnold MS. Tuberculosis in home care. Complying with OSHA. Caring 1995;14:16–8, 20–2.
Lefrak S. Tuberculosis screening in a nursing home: indications for preventive therapy. JAMA 1991;266:2000–3.
Thrupp L, Bradley S, Smith P, et al. Tuberculosis prevention and control in long-term–care facilities for older adults. Infect Control Hosp Epidemiol 2004;25:1097–108.
Bentley DW. Tuberculosis in long-term care facilities. Infect Control Hosp Epidemiol 1990;11:42–6.
Malone JL, Ijaz K, Lambert L, et al. Investigation of healthcare-associated transmission of Mycobacterium tuberculosis among patients with malignancies at three hospitals and at a residential facility. Cancer 2004;101:2713–21.
Stead WW. Special problems in tuberculosis. Tuberculosis in the elderly and in residents of nursing homes, correctional facilities, long-term care hospitals, mental hospitals, shelters for the homeless, and jails. Clin Chest Med 1989;10:397–405.
Stead WW. Management of health care workers after inadvertent exposure to tuberculosis: a guide for the use of preventive therapy. Ann Intern Med 1995;122:906–12.
Linder JF, Enders SR, Craig E, Richardson J, Meyers FJ. Hospice care for the incarcerated in the United States: an introduction. J Palliat Med 2002;5:549–52.
McKeogh MM. tuberculosis in the hospice—a cause for concern? Palliative Medicine 1997;11:469–74.
CDC. Mantoux tuberculin skin test—training materials kit. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2003.
Snider DE Jr, Cauthen GM. Tuberculin skin testing of hospital employees: infection, "boosting," and two-step testing. Am J Infect Control 1984;12:305–11.
Duboczy BO, Brown BT. Multiple readings and determination of maximal intensity of tuberculin reaction. Am Rev Respir Dis 1961;84:60–8.
Cobelens F, van Deutekom H, Draayer-Jansen I, Schepp-Beelen A, Van Gerven P, Mensen M. Tuberculin skin test reactions by time of reading among Dutch travellers. Int J Tuberc Lung Dis 2003;7:758–63.
Huebner RE, Schein MF, Bass JB Jr. The tuberculin skin test. Clin Infect Dis 1993;17:968–75.
Karalliedde S, Katugaha LP, Uragoda CG. Tuberculin response of Sri Lankan children after BCG vaccination at birth. Tubercle 1987;68:33–8.
Mazurek GH, LoBue PA, Daley CL, et al. Comparison of a whole-blood interferon gamma assay with tuberculin skin testing for detecting latent Mycobacterium tuberculosis infection. JAMA 2001;286:1740–7.
Menzies R, Vissandjee B. Effect of Bacille Calmette-Guerin vaccination on tuberculin reactivity. Am Rev Respir Dis 1992;145:621–5.
Snider DE Jr. Bacille Calmette-Guerin vaccinations and tuberculin skin tests. JAMA 1985;253:3438–9.
Bugiani M, Borraccino A, Migliore E, et al. Tuberculin reactivity in adult BCG-vaccinated subjects: a cross-sectional study. Int J Tuberc Lung Dis 2003;7:320–6.
Aronson NE, Santosham M, Comstock GW, et al. Long-term efficacy of BCG vaccine in American Indians and Alaska Natives. A 60-year follow-up study. JAMA 2004;291:2086–91.
Dye C. A booster for tuberculosis vaccines. JAMA 2004;291:2127–8.
Fine PE, Carneiro IAM, Milstien JB, Clements CJ. Issues relating to the use of BCG in immunization programs. A discussion document. Geneva, Switzerland: World Health Organization, Department of Vaccines and Biologicals; 1999.
Senate and House of Representatives of the United States of America. Americans with Disabilities Act of 1990, Titles I and V; 1990:12101–213.
Widdowson MA, Bosman A, van Straten E, et al. Automated, laboratory-based system using the internet for disease outbreak detection, the Netherlands. Emerg Infect Dis 2003;9:1046–52.
Malakmadze N, Gonzalez IM, Oemig T, et al. Unsuspected recent transmission of tuberculosis among high-risk groups: implications of universal tuberculosis genotyping in its detection. Clin Infect Dis 2005;40:366–73.
Nardell E, McInnis B, Thomas B, Weidhaas S. Exogenous reinfection with tuberculosis in a shelter for the homeless. N Engl J Med 1986;315:1570–5.
Occupational Safety and Health Administration. Recording and reporting occupational injuries and illnesses Title 29, Code of Federal Regulations 2003. Part 1904.
Sacks LV, Pendle S, Orlovic D, Blumberg L, Constantinou C. A comparison of outbreak- and nonoutbreak-related multidrug-resistant tuberculosis among human immunodeficiency virus–infected patients in a South African hospital. Clin Infect Dis 1999;29:96–101.
Aznar J, Safi H, Romero J, Alejo A, Gracia A, Palomares JC. Nosocomial transmission of tuberculosis infection in pediatrics wards. Pediatr Infect Dis J 1995;14:44–8.
Bauer J, Kok-Jensen A, Faurschou P, Thuesen J, Taudorf E, Andersen AB. A prospective evaluation of the clinical value of nation-wide DNA fingerprinting of tuberculosis isolates in Denmark. Int J Tuberc Lung Dis 2000;4:295–9.
Blazquez J, Espinosa de Los Monteros LE, Samper S, et al. Genetic characterization of multidrug-resistant Mycobacterium bovis strains from a hospital outbreak involving human immunodeficiency virus-positive patients. J Clin Microbiol 1997;35:1390–3. Erratum in: J Clin Microbiol 1998;36:2398.
Brown TJ, Tansel O, French GL. Simultaneous identification and typing of multi-drug-resistant Mycobacterium tuberculosis isolates by analysis of pncA and rpoB. J Med Microbiol 2000;49:651–6.
Cohn DL, O'Brien RJ. The use of restriction fragment length polymorphism (RFLP) analysis for epidemiological studies of tuberculosis in developing countries. Int J Tuberc Lung Dis 1998;2:16–26.
French AL, Welbel SF, Dietrich SE, et al. Use of DNA fingerprinting to assess tuberculosis infection control. Ann Intern Med 1998;129:856–61.
Garzelli C, Lari N, Nguon B, Falcone G. Evidence of nosocomial transmission of tuberculosis among AIDS patients by DNA fingerprinting. New Microbiol 1996;19:285–91.
Haas DW, Milton S, Kreiswirth BN, Brinsko VL, Bifani PJ, Schaffner W. Nosocomial transmission of a drug-sensitive W-variant Mycobacterium tuberculosis strain among patients with acquired immunodeficiency syndrome in Tennessee. Infect Control Hosp Epidemiol 1998;19:635–9.
Lambregts-van Weezenbeek CS, Keizer ST, Sebek MM, Schepp-Beelen JC, van der Loo CJ. Transmission of multiresistant tuberculosis in a Dutch hospital [Dutch]. Ned Tijdschr Geneeskd 1996;140:2293–5.
Lemaitre N, Sougakoff W, Truffot-Pernot C, et al. Use of DNA fingerprinting for primary surveillance of nosocomial tuberculosis in a large urban hospital: detection of outbreaks in homeless persons and migrant workers. Int J Tuberc Lung Dis 1998;2:390–6.
Moro ML, Gori A, Errante I, et al. An outbreak of multidrug-resistant tuberculosis involving HIV-infected patients of two hospitals in Milan, Italy. AIDS 1998;12:1095–102.
Moss AR, Alland D, Telzak E, et al. A city-wide outbreak of a multiple-drug-resistant strain of Mycobacterium tuberculosis in New York. Int J Tuberc Lung Dis 1997;1:115–21.
Narvskaya O, Otten T, Limeschenko E, et al. Nosocomial outbreak of multidrug-resistant tuberculosis caused by a strain of Mycobacterium tuberculosis W-Beijing family in St. Petersburg, Russia. Eur J Clin Microbiol Infect Dis 2002;21:596–602.
Samper S, Martin C, Pinedo A, et al. Transmission between HIV-infected patients of multidrug-resistant tuberculosis caused by Mycobacterium bovis. AIDS 1997;11:1237–42.
van Soolingen D, Hermans PW. Epidemiology of tuberculosis by DNA fingerprinting. Eur Respir J 1995;20(Suppl):649S–56S.
Behr MA, Warren SA, Salamon H, et al. Transmission of Mycobacterium tuberculosis from patients smear-negative for acid-fast bacilli. Lancet 1999;353:444–9. Erratum in: Lancet 1999;353:1714.
Reichler MR, Etkind S, Taylor Z, Castro KG. Tuberculosis contact investigations. Int J Tuberc Lung Dis 2003;7:S325–S327.
Reichler MR, Reves R, Bur S, et al. Evaluation of investigations conducted to detect and prevent transmission of tuberculosis. JAMA 2002;287:991–5.
Reichler M, Taylor Z, Castro KG. Factors in tuberculosis contact investigations. JAMA 2002;287:2944–5.
Occupational Safety and Health Administration. Occupational exposure to tuberculosis: proposed rule. Federal Register 1997;62:54159–309.
Occupational Safety and Health Administration. Occupational exposure to tuberculosis: proposed rule: termination of rulemaking respiratory protection for M. tuberculosis: final rule (revocation). Federal Register 2003;68:75767–75.
Occupational Safety and Health Administration. Directive number: CPL 2.106. Enforcement procedures and scheduling for occupational exposure to tuberculosis; 1996:1–131.
Occupational Safety and Health Administration. Occupational safety and health standards, subpart I—personal protective equipment. Respiratory protection for M. tuberculosis. Title 29, Code of Federal Regulations 2003. Section 1910.139.
Occupational Safety and Health Administration. Occupational safety and health standards, subpart I—personal protective equipment. Respiratory protection. Title 29, Code of Federal Regulations 2003. Section 1910.134.
CDC. Protect yourself against tuberculosis: a respiratory protection guide for health care workers. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1996. DHHS (NIOSH) publication no. 96–102.
CDC. Guide to the selection and use of particulate respirators certified under 42 CFR 84. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1996. DHHS (NIOSH) publication no. 96-101.
CDC. TB respiratory protection program in health care facilities: administrator's guide. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1999. DHHS (NIOSH) publication no. 99-143.
Ryan MG. Developing a respiratory protection program, Understanding the written elements. AAOHN J 2001;49:293–307.
CDC. Guide to industrial respiratory protection. Morgantown, WV: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1987. DHHS (NIOSH) publication no. 87-116.
American National Standards Institute. American national standard practices for respiratory protection. ANSI Standard Number 288.2–1992. New York, NY: American National Standards Institute; 1992.
European Committee for Standardization. Respiratory protective devices: filtering half masks to protect against particles—Requirements, testing, marking. Europaishe Norm 2001;149.
Food and Drug Administration. Surgical masks—premarket notification [510(k)] submissions. Guidance for Industry and FDA. Rockville, MD: US Department of Health and Human Services, Food and Drug Administration; 2003.
Campbell DL, Coffey CC, Lenhart SW. Respiratory protection as a function of respirator fitting characteristics and fit-test accuracy. AIHA Journal 2001;62:36–44.
Coffey CC, Lawrence RB, Zhuang Z, Campbell DL, Jensen PA, Myers WR. Comparison of five methods for fit-testing N95 filtering-facepiece respirators. Appl Occup Environ Hyg 2002;17:723–30.
Coffey CC, Lawrence RB, Campbell DL, Zhuang Z, Calvert CA, Jensen PA. Fitting characteristics of eighteen N95 filtering-facepiece respirators. J Occup Environ Health 2004;1:262–71.
Hyatt EC, Pritchard JA, Haek AL. Respiratory studies for the National Institute for Occupational Safety and Health. Los Alamos, NM: Los Alamos Scientific Laboratory; 1974.
Lawrence RB, Campbell DL, Myers WR, Calvert CA, Jensen PA, Coffey CC. Determining the efficacy of fit-test protocols using N95 filtering-facepiece respirators—alternate approaches. J Inter Soc Respir Protect 2003;20:45–56.
Lee K, Slavcev A, Nicas M. Respiratory protection against Mycobacterium tuberculosis: quantitative fit test outcomes for five type N95 filtering-facepiece respirators. J Occup Environ Health 2004;1:22–8.
Martyny J, Glazer CS, Newman LS. Current concepts. Respiratory protection. N Engl J Med 2002;347:824–30.
Lowry PL, Hesch PR, Revoir WH. Performance of single-use respirators. Am Industrial Hyg Assoc J 1977;38:462–7.
Nicas M, Neuhaus J. Variability in respiratory protection and the assigned protection factor. J Occup Environ Health 2004;1:99–109.
Lenhart SW, Seitz T, Trout D, Bollinger N. Issues affecting respirator selection for workers exposed to infectious aerosols: emphasis on healthcare settings. Applied Biosafety 2004;9:20–36.
McWilliams T, Wells AU, Harrison AC, Lindstrom S, Cameron RJ, Foskin E. Induced sputum and bronchoscopy in the diagnosis of pulmonary tuberculosis. Thorax 2002;57:1010–4.
Riley RL, Mills CC, O'Grady F, Sultan LU, Wittstadt F, Shivpuri DN. Infectiousness of air from a tuberculosis ward: ultraviolet irradiation of infected air: comparative infectiousness of different patients. Am Rev Respir Dis 1962;85:511–25.
Noble RC. Infectiousness of pulmonary tuberculosis after starting chemotherapy: review of the available data on an unresolved question. Am J Infect Control 1981;9:6–10.
Coronado VG, Beck-Sague CM, Hutton MD, et al. Transmission of multidrug-resistant Mycobacterium tuberculosis among persons with human immunodeficiency virus infection in an urban hospital: epidemiologic and restriction fragment length polymorphism analysis. J Infect Dis 1993;168:1052–5.
Long R, Zielinski M, Kunimoto D, Manfreda J. The emergency department is a determinant point of contact of tuberculosis patients prior to diagno sis. Int J Tuberc Lung Dis 2002;6:332–9.
Luby S, Carmichael S, Shaw G, Horan J, Gamble W Jr, Jones J. A nosocomial outbreak of Mycobacterium tuberculosis. J Fam Pract 1994;39:21–5.
Nivin B, Nicholas P, Gayer M, Frieden TR, Fujiwara PI. A continuing outbreak of multidrug-resistant tuberculosis, with transmission in a hospital nursery. Clin Infect Dis 1998;26:303–7.
Mastorides SM, Oehler RL, Greene JN, Sinnott JT, Kranik M, Sandin RL. The detection of airborne Mycobacterium tuberculosis using micropore membrane air sampling and polymerase chain reaction. Chest 1999;115:19–25.
Sultan L, Nyka W, Mills C, O'Grady F, Wells W, Riley RL. Tuberculosis disseminators. A study of the variability of aerial infectivity of tuberculosis patients. Am Rev Respir Dis 1960;82:358–69.
Fennelly KP, Martyny JW, Fulton KE, Orme IM, Cave DM, Heifets LB. Cough-generated aerosols of Mycobacterium tuberculosis. A new method to study infectiousness. Am J Respir Crit Care Med 2004;169:604–9.
Ijaz K, Castro KG. Pediatric tuberculosis: all in the family? Infect Control Hosp Epidemiol 2002;23:562–3.
Munoz FM, Ong LT, Seavy D, Medina D, Correa A, Starke JR. Tuberculosis among adult visitors of children with suspected tuberculosis and employees at a children's hospital. Infect Control Hosp Epidemiol 2002;23:568–72.
Wallgren A. On contagiousness of childhood tuberculosis. Acta Pediatr Scand 1937;22:229–34.
Garcia-Garcia ML, Valdespino-Gomez JL, Garcia-Sancho C, et al. Underestimation of Mycobacterium tuberculosis infection in HIV-infected subjects using reactivity to tuberculin and anergy panel. Int J Epidemiol 2000;29:369–75.
Ridzon R, Kenyon T, Luskin-Hawk R, Schultz C, Valway S, Onorato IM. Nosocomial transmission of human immunodeficiency virus and subsequent transmission of multidrug-resistant tuberculosis in a healthcare worker. Infect Control Hosp Epidemiol 1997;18:422–3.
Snider DE Jr, Kelly GD, Cauthen GM, Thompson NJ, Kilburn JO. Infection and disease among contacts of tuberculosis cases with drug-resistant and drug-susceptible bacilli. Am Rev Respir Dis 1985;132:125–32.
Schaaf HS, Shean K, Donald PR. Culture confirmed multidrug resistant tuberculosis: diagnostic delay, clinical features, and outcome. Arch Dis Child 2003;88:1106–11.
Cauthen GM, Dooley SW, Onorato IM, et al. Transmission of Mycobacterium tuberculosis from tuberculosis patients with HIV infection or AIDS. Am J Epidemiol 1996;144:69–77.
Espinal MA, Perez EN, Baez J, et al. Infectiousness of Mycobacterium tuberculosis in HIV-1-infected patients with tuberculosis: a prospective study. Lancet 2000;355:275–80.
Klausner JD, Ryder RW, Baende E, et al. Mycobacterium tuberculosis in household contacts of human immunodeficiency virus type 1–eropositive patients with active pulmonary tuberculosis in Kinshasa, Zaire. J Infect Dis 1993;168:106–11. Erratum in: J Infect Dis 1993;168:802.
Nunn P, Mungai M, Nyamwaya J. The effect of human immunodeficiency virus type-1 on the infectiousness of tuberculosis. Tubercle Lung Dis 1994;75:25–32.
Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk for tuberculosis among intravenous drug users with human immunodeficiency virus infection. N Engl J Med 1989;320:545–50.
Rose DN, Schechter CB, Adler JJ. Interpretation of the tuberculin skin test. J Gen Intern Med 1995;10:635–42.
Menzies D. Interpretation of repeated tuberculin tests. Boosting, conversion, and reversion. Am J Respir Crit Care Med 1999;159:15–21.
CDC. Mantoux tuberculin skin test [Poster]. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2004.
Joseph HA, Shrestha-Kuwahara R, Lowry D, et al. Factors influencing healthcare workers' adherence to work site tuberculosis screening and treatment policies. Am J Infect Control 2004;32:456–61.
Mantoux C, Roux E. Report of intradermal reaction of tuberculin [French]. The Academy of Sciences 1908;147:355–7.
Mendel F. The intravenous application of medicine. Therapeutic Monthly 1902;17:177–93.
Mendel F. von Pirquet's skin reaction and intravenous tuberculosis treatment. Medical Clinical Hospital 1908;4:402–4
National Tuberculosis Controllers Association, National Tuberculosis Nurse Consultant Coalition. Tuberculosis nursing: a comprehensive guide to patient care. Smyrna, GA: National Tuberculosis Controllers Association; 1997.
CDC. National Health and Nutrition Examination Survey (NHANES). Tuberculosis skin test procedures manual. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2000.
Occupational Safety and Health Administration. Occupational safety and health standards, subpart Z—toxic and hazardous substances. Bloodborne pathogens Title 29, Code of Federal Regulations 2003. Section 1910.1030.
Sokal JE. Measurement of delayed skin-test responses [Editorial]. N Engl J Med 1975;293:501–2.
Lee E, Holzman RS. Evolution and current use of the tuberculin test. Clin Infect Dis 2002;34:365–70.
Snider DE Jr. The tuberculin skin test. Am Rev Respir Dis 1982;125:108–18.
Marsh BJ, San Vicente J, von Reyn F. Utility of dual skin tests to evaluate tuberculin skin test reactions of 10 to 14 mm in healthcare workers. Infect Control Hosp Epidemiol 2003;24:821–4.
Winthrop KL, Siegel JN, Jereb J, Taylor Z, Iademarco MF. Tuberculosis associated with therapy against tumor necrosis factor alpha. Arthritis Rheum 2005;52:2968–74.
Potter PA, Perry AG. Fundamentals of nursing. 5th ed. St. Louis, MO: Mosby, Inc.; 2001.
Canessa PA, Fasano L, Lavecchia MA, Torraca A, Schiattone ML. Tuberculin skin test in asymptomatic HIV seropositive carriers. Chest 1989;96:1215–6.
Huebner RE, Schein MF, Hall CA, Barnes SA. Delayed-type hypersensitivity anergy in human immunodeficiency virus–infected persons screened for infection with Mycobacterium tuberculosis. Clin Infect Dis 1994;19:26–32.
Slovis BS, Plitman JD, Haas DW. The case against anergy testing as a routine adjunct to tuberculin skin testing. JAMA 2000;283:2003–7.
Narita M, Ashkin D, Hollender ES, Pitchenik AE. Paradoxical worsening of tuberculosis following antiretroviral therapy in patients with AIDS. Am J Respir Crit Care Med 1998;158:157–61.
Snider DE. Pregnancy and tuberculosis. Chest 1984;86:10S–13S.
Addis A, Blowey D, Koren G. Tuberculosis during pregnancy. Can Fam Physician 1996;42:1461–2.
American College of Obstetricians and Gynecologists. ACOG technical bulletin. Pulmonary disease in pregnancy. Number 224–June 1996. Int J Gynecol Obstet 1996;54:187–96.
Cauthen GM, Snider DE Jr, Onorato IM. Boosting of tuberculin sensitivity among Southeast Asian refugees. Am J Respir Crit Care Med 1994;149:1597–600.
Menzies D. What does tuberculin reactivity after Bacille Calmette-Guerin vaccination tell us? Clin Infect Dis 2000;31(Suppl 3):S71–4.
Moreno S, Blazquez R, Novoa A, et al. The effect of BCG vaccination on tuberculin reactivity and the booster effect among hospital employees. Arch Intern Med 2001;161:1760–5.
Villarino ME, Burman W, Wang YC, et al. Comparable specificity of 2 commercial tuberculin reagents in persons at low risk for tuberculous infection. JAMA 1999;281:169–71.
Blumberg HM, White N, Parrott P, Gordon W, Hunter M, Ray S. False-positive tuberculin skin test results among health care workers. JAMA 2000;283:2793.
Greenberg SD, Frager D, Suster B, Walker S, Stavropoulos C, Rothpearl A. Active pulmonary tuberculosis in patients with AIDS: spectrum of radiographic findings (including a normal appearance). Radiology 1994;193:115–9.
Havlir DV, Barnes PF. Tuberculosis in patients with human immunodeficiency virus infection. N Engl J Med 1999;340:367–73.
Jones BE, Ryu R, Yang Z, et al. Chest radiographic findings in patients with tuberculosis with recent or remote infection. Am J Respir Crit Care Med 1997;155:1270–3.
Tattevin P, Casalino E, Fleury L, Egmann G, Ruel M, Bouvet E. The validity of medical history, classic symptoms, and chest radiographs in predicting pulmonary tuberculosis: derivation of a pulmonary tuberculosis prediction model. Chest 1999;115:1248–53.
Chintu C, Mwaba P. Is there a role for chest radiography in identification of asymptomatic tuberculosis in HIV-infected persons? Lancet 2003;362:1516.
Mosimaneotsile B, Talbot EA, Moeti TL, et al. Value of chest radiography in a tuberculosis prevention programme for HIV-infected people, Botswana. Lancet 2003;362:1551–2.
Siddiqui AH, Perl TM, Conlon M, Donegan N, Roghmann MC. Preventing nosocomial transmission of pulmonary tuberculosis: when may isolation be discontinued for patients with suspected tuberculosis? Infect Control Hosp Epidemiol 2002;23:141–4.
Shata AM, Coulter JB, Parry CM, Ching'ani G, Broadhead RL, Hart CA. Sputum induction for the diagnosis of tuberculosis. Arch Dis Child 1996;74:535–7.
Anderson C, Inhaber N, Menzies D. Comparison of sputum induction with fiber-optic bronchoscopy in the diagnosis of tuberculosis. Am J Respir Crit Care Med 1995;152:1570–4.
Burnens AP, Vurma-Rapp U. Mixed mycobacterial cultures—occurrence in the clinical laboratory. Int J Med Microbiol 1989;271:85–90.
Malasky C, Jordan T, Potulski F, Reichman LB. Occupational tuberculous infections among pulmonary physicians in training. Am Rev Respir Dis 1990;142:505–7.
Carr DT, Karlson AG, Stilwell GG. A comparison of cultures of induced sputum and gastric washings in the diagnosis of tuberculosis. Mayo Clin Proc 1967;42:23–5.
Hensler NM, Spivey Jr CG, Dees TM. The use of hypertonic aerosol in production of sputum for diagnosis of tuberculosis. Comparison with gastric specimens. Dis Chest 1961;40:639–42.
Makkar H, Mallampalli A, Matthew M, et al. Improved yield of Mycobacterium tuberculosis with sputum induction in addition to three expectorated sputa. Am J Respir Crit Care Med 2000;161:A298.
Yajko DM, Nassos PS, Sanders CA, Madej JJ, Hadley WK. High predictive value of the acid-fast smear for Mycobacterium tuberculosis despite the high prevalence of Mycobacterium avium complex in respiratory specimens. Clin Infect Dis 1994;19:334–6.
Khilnani GC. Tuberculosis and pregnancy. Indian J Chest Dis Allied Sci 2004;46:105–11.
Edwards LB, Palmer CE, Magnus K, eds. Response to BCG vaccination [Chapter 3]. In: BCG Vaccination Studies by the WHO Tuberculosis Research Office, Copenhagen. Geneva, Switzerland: World Health Organization; 1953:51–64.
Menzies RI. Tuberculin skin testing. In: Reichman LB, Hershfield ES, eds. Tuberculosis. A comprehensive international approach. 2nd ed. New York, NY: Marcel Dekker, Inc.; 2000:279–322.
Caminero JA, Pena MJ, Campos-Herrero MI, et al. Exogenous reinfection with tuberculosis on a European island with a moderate incidence of disease. Am J Respir Crit Care Med 2001;163:717–20.
de Viedma DG, Marin M, Hernangomez S, et al. Tuberculosis recurrences: reinfection plays a role in a population whose clinical/epidemiological characteristics do not favor reinfection. Arch Intern Med 2002;162:1873–9.
Small PM, Shafer RW, Hopewell PC, et al. Exogenous reinfection with multidrug-resistant Mycobacterium tuberculosis in patients with advanced HIV infection. N Engl J Med 1993;328:1137–44.
van Rie A, Warren R, Richardson M, et al. Exogenous reinfection as a cause of recurrent tuberculosis after curative treatment. N Engl J Med 1999;341:1174–9.
Iseman MD, Madsen LA. Drug-resistant tuberculosis. Clin Chest Med 1989;10:341–53.
Iseman MD. Drug therapy: treatment of multidrug-resistant tuberculosis. N Engl J Med 1993;329:784–91. Erratum in: N Engl J Med 1993;329:1435.
Goble M. Drug-resistant tuberculosis. Semin Respir Infect 1986;1:220–9.
Goble M, Iseman MD, Madsen LA, Waite D, Ackerson L, Horsburgh CR Jr. Treatment of 171 patients with pulmonary tuberculosis resistant to isoniazid and rifampin. N Engl J Med 1993;328:527–32.
Simone PM, Iseman MD. Drug-resistant tuberculosis: a deadly — and growing — danger. J Respir Dis 1992;13:960–71.
Riley RL, Knight M, Middlebrook G. Ultraviolet susceptibility of BCG and virulent tubercle bacilli. Am Rev Respir Dis 1976;113:413–8.
Riley RL, Nardell EA. Clearing the air. The theory and application of ultraviolet air disinfection. Am Rev Respir Dis 1989;139:1286–94.
American National Standards Institute, American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. ANSI/ASHRAE Standard 62.1-2004: ventilation for acceptable indoor air quality. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.; 2004.
Hayden II CS, Fischbach TJ, Johnston OE, Hughes RT, Jensen PA. A model for calculating leakage areas into negative pressure isolation rooms. Cincinnati, OH: US Department of Health and Human Services, CDC; 1996.
Rice N, Streifel A, Vesley D. An evaluation of hospital special-ventilation-room pressures. Infect Control Hosp Epidemiol 2001;22:19–23.
Streifel AJ, Marshall JW. Parameters for ventilation controlled environments in hospitals. In: Moschandreas DJ, ed. Design, construction, and operation of healthy buildings: solutions to global and regional concerns. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers Press; 1998:305–9.
DeLuga GF. Designing laboratory ventilation. In: Richmond JY, ed. Designing a modern microbiological/biomedical laboratory. Lab design process & technology. Washington, DC: American Public Health Association; 1997:234.
Jensen PA, Hayden II CS, Burroughs E, Hughes RT. Assessment of the health hazard associated with the use of smoke tubes in healthcare facilities. Appl Occup Environ Hyg 1998;13:172–6.
Pavelchak N, DePersis RP, London M, et al. Identification of factors that disrupt negative air pressurization of respiratory isolation rooms. Infect Control Hosp Epidemiol 2000;21:191–5.
Hayden II CS. Positive advice on negative pressure for TB isolation rooms. Health Facil Manage 1997;10:43–5.
Hayden II CS, Johnston OE, Hughes RT, Jensen PA. Air volume migration from negative pressure isolation rooms during entry/exit. Appl Occup Environ Hyg 1998;13:518–27.
American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. Airflow around buildings [Chapter 16]. 2005 ASHRAE handbook: 2005 fundamentals. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.; 2005:16.1–16.12.
CDC. Health hazard evaluations: tuberculosis 1990–1999. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 2001. DHHS (NIOSH) publication no. 2001-116.
Esterhai JL Jr, Reynolds MR, Chou L. Hazards to the orthopaedic trauma surgeon: occupational exposure to tuberculosis. Risk reduction, testing, and treatment (a review article). J Orthop Trauma 1996;10:366–70.
Seitz T, Decker J. Health hazard evaluation report. Onondaga County Medical Examiner's Office, Syracuse, New York. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1992; report no. HETA 92-171-2255.
Opal SM, Asp AA, Cannady PB Jr, Morse PL, Burton LJ, Hammer II PG. Efficacy of infection control measures during a nosocomial outbreak of disseminated aspergillosis associated with hospital construction. J Infect Dis 1986;153:634–7.
Rhame FS, Streifel AJ, Kersey JH Jr, McGlave PB. Extrinsic risk factors for pneumonia in the patient at high risk of infection. Am J Med 1984;76:42–52.
Sherertz RJ, Belani A, Kramer BS, et al. Impact of air filtration on nosocomial aspergillus infections. Unique risk for bone marrow transplant recipients. Am J Med 1987;83:709–18.
Rippon JW, Gerhold R, Heath M. Thermophillic and thermotolerant fungi isolated from the thermal effluent of nuclear power generating reactors: dispersal of human opportunistic and veterinary pathogenic fungi. Mycopathologia 1980;70:169–79.
Brown RC. Air filtration. An integrated approach to the theory and applications of fibrous filters. 1st ed. Tarrytown, NY: Pergamon Press; 1993.
Woods JE. Cost avoidance and productivity in owning and operating buildings. 4th ed. Philadelphia, PA: Hanley & Belfus, Inc.; 1989:753–70.
Cheng YS, Lu JC, Chen TR. Efficiency of a portable indoor air cleaner in removing pollens and fungal spores. Aerosol Science and Technology 1998;29:92–101.
ECRI. TB engineering controls: mobile high-efficiency-filter air cleaners. Health Devices 1995;24:370–418.
Marier RL, Nelson T. A ventilation-filtration unit for respiratory isolation. Infect Control Hosp Epidemiol 1993;14:700–5.
Miller-Leiden S, Lobascio C, Nazaroff WW, Macher JM. Effectiveness of in-room air filtration and dilution ventilation for tuberculosis infection control. J Air Waste Manag Assoc 1996;46:869–82.
Miller SL, Hernandez M. Evaluating portable air cleaner removal efficiencies for bioaerosols. Boulder, CO: University of Colorado at Boulder; 2002; NIOSH contract report PO-36755-R-00077B5D.
Rutala WA, Jones SM, Worthington JM, Reist PC, Weber DJ. Efficacy of portable filtration units in reducing aerosolized particles in the size range of Mycobacterium tuberculosis. Infect Control Hosp Epidemiol 1995;16:391–8.
Woods JE, Rask DR. Heating, ventilation, air-conditioning systems: the engineering approach to methods of control. In: Kundsin RB, ed. Architectural design and indoor microbial pollution. New York, NY: Oxford University Press; 1988:123–53.
American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. Air cleaners for particulate contaminants. 2004 ASHRAE handbook: HVAC systems and equipment. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.; 2004:24.1–24.13.
National Sanitation Foundation (NSF). Class II (laminar flow) biohazard cabinetry—NSF/ANSI standard 49-2002. Ann Arbor, MI: National Sanitation Foundation International; 2001.
Ko G, Burge HA, Muilenberg M, Rudnick S, First M. Survival of mycobacteria on HEPA filter material. J Amer Biologic Safety Assoc 1998;3:65–78.
Qian Y, Willeke K, Grinshpun SA, Donnelly J. Performance of N95 respirators: reaerosolization of bacteria and solid particles. AIHA Journal 1997;58:876–80.
Reponen TA, Wang Z, Willeke K, Grinshpun SA. Survival of mycobacteria on N95 personal respirators. Infect Control Hosp Epidemiol 1999;20:237–41.
Rutala WA, Cole EC, Wannamaker NS, Weber DJ. Inactivation of Mycobacterium tuberculosis and Mycobacterium bovis by 14 hospital disinfectants. Am J Med 1991;91(Suppl 3B):267S–71S.
Illuminating Engineering Society of North America. The IESNA lighting handbook—reference and application. 9th ed. New York, NY: Illuminating Engineering Society of North America; 2000.
Riley RL, Wells WF, Mills CC, Nyka W, McLean RL. Air hygiene in tuberculosis: quantitative studies of infectivity and control in a pilot ward. Am Rev Tuberc 1957;75:420–31.
Riley RL. Ultraviolet air disinfection for control of respiratory contagion. In: Kundsin RB, ed. Architectural design and indoor microbial pollution. New York, NY: Oxford University Press; 1988:174–97.
Stead WW. Clearing the air: the theory and application of ultraviolet air disinfection. Am Rev Respir Dis 1989;140:1832.
Xu P. Ultraviolet germicidal irradiation for preventing infectious disease transmission. Boulder, CO: University of Colorado, Department of Civil, Environmental, and Architectural Engineering; 2001.
Xu P, Peccia J, Fabian P, et al. Efficacy of ultraviolet germicidal irradiation of upper-room air in inactivating airborne bacterial spores and mycobacteria in full-scale studies. Atmospheric Environment 2003;37:405–19.
McLean RL. Mechanisms of spread. The mechanism of spread of Asian influenza. Am Rev Respir Dis 1961;83:29–40.
Willmon TL, Hollaender A, Langmuir AD. Studies of the control of acute respiratory diseases among naval recruits. I. A review of a four-year experience with ultraviolet irradiation and dust suppressive measures, 1943 to 1947. Am J Hyg 1948;48:227–32.
Perkins JE, Bahlke AM, Silverman HF. Effect of ultra-violet irradiation of classrooms on spread of measles in large rural central schools. Am J Public Health 1947;37:529–37.
Wells WF, Wells MW, Wilder TS. The environmental control of epidemic contagion: I. An epidemiologic study of radiant disinfection of air in day schools. Am J Hyg 1942;35:97–121.
Wells WF, Holla WA. Ventilation in the flow of measles and chickenpox through a community. Progress report, January 1, 1946 to June 15, 1949, Airborne Infection Study, Westchester County Department of Health. JAMA 1950;142:1337–44.
Collins FM. Relative susceptibility of acid-fast and non-acid-fast bacteria to ultraviolet light. Appl Microbiol 1971;21:411–3.
David HL, Jones WD Jr, Newman CM. Ultraviolet light inactivation and photoreactivation in the mycobacteria. Infect Immun 1971;4:318–9.
David HL. Response of mycobacteria to ultraviolet light radiation. Am Rev Respir Dis 1973;108:1175–85.
Lurie MB. Resistance to tuberculosis: experimental studies in native and acquired defensive mechanisms. Cambridge, MA: Harvard University Press; 1964.
National Tuberculosis and Respiratory Disease Association. Guidelines for the general hospital in the admission and care of tuberculous patients. Am Rev Respir Dis 1969;99:631–3.
Schieffelbein CW Jr, Snider DE Jr. Tuberculosis control among homeless populations. Arch Intern Med 1988;148:1843–6.
First MW, Nardell EA, Chaisson RE, Riley R. Guidelines for the application of upper-room ultraviolet germicidal irradiation for preventing transmission of airborne contagion—part 1: basic principles. ASHRAE Transactions: Symposia 1999;105:869–76.
First MW, Nardell EA, Chaisson RE, Riley R. Guidelines for the application of upper-room ultraviolet germicidal irradiation for preventing transmission of airborne contagion—part 2: design and operation guidance. ASHRAE Transactions: Symposia 1999;105:877–87.
Miller SL, Macher JM. Evaluation of a methodology for quantifying the effect of room air ultraviolet germicidal irradiation on airborne bacteria. Aerosol Science and Technology 2000;33:274–95.
Kowalski WJ, Bahnfleth WP. UVGI design basics for air and surface disinfection. Ultraviolet germicidal irradiation lamps can help clean coils and improve indoor air quality. HPAC 2000;100–10.
Green CF, Scarpino PV. The use of ultraviolet germicidal irradiation (UVGI) in disinfection of airborne bacteria. Environ Eng Policy 2002;3:101–7.
Riley RL, Permutt S, Kaufman JE. Convection, air mixing, and ultraviolet air disinfection in rooms. Arch Environ Health 1971;22:200–7.
Riley RL, Permutt S, Kaufman JE. Room air disinfection by ultraviolet irradiation of upper air. Further analysis of convective air exchange. Arch Environ Health 1971;23:35–9.
Riley RL, Permutt S. Room air disinfection by ultraviolet irradiation of upper air. Air mixing and germicidal effectiveness. Arch Environ Health 1971;22:208–19.
Riley RL, Kaufman JE. Air disinfection in corridors by upper air irradiation with ultraviolet. Arch Environ Health 1971;22:551–3.
Ko G, First MW, Burge HA. The characterization of upper-room ultraviolet germicidal irradiation in inactivating airborne microorganisms. Environmental Health Perspectives 2002;110:95–101.
Xu P, Peccia J, Hernandez M, Miller SL. The efficacy of upper room ultraviolet germicidal irradiation in inactivating airborne microorganisms under incomplete mixing conditions. Proceedings of Engineering Solutions to Indoor Air Quality Problems, Raleigh, NC; July 17–19, 2000.
Memarzadeh F, Jiang J. Methodology for minimizing risk from airborne organisms in hospital isolation rooms. ASHRAE Transactions: Symposia 2000;733–49.
Ko G, First MW, Burge HA. Influence of relative humidity on particle size and UV sensitivity of Serratia marcescens and Mycobacterium bovis BCG aerosols. Tubercle Lung Dis 2000;80:217–28.
Peccia J, Werth HM, Miller S, Hernandez M. Effects of relative humidity on the ultraviolet induced inactivation of airborne bacteria. Aerosol Science and Technology 2001;35:728–40.
Riley RL, O'Grady F. Airborne infection: transmission and control. New York, NY: MacMillan; 1961.
Riley RL, Kaufman JE. Effect of relative humidity on the inactivation of airborne Serratia marcescens by ultraviolet radiation. Appl Microbiol 1972;23:1113–20.
American National Standards Institute, American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc. Standard 55–2004. Thermal environmental conditions for human occupancy. Atlanta, GA: American Society of Heating, Refrigerating and Air-Conditioning Engineers, Inc.; 2004.
Kethley TW, Branch K. Ultraviolet lamps for room air disinfection. Effect of sampling location and particle size of bacterial aerosol. Arc Environ Health 1972;25:205–14.
National Institute for Occupational Safety and Health. Criteria for a recommended standard. Occupational exposure to ultraviolet radiation. Atlanta, GA: US Department of Health, Education, and Welfare, Public Health Service, Health Services and Mental Health Administration; 1972.
International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans: solar and ultraviolet radiation. Lyon, France: World Health Organization; 1992.
Clerici M, Shearer GM. UV light exposure and HIV replication. Science 1992;258:1070–1.
Stein B, Rahmsdorf HJ, Steffen A, Litfin M, Herrlich P. UV-induced DNA damage is an intermediate step in UV-induced expression of human immunodeficiency virus type 1, collagenase, c-fos, and metallothionein. Mol Cell Biol 1989;9:5169–81.
Valerie K, Delers A, Bruck C, et al. Activation of human immunodeficiency virus type 1 by DNA damage in human cells. Nature 1988;333:78–81.
Valerie K, Rosenberg M. Chromatin structure implicated in activation of HIV-1 gene expression by ultraviolet light. New Biol 1990;2:712–8.
Wallace BM, Lasker JS. Awakenings... UV light and HIV gene activation. Science 1992;257:1211–2.
Zmudzka BZ, Beer JZ. Activation of human immunodeficiency virus by ultraviolet radiation. Photochem Photobiol 1990;52:1153–62.
Everett MA, Sayre RM, Olson RL. Physiologic response of human skin to ultraviolet light. In: Urbach F, ed. The biologic effects of ultraviolet radiation (with emphasis on the skin). Oxford, England: Pergamon Press; 1969:181–6.
Boudreau Y, Decker J, Burton N, Moss CE, Mortimer V, Deitchman S. Health hazard evaluation report. Jackson Memorial Hospital, Miami, Florida. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1995; report no. HETA 91-187-2544.
Moss CE, Seitz T. Health Hazard Evaluation Report. John C. Murphy Family Health Center, Berkeley, Missouri. Cincinnati, OH: US Department of Health and Human Services, Public Health Service, CDC, National Institute for Occupational Safety and Health; 1992; HETA 91-148-2236.
Brubacher J, Hoffman RS. Hazards of ultraviolet lighting used for tuberculosis control. Chest 1996;109:582–3.
American Conference of Governmental Industrial Hygienists. 2004 TLVs(r) and BEIs(r). Based on the documentation of the threshold limit values for chemical substances and physical agents & biological exposure indices. Cincinnati, OH: American Conference of Governmental Industrial Hygienists; 2004.
Dumyahn T, First M. Characterization of ultraviolet upper room air disinfection devices. AIHA Journal 1999;60:219–27.
Rahn RO, Xu P, Miller SL. Dosimetry of room-air germicidal (254 nm) radiation using spherical actinometry. Photochem Photobiol 1999;70:314–8.
Ikeda RM, Birkhead GS, DiFerdinando GT Jr, et al. Nosocomial tuberculosis: an outbreak of a strain resistant to seven drugs. Infect Control Hosp Epidemiol 1995;16:152–9.
Fraser VJ, Johnson K, Primack J, Jones M, Medoff G, Dunagan WC. Evaluation of rooms with negative pressure ventilation used for respiratory isolation in seven midwestern hospitals. Infect Control Hosp Epidemiol 1993;14:623–8.
Sutton PM, Nicas M, Reinisch F, Harrison RJ. Evaluating the control of tuberculosis among healthcare workers: adherence to CDC guidelines of three urban hospitals in California. Infect Control Hosp Epidemiol 1998;19:487–93.
Streifel AJ. Design and maintenance of hospital ventilation systems and the prevention of airborne nosocomial infections. In: Mayall CG, ed. Hospital Epidemiology and Infection Control. 2 ed. Philadelphia, PA: Lippincot Williams and Wilkins; 1999:1211–21.
Bloom BR, Murray CJ. Tuberculosis: commentary on a reemergent killer. Science 1992;257:1055–64.
Nardell EA. Dodging droplet nuclei. Reducing the probability of nosocomial tuberculosis transmission in the AIDS era. Am Rev Respir Dis 1990;142:501–3.
Public Health Service, US Department of Health and Human Services. Approval of respiratory protective devices. Title 42, Code of Federal Regulations 2004. Part 84.
Occupational Safety and Health Administration. Respiratory protection program guidelines. Washington, DC: Occupational Safety and Health Administration; 2000. Directive number CPL 2-2.54A.
Hyatt EC. Current problems and new developments in respiratory protection. AIHA Journal 1963;24:295–304.
Rikimaru T, Kondo M, Kajimura K, et al. Efficacy of common antiseptics against multidrug-resistant Mycobacterium tuberculosis. Int J Tuberc Lung Dis 2002;6:763–70.
George RH. The prevention and control of mycobacterial infections in hospitals. J Hosp Infect 1988;11(Suppl A):386–92.
Johnson KR, Braden CR, Cairns KL, et al. Transmission of Mycobacterium tuberculosis from medical waste. JAMA 2000;284:1683–8.
Alvarado CJ, Reichelderfer M. APIC guideline for infection prevention and control in flexible endoscopy. Am J Infect Control 2000;28:138–55.
American Society for Gastrointestinal Endoscopy. Reprocessing of flexible gastrointestinal endoscopes. Gastrointest Endosc 1996;43:540–6.
American Society for Testing and Materials. Standard practice for cleaning and disinfection of flexible fiberoptic and video endoscopes used in the examination of the hollow viscera. West Conshohocken, PA: American Society for Testing and Materials; 2000.
Society of Gastroenterology Nurses and Associates, Inc. SGNA monograph series. Standards for infection control and reprocessing of flexible gastrointestinal endoscopes. Chicago, IL: Society of Gastroenterology Nurses and Associates, Inc.; 1997.
Axon ATR. World Congress of Gastroenterology. Working party report to the World Congress of Gastroenterology, Sydney, 1990. Disinfection and endoscopy: summary and recommendations. J Gastroenterol Hepatol 1991;6:23–4.
Favero MS, Bond WW. Chemical disinfection of medical and surgical materials [Chapter 35]. In: Block SS, ed. Disinfection, sterlization, and preservation. 4th ed. Philadelphia, PA: Lea & Febiger; 1991:617–41.
Food and Drug Administration, CDC. FDA and CDC Public Health Advisory: infections from endoscopes inadequately reprocessed by an automated endoscope reprocessing system. Rockville, MD: US Food and Drug Administration, Center for Devices and Radiological Health; 1999:1–5.
Terms and Abbreviations Used in this Report
ACET
Advisory Council for the Elimination of Tuberculosis
ACGIH
American Conference of Governmental Industrial
Hygienists
ACGIH
American Conference of Governmental Industrial
Hygienists
ACGIH
American Conference of Governmental Industrial
Hygienists
ACH
Air changes per hour
ACOG
American College of Obstetricians and Gynecologists
AERS
Adverse event reporting system
AFB
Acid-fast bacilli
AIA
American Institute of Architects
AIDS
Acquired immunodeficiency syndrome
AII
Airborne infection isolation
ALA
American Lung Association
ALT
Alanine aminotransferase
ANSI
American National Standards Institute
APF
Assigned protection factor
APIC
Association for Professionals in Infection Control
and Epidemiology, Inc.
ART
Antiretroviral therapy
ASHRAE
American Society of Heating, Refrigerating, and
Air-Conditioning Engineers, Inc.
AST
Aspartate aminotransferase
ATS
American Thoracic Society
BAMT
Blood assay for Mycobacterium tuberculosis
BCG
Bacille Calmette-Guérin
BIDR
Blinded independent duplicate reading
BMBL
Biosafety in Microbiological and Biomedical
Laboratories
BSL
Biosafety level
BSC
Biological safety cabinet
CAV
Constant air volume
CDC
Centers for Disease Control and Prevention
CEL
Certified equipment list
CFM
Cubic feet per minute
CFR
Code of Federal Regulations
CoV
Coronavirus
CPL
Compliance policy directive
CT
Computed tomography
DHHS
U.S. Department of Health and Human Services
DNA
Deoxyribonucleic acid
DTBE
Division of Tuberculosis Elimination
DOT
Directly observed therapy
DTH
Delayed-type hypersensitivity
ED
Emergency department
EMS
Emergency medical service
EPA
Environmental Protection Agency
ESRD
End-stage renal disease
ETL
Electrical Testing Laboratories
FDA
U.S. Food and Drug Administration
FGI
Facility Guideline Institute
FPM
Feet per minute
HAART
Highly active antiretroviral therapy
HCW
Health-care worker
HEPA
High-efficiency particulate air
HIV
Human immunodeficiency virus
HMO
Health maintenance organization
HPLC
High-pressure liquid chromatograph
HVAC
Heating, ventilation, air conditioning
ICU
Intensive care unit
IDSA
Infectious Diseases Society of America
IFN-γ
Inteferon-gamma
IGRA
Interferon gamma release assay
INH
Isoniazid
IUATLD
International Union Against Tuberculosis and Lung
Disease
JCAHO
Joint Commission on Accreditation of Healthcare
Organizations
LTBI
Latent tuberculosis infection
MDR
TB Multidrug-resistant tuberculosis
MOTT
Mycobacterium other than tuberculosis
NAA
Nucleic acid amplification
NCID
National Center for Infectious Diseases
NIAID
National Institute of Allergy and Infectious
Diseases
NIH
National Institutes of Health
NIOSH
National Institute for Occupational Safety and
Health
NM
Nanometer
NNRTI
Nonnucleoside reverse transcriptase inhibitors
NPIN
National Prevention Information Network
NTCA
National Tuberculosis Controllers Association
NTM
Nontuberculous mycobacteria
OR
Operating room
OSHA
Occupational Safety and Health Administration
PAPR
Powered air-purifying respirator
PCP
Pneumocystis pneumonia
PCR
Polymerase chain reaction
PE
Protective environment
PET
Permissible exposure time
PI
Protease inhibitor
PPD
Purified protein derivative
PPE
Personal protective equipment
QC
Quality control
QFT
QuantiFERON®-TB test
QFT-G
QuantiFERON®-TB Gold test
QLFT
Qualitative fit test
QNFT
Quantitative fit test
REL
Recommended exposure limit
RFLP
Restriction fragment length polymorphism
RNA
Ribonucleic acid
RZ
Rifampin and pyrazinamide
SARS
Severe acute respiratory syndrome
SGOT
Serum glutamic-oxalacetic transaminase*
SGPT
Serum glutamic-pyruvic transaminase†
SWPF
Simulated workplace protection factor
TB
Tuberculosis
TNF-α
Tumor necrosis factor-alpha
TU
Tuberculin unit
TST
Tuberculin skin test
UL
Underwriters Laboratories
UV
Ultraviolet
UVGI
Ultraviolet germicidal irradiation
VAV
Variable air volume
WHO
World Health Organization
WPF
Workplace protection factor
* Older term for AST.
† Older term for ALT.
Glossary of Definitions
acid-fast bacilli (AFB)
examination
A laboratory test that involves microscopic examination of a stained smear of a patient specimen (usually sputum) to determine if mycobacteria are present. A presumptive diagnosis of pulmonary tuberculosis (TB) can be made with a positive AFB sputum smear result; however, approximately 50% of patients with TB disease of the lungs have negative AFB sputum smear results. The diagnosis of TB disease is usually not confirmed until Mycobacterium tuberculosis is identified in culture or by a positive nucleic acid amplification (NAA) test result.
administrative controls
Managerial measures that reduce the risk for exposure to persons who might have TB disease. Examples include coordinating efforts with the local or state health department; conducting a TB risk assessment for the setting; developing and instituting a written TB infection-control plan to ensure prompt detection, airborne infection isolation (AII), and treatment of persons with suspected or confirmed TB disease; and screening and evaluating health-care workers (HCWs) who are at risk for TB disease or who might be exposed to M. tuberculosis.
aerosol
Dispersions of particles in a gaseous medium (e.g., air). Droplet nuclei are an example of particles that are expelled by a person with an infectious disease (e.g., by coughing, sneezing, or singing). For M. tuberculosis, the droplet nuclei are approximately 1–5 µm. Because of their small size, the droplet nuclei can remain suspended in the air for substantial periods and can transmit M. tuberculosis to other persons.
air change rate
Ratio of the airflow in volume units per hour to the volume of the space under consideration in identical volume units, usually expressed in air changes per hour (ACH).
air change rate
(equivalent)
Ratio of the volumetric air loss rate associated with an environmental control (or combination of controls) (e.g., an air cleaner or ultraviolet germicidal irradiation [UVGI] system) divided by the volume of the room where the control has been applied. The equivalent air change rate is useful for describing the rate at which bioaerosols are removed by means other than ventilation.
air change rate
(mechanical)
Ratio of the airflow to the space volume per unit time, usually expressed in air changes per hour (ACH).
air changes per hour
(ACH)
Air change rate expressed as the number of air exchange units per hour.
airborne infection
isolation (AII) precautions
The isolation of patients infected with organisms spread through airborne droplet nuclei 1–5 µm in diameter. This isolation area receives substantial ACH (≥12 ACH for new construction since 2001 and ≥6 ACH for construction before 2001) and is under negative pressure (i.e., the direction of the air flow is from the outside adjacent space [e.g., the corridor] into the room). The air in an AII room is preferably exhausted to the outside, but can be recirculated if the return air is filtered through an high efficiency particulate respirator (HEPA) filter.
AII room
A room designed to maintain AII. Formerly called negative pressure isolation room, an AII room is a single-occupancy patient-care room used to isolate persons with suspected or confirmed infectious TB disease. Environmental factors are controlled in AII rooms to minimize the transmission of infectious agents that are usually spread from person-to-person by droplet nuclei associated with coughing or aerosolization of contaminated fluids. AII rooms should provide negative pressure in the room (so that air flows under the door gap into the room), an air flow rate of 6–12 ACH, and direct exhaust of air from the room to the outside of the building or recirculation of air through a HEPA filter.
American Institute of
Architects/Facility Guideline Institute (AIA/FGI)
A professional organization that develops standards for building design and construction, including ventilation parameters, and enforced by the Joint Commission on Accreditation of Healthcare Organizations.
American Society of
Heating, Refrigerating, and Air-Conditioning Engineers, Inc. (ASHRAE)
A professional organization that develops guidelines for building ventilation.
aminotransaminases
Also called transaminases. Used to assess for hepatotoxicity in persons taking antituberculosis medications and include aspartate amino transferase (AST), serum glutamic oxalacetic transaminase, formerly SGOT, and amino alanine transferase, formerly ALT.
aminotransferases
Also called transaminases. Used to assess for hepatotoxicity in persons taking antituberculosis medications and include aspartate amino transferase (AST) (formerly serum glutamic oxalacetic transaminase) and amino alanine transferase (ALT) (formerly serum glutamic pyruvic transaminase).
anaphylactic shock
An often severe and sometimes fatal systemic reaction upon a second exposure to a specific antigen (as wasp venom or penicillin) after previous sensitization that is characterized especially by respiratory symptoms, fainting, itching, and hives.
anemometer
An instrument used to measure the velocity (speed) of air.
anergy
A condition in which a person has a diminished ability to exhibit delayed T-cell hypersensitivity to antigens because of a condition or situation resulting in altered immune function. An inability to react to a skin test is called cutaneous anergy. Skin tests for anergy (i.e., control antigens) have poor predictive value and are not recommended.
anteroom
Small room leading from a corridor into an AII room. An anteroom is separated from both the AII room and the corridor by doors. An anteroom can act as an airlock, preventing the escape of contaminants from the AII room into the corridor.
apical
Relating to or located at the tip (an apex).
assigned protection factor (APF)
The minimum anticipated protection provided by a properly worn and functioning respirator or class of respirators.
asymptomatic
Neither causing nor exhibiting signs or symptoms of disease.
Bacille Calmette-Guérin (BCG)
A vaccine for TB named after the French scientists Calmette and Guérin used in most countries where TB disease is endemic. The vaccine is effective in preventing disseminated and meningeal TB disease in infants and young children. It may have approximately 50% efficacy for preventing pulmonary TB disease in adults.
baseline TB screening
Screening HCWs for LTBI and TB disease at the beginning of employment. TB screening includes a symptom screen for all HCWs, and tuberculin skin tests (TSTs) or blood assay for Mycobacterium tuberculosis (BAMT) for those with previous negative test results for M. tuberculosis infection.
baseline TST or baseline BAMT
The TST or BAMT is administered at the beginning of employment to newly hired HCWs. If the TST method is used, for HCWs who have not had a documented negative test result for M. tuberculosis during the preceding 12 months, the baseline TST result should be obtained by using the two-step method. BAMT baseline testing does not need the two-step method.
biological safety cabinet (BSC)
A ventilated box that provides HCWs with a degree of protection against hazardous aerosols that are generated within it. BSC is the principal device used to contain infectious splashes or aerosols generated by multiple microbiology processes. BSC provides physical barriers and directional airflow to carry hazards away from the HCW. Maintenance is an essential part of ensuring proper BCS function.
Biosafety in
Microbiological and Biomedical Laboratories (BMBL)
A publication of the U.S. Public Health Service that describes the combinations of standard and special microbiology practices, safety equipment, and facilities constituting biosafety levels (BSLs) 1–4, which are recommended for work with various infectious agents in laboratory settings. The recommendations are advisory and intended to provide a voluntary guide or code of practice.
biosafety levels (BSLs)
Four BSLs are described in Section III of BMBL that comprise combinations of laboratory practices and techniques, safety equipment, and laboratory settings.
blinded independent
duplicate reading (BIDR)
Process in which two or more TST readers immediately measure the same TST result by standard procedures, without consulting or observing one another's readings, and record results. BIDRs help ensure that TST readers continue to read TST results correctly.
blood assay for
Mycobacterium tuberculosis (BAMT)
A general term to refer to recently developed in vitro diagnostic tests that assess for the presence of infection with M. tuberculosis. This term includes, but is not limited to, IFN-γ release assays (IGRA). In the United States, the currently available test is QuantiFERON®-TB Gold test (QFT-G).
BAMT converter
A change from a negative to a positive BAMT result over a 2-year period.
boosting
When nonspecific or remote sensitivity to tuberculin purified protein derivative (PPD) in the skin test wanes or disappears over time, subsequent TSTs can restore the sensitivity. This process is called boosting or the booster phenomenon. An initially small TST reaction size is followed by a substantial reaction size on a later test, and this increase in millimeters of induration can be confused with a conversion or a recent M. tuberculosis infection. Two-step testing is used to distinguish new infections from boosted reactions in infection-control surveillance programs.
bronchoscopy
A procedure for examining the lower respiratory tract in which the end of the endoscopic instrument is inserted through the mouth or nose (or tracheostomy) and into the respiratory tree. Bronchoscopy can be used to obtain diagnostic specimens. Bronchoscopy also creates a high risk for M. tuberculosis transmission to HCWs if it is performed on an untreated patient who has TB disease (even if the patient has negative AFB smear results) because it is a cough-inducing procedure.
case
A particular instance of a disease (e.g., TB). A case is detected, documented, and reported.
cavity (pulmonary)
A hole in the lung parenchyma, usually not involving the pleural space. Although a lung cavity can develop from multiple causes, and its appearance is similar regardless of its cause, in pulmonary TB disease, cavitation results from the destruction of pulmonary tissue by direct bacterial invasion and an immune interaction triggered by M. tuberculosis. A TB cavity substantial enough to see with a normal chest radiograph predicts infectiousness.
clinical examination
A physical evaluation of the clinical status of a patient by a physician or equivalent practitioner.
close contact (TB)
A person who has shared the same air space in a household or other enclosed environment for a prolonged period (days or weeks, not minutes or a couple hours) with a person with suspected or confirmed TB disease. Close contacts have also been referred to as high-priority contacts because they have the highest risk for infection with M. tuberculosis.
cluster (TB)
A group of patients with LTBI or TB disease that are linked by epidemiologic, location, or genotyping data. Two or more TST conversions within a short period can be a cluster of TB disease and might suggest transmission within the setting. A genotyping cluster is two or more cases with isolates that have an identical genotyping pattern.
Product certified by CDC's National Institute for Occupational Safety and Health (NIOSH) and cleared by the Food and Drug Administration (FDA) that provides both respiratory protection and bloodborne pathogen protection.
constant air volume (CAV)
A descriptor for an air-handling system which, as the name implies, supplies and exhausts air at a constant flow rate. The flow rate does not change over time based on temperature load or other parameters.
contact (TB)
Refers to someone who was exposed to M. tuberculosis infection by sharing air space with an infectious TB patient.
contact investigation
Procedures that occur when a case of infectious TB is identified, including finding persons (contacts) exposed to the case, testing and evaluation of contacts to identify LTBI or TB disease, and treatment of these persons, as indicated.
contagious
Describes a characteristic of a disease that can be transmitted from one living being to another through direct contact or indirect contact; communicable. The agent responsible for the contagious character of a disease is also described as being infectious; the usual culprits are microorganisms.
contraindication
Any condition, especially any condition of disease, which renders a certain line of treatment improper or undesirable.
conversion
See TST conversion.
conversion rate
The percentage of a population with a converted test result (TST or BAMT) for M. tuberculosis within a specified period. This is calculated by dividing the number of conversions among eligible HCWs in the setting in a specified period (numerator) by the number of HCWs who received tests in the setting over the same period (denominator) multiplied by 100.
culture
Growth of microorganisms in the laboratory performed for detection and identification in sputum or other body fluids and tissues. This test usually takes 2–4 weeks for mycobacteria to grow (2–4 days for most other bacteria).
cough etiquette
See respiratory hygiene and cough ettiquette.
cross contamination
When organisms from one sample are introduced into another sample, causing a false-positive result.
delayed-type hypersensitivity (DTH)
Cell-mediated inflammatory reaction to an antigen, which is recognized by the immune system usually because of previous exposure to the same antigen or similar ones. Cell-mediated reactions are contrasted with an antibody (or humoral) response. DTH typically peaks at 48–72 hours after exposure to the antigen.
deoxyribonucleic acid
DNA fingerprinting is a clinical laboratory technique used to distinguish between different strains of M. tuberculosis and to help assess the likelihood of TB transmission.
differential pressure
A measurable difference in air pressure that creates a directional airflow between adjacent compartmentalized spaces.
directly observed therapy
(DOT)
Adherence-enhancing strategy in which an HCW or other trained person watches a patient swallow each dose of medication. DOT is the standard care for all patients with TB disease and is a preferred option for patients treated for LTBI.
disposable respirator
A respirator designed to be used and then discarded; also known as a filtering-facepiece respirator. Respirators should be discarded after excessive resistance, physical damage, or hygiene considerations.
droplet nuclei
Microscopic particles produced when a person coughs, sneezes, shouts, or sings. These particles can remain suspended in the air for prolonged periods and can be carried on normal air currents in a room and beyond to adjacent spaces or areas receiving exhaust air.
drug-susceptibility test
A laboratory determination to assess whether an M. tuberculosis complex isolate is susceptible or resistant to antituberculosis drugs that are added to mycobacterial growth medium or are detected genetically. The results predict whether a specific drug is likely to be effective in treating TB disease caused by that isolate.
environmental control
measures
Physical or mechanical measures (as opposed to administrative control measures) used to reduce the risk for transmission of M. tuberculosis. Examples include ventilation, filtration, ultraviolet lamps, AII rooms, and local exhaust ventilation devices.
epidemiologic cluster
A closely grouped series of cases in time or place.
erythema
Abnormal redness of the skin. Erythema can develop around a TST site but should not be read as part of the TST result.
expert TST trainer
A designated instructor who has documented TST training experience. This may include having received training on placing and reading multiple TST results.
exposed cohorts
Groups of persons (e.g., family members, co-workers, friends, club, team or choir members, persons in correctional facilities, or homeless shelter residents) who have shared the same air space with the suspected patient with TB disease during the infectious period. A person in the exposed cohort is a contact. See also contact and close contact.
exposure
The condition of being subjected to something (e.g., an infectious agent) that could have an adverse health effect. A person exposed to M. tuberculosis does not necessarily become infected. See also transmission.
exposure period
The coincident period when a contact shared the same air space as the index TB patient during the infectious period.
exposure site
A location that the index patient visited during the infectious period (e.g., school, bar, bus, or residence).
extrapulmonary TB
TB disease in any part of the body other than the lungs (e.g., kidney, spine, or lymph nodes). The presence of extrapulmonary disease does not exclude pulmonary TB disease.
false-negative TST or BAMT
result
A TST or BAMT result that is interpreted as negative in a person who is actually infected with M. tuberculosis.
false-positive TST or BAMT
result
A TST or BAMT result that is interpreted as positive in a person who is not actually infected with M. tuberculosis. A false-positive TST result is more likely to occur in persons who have been vaccinated with BCG or who are infected with nontuberculous mycobacteria (NTM).
facility
A physical building or set of buildings.
filtering-facepiece
respirator
A type of air purifying respirator that uses a filter as an integral part of the facepiece or with the entire facepiece composed of the filtering medium.
fit check
See user-seal check.
fit factor
A quantitative estimate of the fit of a particular respirator to a specific person; typically estimates the ratio of the concentration of a substance in ambient air to its concentration inside the respirator when worn.
fit test
The use of a protocol to qualitatively or quantitatively evaluate the fit of a respirator on a person. See also QLFT and QNFT.
flutter strips
Physical indicators used to provide a continuous visual sign that a room is under negative pressure. These simple and inexpensive devices are placed directly in the door and can be useful in identifying a pressure differential problem.
genotype
The DNA pattern of M. tuberculosis used to discriminate among different strains.
health-care–associated
Broader term used instead of "nosocomial."
health-care setting
A place where health care is delivered.
health-care workers (HCWs)
All paid and unpaid persons working in health-care settings.
heating, ventilating, or
air conditioning (HVAC)
Mechanical systems that provide either collectively or individually heating, ventilating, or air conditioning for comfort within or associated with a building.
high efficiency
particulate air (HEPA) filter
A filter that is certified to remove ≥99.97% of particles 0.3 µm in size, including
M. tuberculosis–containing droplet nuclei; the filter can be either portable or stationary. Use of HEPA filters in building ventilation systems requires expertise in installation and maintenance.
high-pressure liquid
chromatograph(HPLC)
Laboratory method used to identify Mycobacterium species by analysis of species-specific fatty acids called mycolic acids, which are present in the cell walls of mycobacteria.
human immunodeficiency
virus (HIV) infection
Infection with the virus that causes acquired immunodeficiency syndrome (AIDS). A person with both LTBI and HIV infection is at high risk for developing TB disease.
hemoptysis
The expectoration or coughing up of blood or blood-tinged sputum; one of the symptoms of pulmonary TB disease. Hemoptysis can also be observed in other pulmonary conditions (e.g., lung cancer).
hypersensitivity
A state in which the body reacts with an exaggerated immune response to a foreign substance. Hypersensitivity reactions are classified as immediate or delayed, types I and IV, respectively. See also delayed-type hypersensitivity.
immunocompromised and immunosuppressed
Describes conditions in which at least part of the immune system is functioning at less than normal capacity. According to certain style experts, "immunocompromised" is the broader term, and "immunosuppressed" is restricted to conditions with iatrogenic causes, including treatments for another condition.
incentive
A gift given to patients to encourage or acknowledge their adherence to treatment.
incidence
The number of new events or cases of disease that develop during a specified period.
index case
The first person with TB disease who is identified in a particular setting. This person might be an indicator of a potential public health problem and is not necessarily the source case. See also source case or patient.
induration
The firmness in the skin test reaction; produced by immune-cell infiltration in response to the tuberculin antigen that was introduced into the skin. Induration is measured transversely by palpation, and the result is recorded in millimeters. The measurement is compared with guidelines to determine whether the test result is classified as positive or negative.
infection with M. tuberculosis
In some persons who are exposed to and who inhale M. tuberculosis bacteria, the bacteria are not promptly cleared by respiratory defense systems, and the bacteria multiply and are spread throughout the body, thereby infecting the exposed person. In the majority of persons who become infected, the body is able to fight the bacteria to stop the bacteria from growing, further establishing a latent state. The bacteria are inactive, but they remain alive in the body and can become active later. In other persons, the infection with M. tuberculosis can progress to TB disease more promptly. M. tuberculosis infection encompasses both latent TB infection and TB disease. See also latent TB infection and reinfection.
infectious
See contagious.
infectious droplet nuclei
Droplet nuclei produced by an infectious TB patient that can carry tubercle bacteria and be inhaled by others. Although usually produced from patients with pulmonary TB through coughing, aerosol-generating procedures can also generate infectious droplet nuclei.
infectious period
The period during which a person with TB disease might have transmitted M. tuberculosis organisms to others. For patients with positive AFB sputum smear results, the infectious period begins 3 months before the collection date of the first positive smear result or the symptom onset date (whichever is earlier) and ends when the patient is placed into AII or the date of collection for the first of consistently negative smear results. For patients with negative AFB sputum smear results, the infectious period extends from 1 month before the symptom onset date and ends when the patient is placed into AII (whichever was earlier).
interferon-γ release assays (IGRA)
A type of an ex vivo test that detects cell-mediated immune response to this cytokine. In the United States, QFT-G is a currently available IGRA.
isoniazid (INH)
A highly active antituberculosis chemotherapeutic agent that is a cornerstone of treatment for TB disease and the cornerstone of treatment for LTBI.
laryngeal TB
A form of TB disease that involves the larynx and can be highly infectious.
latent TB infection (LTBI)
Infection with M. tuberculosis without symptoms or signs of disease have manifested. See also Infection with M. tuberculosis.
manometer
An instrument used to measure pressure differentials (i.e., pressure inside an AII room relative to the corridor of the room).
Mantoux method
A skin test performed by intradermally injecting 0.1 mL of PPD tuberculin solution into the volar or dorsal surface of the forearm. This method is the recommended method for TST.
mask
A device worn over the nose and mouth of a person with suspected or confirmed infectious TB disease to prevent infectious particles from being released into room air.
mechanical ACH
Air change rate based on only the mechanical ventilation flowrates.
medical evaluation
An examination to diagnose TB disease or LTBI, to select treatment, and to assess response to therapy. A medical evaluation can include medical history and TB symptom screen, clinical or physical examination, screening and diagnostic tests (e.g., TSTs, chest radiographs, bacteriologic examination, and HIV testing), counseling, and treatment referrals.
meningeal TB
A serious form of TB disease involving the meningies, the covering of the brain. Meningeal TB can result in serious neurologic complications.
miliary TB
A serious form of TB disease sometimes referred to as disseminated TB. A dangerous and difficult form to diagnose of rapidly progressing TB disease that extends throughout the body. Uniformly fatal if untreated; in certain instances, it is diagnosed too late to save a life. Certain patients with this condition have normal findings or ordinary infiltrates on the chest radiograph.
mitogen
A substance that stimulates the growth of certain white blood cells. Mitogen is used as a positive control in BAMT tests.
multidrug-resistant
tuberculosis (MDR TB)
TB disease caused by M. tuberculosis organisms that are resistant to at least INH and rifampin.
mycobacteria other than tuberculosis (MOTT)
See NTM.
Mycobacterium
tuberculosis
The namesake member organism of M. tuberculosis complex and the most common causative infectious agent of TB disease in humans. In certain instances, the species name refers to the entire M. tuberculosis complex, which includes M. bovis, M. african, M. microti, M. canetii, M. caprae, and M. pinnipedii.
M. tuberculosis
culture
A laboratory test in which the organism is grown from a submitted specimen (e.g., sputum) to determine the presence of M. tuberculosis. In the absence of cross-contamination, a positive culture confirms the diagnosis of TB disease.
N95 disposable respirator
An air-purifying, filtering-facepiece respirator that is ≥95% efficient at removing 0.3 µm particles and is not resistant to oil. See also respirator.
negative pressure
The difference in air-pressure between two areas. A room that is under negative pressure has a lower pressure than adjacent areas, which keeps air from flowing out of the room and into adjacent rooms or areas. Also used to describe a nonpowered respirator. See also AII and AII room.
nontuberculous mycobacteria (NTM)
Refers to mycobacterium species other than those included as part of M. tuberculosis complex. Although valid from a laboratory perspective, the term can be misleading because certain types of NTM cause disease with pathologic and clinical manifestations similar to TB disease. Another term for NTM is mycobacterium other than tuberculosis (MOTT). NTM are environmental mycobacteria.
nosocomial
Acquired in a hospital. The broader term "health-care–associated" is used in this report.
nucleic acid amplification (NAA)
Laboratory method used to target and amplify a single DNA or RNA sequence usually for detecting and identifying a microorganism. The NAA tests for M. tuberculosis complex are sensitive and specific and can accelerate the confirmation of pulmonary TB disease.
periodic fit testing
Repetition of fit testing performed in accordance with local, state, and federal regulations. Additional fit testing should be used when 1) a new model of respirator is used, 2) a physical characteristic of the user changes, or 3) when the user or respiratory program administrator is uncertain that the HCW is obtaining an adequate fit.
pleural effusion
Abnormal accumulation of fluid between the lining of the lung and the chest wall. Persons with TB pleural effusions might also have concurrent unsuspected pulmonary or laryngeal TB disease. These patients should be considered contagious until infectious TB disease is excluded.
polymerase chain reaction (PCR)
A system for in vitro amplification of DNA that can be used for diagnosis of infections.
positive predictive value of a TST
The probability that a person with a positive TST result is actually infected with M. tuberculosis. The positive predictive value is dependent on the prevalence of infection with M. tuberculosis in the population being tested and on the sensitivity and specificity of the test.
potential ongoing
transmission
A risk classification for TB screening, including testing for M. tuberculosis infection when evidence of ongoing transmission of M. tuberculosis is apparent in the setting. Testing might need to be performed every 8–10 weeks until lapses in infection controls have been corrected, and no further evidence of ongoing transmission is apparent. Use potential ongoing transmission as a temporary risk classification only. After corrective steps are taken, reclassify the setting as medium risk. Maintaining the classification of medium risk for at least 1 year is recommended.
powered air-purifying
respirator (PAPR)
A respirator equipped with a tight-fitting facepiece (rubber facepiece) or loose-fitting facepiece (hood or helmet), breathing tube, air-purifying filter, cartridge or canister, and a fan. Air is drawn through the air-purifying element and pushed through the breathing tube and into the facepiece, hood, or helmet by the fan. Loose-fitting PAPRs (e.g., hoods or helmets) might be useful for persons with facial hair because they do not require a tight seal with the face.
prevalence
The proportion of persons in a population who have a disease at a specific time.
protection factor
A general term for three specific terms: 1) APF, 2) SWPF, and 3) WPF. These terms refer to different methods of defining adequacy of respirator fit. See also APF, SWPF, and WPF.
pulmonary TB
TB disease that occurs in the lung parenchyma, usually producing a cough that lasts ≥3 weeks.
purified protein derivative (PPD)
tuberculin
A material used in diagnostic tests for detecting infection with M. tuberculosis. In the United States, PPD solution is approved for administration as an intradermal injection (5 TU per 0.1 mL), a diagnostic aid for LTBI (see TST). In addition, PPD tuberculin was one of the antigens in the first-generation QFT.
qualitative fit test (QLFT)
A pass-fail fit test to assess the adequacy of respirator fit that relies on the response of the person to the test agent.
quality control (QC)
A function to ensure that project tools and procedures are reviewed and verified according to project standards.
QFT and QFT-G
Types of BAMT that are in vitro cytokine assays that detects cell-mediated immune response (see also DTH) to M. tuberculosis in heparinized whole blood from venipuncture. This test requires only a single patient encounter, and the result can be ready within 1 day. In 2005, QuantiFERON(r)-TB was replaced by QuantiFERON(r)-TB Gold (QFT-G), which has greater specificity because of antigen selection. QFT-G appears to be capable of distinguishing between the sensitization caused by M. tuberculosis infection and that caused by BCG vaccination.
quantitative fit test (QNFT)
An assessment of the adequacy of respirator fit by numerically measuring the amount of leakage into the respirator.
recirculation
Ventilation in which all or the majority of the air exhausted from an area is returned to the same area or other areas of the setting.
recommended exposure
limit (REL)
The occupational exposure
limit established by CDC/NIOSH. RELs are intended to
suggest levels of exposure to which the majority of HCWs
can be exposed without experiencing adverse health
effects.
reinfection
A second infection that follows from a previous infection by the same causative agent. Frequently used when referring to an episode of TB disease resulting from a subsequent infection with M. tuberculosis and a different genotype.
resistance
The ability of certain strains of mycobacteria, including M. tuberculosis, to grow and multiply in the presence of certain drugs that ordinarily kill or suppress them. Such strains are referred to as drug-resistant strains and cause drug-resistant TB disease. See also multidrug-resistant TB.
respirator
A CDC/NIOSH-approved device worn to prevent inhalation of airborne contaminants.
respiratory hygiene and
cough etiquette
Procedures by which patients with suspected or confirmed infectious TB disease can minimize the spread of infectious droplet nuclei by decreasing the number of infectious particles that are released into the environment. Patients with a cough should be instructed to turn their heads away from persons and to cover their mouth and nose with their hands or preferably a cloth or tissue when coughing or sneezing.
respiratory protection
The third level in the hierarchy of TB infection-control measures after administrative and environmental controls is used because of the risk for exposure.
restriction fragment
length polymorphism (RFLP)
A technique by which organisms can be differentiated by analysis of patterns derived from cleavage of their DNA. The similarity of the patterns generated can be used to differentiate strains from one another. See also genotype.
reversion
A subsequent TST or BAMT result that is substantially smaller than a previous test; reversion has been observed to be more likely when the intervening time between TSTs increases.
Rifampin
A highly active antituberculosis chemotherapeutic agent that is a cornerstone of treatment for TB disease.
screening (TB)
Measures used to identify persons who have TB disease or LTBI. See also symptom screen.
secondary (TB) case
A new case of TB disease that is attributed to recent transmission as part of the scenario under investigation. The period for "recent" is not defined but usually will be briefer than 2 years. Technically, all cases are secondary, in that they originate from other contagious cases.
simulated workplace
protection factor (SWPF)
A surrogate measure of the workplace protection provided by a respirator.
smear (AFB smear)
A laboratory technique for preparing a specimen so that bacteria can be visualized microscopically. Material from the specimen is spread onto a glass slide and usually dried and stained. Specific smear, stain, and microscopy methods for mycobacteria are designed to optimally detect members of this genus. The slide can be scanned by light or fluorescent high-power microscopy. These methods require ongoing quality assurance for prompt and reliable results. The results for sputum smears usually are reported as numbers of AFB per high-powered microscopy field or as a graded result, from +1 to +4. The quantity of stained organisms predicts infectiousness. See also AFB.
source case or patient
The person or the case that was the original source of infection for secondary cases or contacts. The source case can be, but is not necessarily, the index case.
source case investigation
An investigation to determine the source case could be conducted in at least two circumstances: 1) when a health-care setting detects an unexplained cluster of TST conversions among HCWs or 2) when TB infection or disease is diagnosed in a young child. The purposes of a source case investigation are to ascertain that the source case has been diagnosed and treated, to prevent further M. tuberculosis transmission, and to ensure that other contacts of that source case are also evaluated and, if indicated, provided treatment.
source control
A process for preventing or minimizing emission (e.g., aerosolized M. tuberculosis) at the place of origin. Examples of source-control methods are booths in which a patient coughs and produces sputum, BSCs in laboratories, and local exhaust ventilation.
spirometry
A procedure used to measure time expired and the volume inspired, and from these measurements, calculations can be made on the effectiveness of the lungs.
sputum
Mucus containing secretions coughed up from inside the lungs. Tests of sputum (e.g., smear and culture) can confirm pulmonary TB disease. Sputum is different from saliva or nasal secretions, which are unsatisfactory specimens for detecting TB disease. However, specimens suspected to be inadequate should still be processed because positive culture results can still be obtained and might be the only bacteriologic indication of disease.
sputum induction
A method used to obtain sputum from a patient who is unable to cough up a specimen spontaneously. The patient inhales a saline mist, which stimulates coughing from deep inside the lungs.
supervised TST
administration
A procedure in which an expert TST trainer supervises a TST trainee who performs all procedures on the procedural observation checklist for administering TSTs.
supervised TST reading
A procedure in which an expert TST trainer supervises a TST trainee who performs all procedures on the procedural observation checklist for reading TST results.
suspected TB
A tentative diagnosis of TB that will be confirmed or excluded by subsequent testing. Cases should not remain in this category for longer than 3 months.
symptomatic
A term applied to a patient with health-related complaints (symptoms) that might indicate the presence of disease. In certain instances, the term is applied to a medical condition (e.g., symptomatic pulmonary TB).
symptom screen
A procedure used during a clinical evaluation in which patients are asked if they have experienced any departure from normal in function, appearance, or sensation related to TB disease (e.g., cough).
targeted testing
A strategy to focus testing for infection with M. tuberculosis in persons at high risk for LTBI and for those at high risk for progression to TB disease if infected.
tuberculosis (TB) disease
Condition caused by infection with a member of the M. tuberculosis complex that has progressed to causing clinical (manifesting symptoms or signs) or subclinical (early stage of disease in which signs or symptoms are not present, but other indications of disease activity are present [see below]) illness. The bacteria can attack any part of the body, but disease is most commonly found in the lungs (pulmonary TB). Pulmonary TB disease can be infectious, whereas extrapulmonary disease (occurring at a body site outside the lungs) is not infectious, except in rare circumstances. When the only clinical finding is specific chest radiographic abnormalities, the condition is termed "inactive TB" and can be differentiated from active TB disease, which is accompanied by symptoms or other indications of disease activity (e.g., the ability to culture reproducing TB organisms from respiratory secretions or specific chest radiographic finding).
TB case
A particular episode of clinical TB disease. Refers only to the disease, not to the person with the disease. According to local laws and regulation, TB cases and suspect TB cases must be reported to the local or state health department.
TB contact
A person who has shared the same air space with a person who has TB disease for a sufficient amount of time to allow possible transmission of M. tuberculosis.
TB exposure incident
A situation in which persons (e.g., HCWs, visitors, and inmates) have been exposed to a person with suspected or confirmed infectious TB disease (or to air containing M. tuberculosis), without the benefit of effective infection-control measures.
TB infection
See LTBI.
TB infection-control
program
A program designed to control transmission of M. tuberculosis through early detection, isolation, and treatment of persons with infectious TB. A hierarchy of control measures are used, including 1) administrative controls to reduce the risk for exposure to persons with infectious TB disease and screening for HCWs for LTBI and TB disease, 2) environmental controls to prevent the spread and reduce the concentration of infectious droplet nuclei in the air, and 3) respiratory protection in areas where the risk for exposure to M. tuberculosis is high (e.g., AII rooms). A TB infection-control plan should include surveillance of HCWs who have unprotected high-risk exposure to TB patients or their environment of care.
TB screening
An administrative control measure in which evaluation for LTBI and TB disease are performed through initial and serial screening of HCWs, as indicated. Evaluation might comprise TST, BAMT, chest radiograph, and symptom screening. See also symptom screen.
TB screening program
A plan that health-care settings should implement to provide information that is critical in caring for HCWs and information and that facilitates detection of M. tuberculosis transmission. The TB screening program comprises four major components: 1) baseline testing for M. tuberculosis infection, 2) serial testing for M. tuberculosis infection, 3) serial screening for signs or symptoms of TB disease, and 4) TB training and education.
TB risk assessment
An initial and ongoing evaluation of the risk for transmission of M. tuberculosis in a particular health-care setting. To perform a risk assessment, the following factors should be considered: the community rate of TB, number of TB patients encountered in the setting, and the speed with which patients with TB disease are suspected, isolated, and evaluated. The TB risk assessment determines the types of administrative and environmental controls and respiratory protection needed for a setting.
transmission
Any mode or mechanism by which an infectious agent is spread from a source through the environment or to a person (or other living organism). In the context of health-care–associated TB infection control, transmission is the airborne conveyance of aerosolized M. tuberculosis contained in droplet nuclei from a person with TB disease, usually from the respiratory tract, to another person, resulting in infection.
treatment for LTBI
Treatment that prevents the progression of infection into disease.
tuberculin skin test (TST)
A diagnostic aid for finding M. tuberculosis infection. A small dose of tuberculin is injected just beneath the surface of the skin (in the United States by the Mantoux method), and the area is examined for induration by palpation 48–72 hours after the injection. The indurated margins should be read transverse (perpendicular) to the long axis of the forearm. See also Mantoux method and PPD.
TST conversion
A change in the result of a test for M. tuberculosis infection wherein the condition is interpreted as having progressed from uninfected to infected. An increase of ≥10 mm in induration during a maximum of 2 years is defined as a TST conversion for the purposes of a contact investigation. A TST conversion is presumptive evidence of new M. tuberculosis infection and poses an increased risk for progression to TB disease. See also conversion rate.
tubercle bacilli
M. tuberculosis organisms.
tuberculin
A precipitate made from a sterile filtrate of M. tuberculosis culture medium.
tumor necrosis factor-alpha (TNF-α)
A small molecule (called a cytokine) discovered in the blood of animals (and humans) with tumors but which has subsequently been determined to be an essential host mediator of infection and inflammation. TNF-α is released when humans are exposed to bacterial products (e.g., lipopolysaccharide) or BCG. Drugs (agents) that block human TNF-α have been demonstrated to increase the risk for progression to TB disease in persons who are latently infected.
two-step TST
Procedure used for the baseline skin testing of persons who will receive serial TSTs (e.g., HCWs and residents or staff of correctional facilities or long-term–care facilities) to reduce the likelihood of mistaking a boosted reaction for a new infection. If an initial TST result is classified as negative, a second step of a two-step TST should be administered 1–3 weeks after the first TST result was read. If the second TST result is positive, it probably represents a boosted reaction, indicating infection most likely occurred in the past and not recently. If the second TST result is also negative, the person is classified as not infected. Two-step skin testing has no place in contact investigations or in other circumstances in which ongoing transmission of M. tuberculosis is suspected.
ulceration (TST)
A break in the skin or mucosa with loss of surface tissue.
ultraviolet germicidal
radiation (UVGI)
Use of ultraviolet germicidal irradiation to kill or inactivate microorganisms.
UVGI lamp
An environmental control measure that includes a lamp that kills or inactivates microorganisms by emitting ultraviolet germicidal irradiation, predominantly at a wavelength of 254 nm (intermediate light waves between visible light and radiographs). UVGI lamps can be used in ceiling or wall fixtures or within air ducts of ventilation systems as an adjunct to other environmental control measures.
user-seal check
Formerly called "fit check." A procedure performed after every respirator is donned to check for proper seal of the respirator.
variable air volume (VAV)
VAV ventilation systems are designed to vary the quantity of air delivered to a space while maintaining a constant supply air temperature to achieve the desired temperature in the occupied space. Minimum levels are mechanical, and outside air is maintained.
vesiculation
An abnormal elevation of the outer layer of skin enclosing a watery liquid; blister.
wheal
A small bump that is produced when a TST is administered. The wheal disappears in approximately 10 minutes after TST placement.
workplace protection factor (WPF)
A measure of the protection provided in the workplace by a properly functioning respirator when correctly worn and used.
Guidelines for Preventing the Transmission of Mycobacterium tuberculosis in Health-Care Settings, 2005
TB Infection-Control Guidelines Work Group: Diane I. Bennett, MD, Michael F. Iademarco, MD, Paul A. Jensen, PhD, Lauren A. Lambert, MPH, Beverly Metchock, DrPH, Renee Ridzon, MD, Division of Tuberculosis Elimination, National Center for HIV, STD and TB Prevention, CDC (Currently with the Bill and Melinda Gates Foundation); Paul M. Arguin, MD, Denise M. Cardo, MD, Amy B. Curtis, PhD, Adelisa L. Panlilio, MD, Patricia M. Simone, MD, Division of Global Migration and Quarantine, National Center for Infectious Diseases, CDC; Jennifer L. Cleveland, DMD, Amy S. Collins, MPH, Division of Oral Health, National Center for Chronic Disease Prevention and Health Promotion, CDC; G. Scott Earnest, PhD, Division of Applied Research and Technology, National Institute for Occupational Safety and Health, CDC; Teri Palermo, Division of Respiratory Disease Studies, National Institute for Occupational Safety and Health, CDC; Teresa A. Seitz, MPH, Division of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health; Yona Hackl, MS, Occupational Health and Safety, Office of the Director, CDC; Jonathan Y. Richmond, PhD (Retired), Office of Health and Safety, Office of the Director, CDC; John C. Ridderhof, DrPH, Division of Public Health Partnerships, National Center for Health Marketing, CDC; Allison Greenspan, Office of the Director, National Center for Infectious Diseases, CDC.
External Contributors: James August, MPH, American Federation of State, County and Municipal Employees, Washington, DC; Scott Barnhart, MD, Harborview Medical Center, Seattle, Washington; Joe Bick, MD, University of California, Davis, California; Henry Blumberg, MD, Emory University, Atlanta, Georgia; Dorothy Dougherty, Occupational Safety and Health Administration, Washington, DC; Charles E. Dunn, Sr, Commercial Lighting Design, Inc. (Lumalier), Memphis, Tennessee; Amanda L. Edens, MPH, Occupational Safety and Health Administration, Washington, DC, New Jersey Medical School, Newark, New Jersey; Kevin Fennelly, MD, New Jersey Medical School, Newark, New Jersey; Victoria Fraser, MD, Washington University School of Medicine, St. Louis, Missouri; Mary Gilchrist, PhD, University Hygienic Laboratory, Iowa City, Iowa; Robert J. Harrison, MD, California Department of Health Services, Oakland, California; Denise Ingman, U.S. Department of Health and Human Services, Helena, Montana; Pam Kellner, MPH, New York City Department of Health, New York, New York; James McAuley, MD, Rush-Presbyterian-St. Luke's Medical Center, Chicago, Illinois; Roy McKay, PhD, University of Cincinnati, Cincinnati, Ohio; Dick Menzies, MD, McGill University, Montreal, Canada; Shelly L. Miller, PhD, University of Colorado, Boulder, Colorado; Jose Montero, MD, New Hampshire Department of Health and Human Services, Concord, New Hampshire; Edward Nardell, MD, Harvard Medical School, Boston, Massachusetts; Mark Nicas, PhD, University of California at Berkeley, Berkeley, California; Paul S. Ninomura, Health Resources and Services Administration, Seattle, Washington; Tholief O'Flaherty, PhD, New York City Department of Health, New York, New York; Nicholas Pavelchak, New York State Department of Health, Troy, New York; Jean Pottinger, MA, University of Iowa, Iowa City, Iowa; Gina Pugliese, MS, Premier Safety Institute, Chicago, Illinois; Randall Reves, MD, Denver Public Health Department, Denver, Colorado; Jane Siegel, MD, University of Texas, Dallas, Texas; Kent Sepkowitz, MD, Memorial Sloan-Kettering Cancer Center, New York, New York; Andrew J. Streifel, MS, University of Minnesota, Minneapolis, Minnesota; Rachel L. Stricof, MPH, New York State Department of Health, Albany, New York; Michael L. Tapper, MD, Lenox Hill Hospital, New York, New York; Robert Weinstein, MD, Healthcare Infection Control Practices Advisory Committee; Sharon Welbel, MD, Cook County Hospital, Chicago, Illinois; Karen Worthington, MS, Occupational Safety and Health Administration, Lambertville, New Jersey.
CDC Contributors: Heinz William Ahlers, JD, National Institute for Occupational Safety and Health, CDC, Pittsburgh, Pennsylvania; Gabrielle Benenson, MPH, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Roland BerryAnn, National Institute for Occupational Safety and Health, CDC, Pittsburgh, Pennsylvania; Regina Bess, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Yvonne Boudreau, MD, National Institute for Occupational Safety and Health, CDC, Denver, Colorado; Kenneth G. Castro, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; L. Casey Chosewood, MD, Office of Health and Safety, CDC, Atlanta, Georgia; Christopher C. Coffey, PhD, National Institute for Occupational Safety and Health, CDC, Morgantown, West Virginia; Janet L. Collins, PhD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Maria Fraire, MPH, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Judy Gibson, MSN, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Robert C. Good, PhD (Retired), National Center for Infectious Diseases, CDC, Atlanta, Georgia; Maryam Haddad, MSN, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Connie Henderson, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Kashef Ijaz, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; William R. Jarvis, MD (Retired), National Center for Infectious Diseases, CDC, Atlanta, Georgia; John A. Jereb, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Margaret Kitt, MD, National Institute for Occupational Safety and Health, CDC, Morgantown, West Virginia; Mark Lobato, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Suzanne Marks, MPH, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Stephen B. Martin, Jr., National Institute for Occupational Safety and Health, CDC, Morgantown, West Virginia; Kenneth F. Martinez, MSEE, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Jerry Mazurek, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; R. Leroy Mickelsen, MS, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Vincent Mortimer, MS (Retired), National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Glenda Newell, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Tanja Popovic, MD, Office of the Director, CDC, Atlanta, Georgia; Laurence D. Reed, MS, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Apavoo Rengasamy, PhD, National Institute for Occupational Safety and Health, CDC, Pittsburgh, Pennsylvania; Millie P. Schafer, PhD, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Philip Spradling, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; James W. Stephens, PhD, National Institute for Occupational Safety and Health, CDC, Atlanta, GA; Carol M. Stephenson, PhD, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Zachary Taylor, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Tonya Thrash, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Douglas B. Trout, MD, National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio; Andrew Vernon, MD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Gregory R. Wagner, MD, National Institute for Occupational Safety and Health, CDC, Washington, DC; Wanda Walton, PhD, National Center for HIV, STD, and TB Prevention, CDC, Atlanta, Georgia; Angela M. Weber, MS, National Center for Environmental Health, CDC, Atlanta, Georgia; Robbin S. Weyant, PhD, Office of Health and Safety, CDC, Atlanta, Georgia; John J. Whalen, MS (Retired), National Institute for Occupational Safety and Health, CDC, Cincinnati, Ohio.
TABLE 1. Air changes per hour (ACH) and time required for removal efficiencies of 99% and 99.9% of airborne contaminants*
BOX 1. Indications for two-step tuberculin skin tests (TSTs)
TABLE 2. Ventilation recommendations for selected areas in new or renovated health-care settings
BOX 2. Interpretation of QuantiFERON(r)-TB Gold test (QFT-G) results
FIGURE 1. The tuberculin skin test result in this picture should be recorded as 16 mm. The "0" mm ruler line is inside the edge of the left dot.
BOX 3. Interpretations of tuberculin skin test (TST) and QuantiFERON(r)-TB test (QFT) results according to the purpose of testing for Mycobacterium tuberculosis infection in a health-care setting
TABLE 3. Standard drug regimens for treatment of latent TB infection (LTBI)*
BOX 4. Conditions requiring caution in interpreting negative QuantiFERON(r)-TB Gold test results
BOX 5. Factors affecting treatment decisions during the medical and diagnostic evaluation, by tuberculin skin test (TST) result
FIGURE 2. An enclosing booth designed to sweep air past a patient with tuberculosis disease and collect the infectious droplet nuclei on a high efficiency particular air (HEPA) filter
FIGURE 3. Room airflow patterns designed to provide mixing of air and prevent short-circuiting*
* Short-circuiting is the passage of air directly from the air supply to the exhaust.
FIGURE 4. Empirical relation between differential airflow, differential pressure, and leakage areas*
* Black solid lines indicate leakage areas. SOURCE: Hayden II CS, Fischbach TJ, Johnston OE, Hughes RT, Jensen PA. A model for calculating leakage areas into negative pressure isolation rooms. Cincinnati, OH: US Department of Health and Human Services, CDC; 1996.
FIGURE 5. Smoke tube testing and manometer placement to determine the direction of airflow into and out of a room
FIGURE 6. Cross-sectional view of a room indicating the location of negative pressure measurement*
* Airflow pressure at location 1 might differ from that at location 2. Measure pressure at location 2 for correct indication of negative pressure.
FIGURE 7. Fixed ducted room-air recirculation system using a high efficiency particulate air (HEPA) filter inside an air duct
FIGURE 8. Fixed ceiling-mounted room-air recirculation system using a high efficiency particulate air (HEPA) filter
BOX 6. Examples of ultraviolet germicidal irradiation (UVGI) signs
Appendix A. Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix A. (Continued) Administrative, environmental, and respiratory-protection controls for selected health-care settings
Appendix B. Tuberculosis (TB) risk assessment worksheet
Appendix B. (Continued) Tuberculosis (TB) risk assessment worksheet
Appendix B. (Continued) Tuberculosis (TB) risk assessment worksheet
Appendix B. (Continued) Tuberculosis (TB) risk assessment worksheet
Appendix B. (Continued) Tuberculosis (TB) risk assessment worksheet
Appendix B. (Continued) Tuberculosis (TB) risk assessment worksheet
Appendix C. Risk classifications for various health-care settings and recommended frequency of screening for Mycobacterium tuberculosis infection among health-care workers (HCWs)*
Appendix D. Environmental controls record and evaluation*
Appendix E. Tuberculosis (TB) Internet addresses
Appendix E. (Continued) Tuberculosis (TB) Internet addresses
Appendix F. Quality control (QC) procedural observation checklists
Appendix F. (Continued) Quality control (QC) procedural observation checklists
Appendix G. Model framework for medical evaluation request and questionnaire for users of N95 disposable respirators
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.
Centers for Disease Control and Prevention 1600 Clifton Road Atlanta, GA 30329-4027, USA
800-CDC-INFO (800-232-4636) TTY: (888) 232-6348 - Contact CDC–INFO