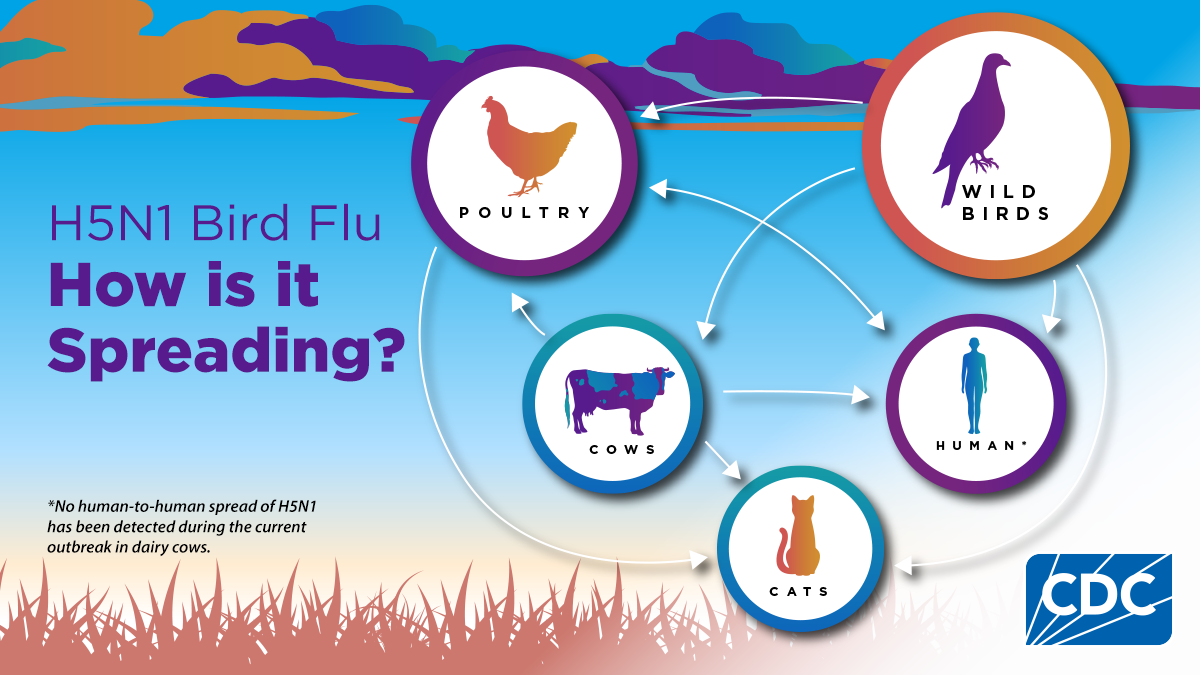
H5 bird flu is causing outbreaks in wild birds and poultry, other animals and sporadic human cases.

Learn about signs and symptoms of bird flu in people
Find the latest information about detections of H5N1 bird flu in people.
A multi-state outbreak of HPAI A(H5N1) bird flu in dairy cows was first reported on March 25, 2024.
Featured

CDC surveillance shows no indicators of unusual flu activity in people, including H5N1 bird flu.

This page outlines CDC’s recommendations for preventing exposure to avian influenza viruses.

A collection of materials and tools to help educate and inform the public about bird flu