 ShareCompartir
ShareCompartir

Monthy Case Studies - 2000
Case #47 - November, 2000
A 4-year-old girl from Mexico City was seen by her pediatrician for chronic diarrhea of three months duration. Her mother is HIV-positive and was undergoing therapy for HIV at the time of the examination. A smear of the girl's stool was stained with Chromotrope 2R and examined for ova and parasites. In the smear, oval-shaped objects were observed (1000×, indicated by arrows in Figure A). The objects averaged 1.3 to 2.7 micrometers in diameter. What is your diagnosis? Based on what criteria? Would you recommend any other laboratory tests?
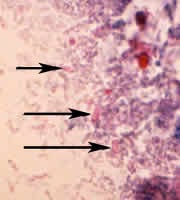
Figure A
Answer to Case #47
This was a case of microsporidiosis. The objects shown in Figure A are microsporidia spores. The microsporidia species was found to be Encephalitozoon intestinalis by PCR with diagnostic primers. Other techniques used for speciation of microsporidia include immunofluorescence assays and transmission electron microscopy. These techniques are generally only available in research laboratories.
The morphological diagnostic features observed were:
- the shape of the spores of microsporidia (round to oval). They will stain pinkish red when using the Chromotrope 2R staining technique. Often, an equatorial belt-like stripe can be seen in the spores.
- the size of the spores. Encephalitozoon spp. measure 1.0 to 1.5 by 2.5 to 3.0 micrometers, consistently appearing larger than Enterocytozoon bieneusi spores (0.8 to 1.4 micrometers). Enterocytozoon bieneusi is the most commonly recognized species causing diarrhea in immunocompromised patients. The difference in size between the spores allows a tentative genus-level diagnosis, but definitive confirmation depends on laboratory testing using one or more of the techniques listed above.
More on: Microsporidiosis
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
