 ShareCompartir
ShareCompartir

Monthy Case Studies - 2000
Case #46 - October, 2000
A 14-month-old toddler was admitted to a hospital in Jamaica with a high fever and neurological abnormalities of unknown origin. A spinal tap was performed and, based on the results, the child was diagnosed with eosinophilic meningitis (more than 10% of white blood cells were eosinophils). The child died three days after being admitted. A brain biopsy revealed the following structures (Figures A and B). Findings from the epidemiological investigation conducted indicated that the infection was strongly associated with the ingestion of uncooked vegetables where snails or slugs may have been present. What is your diagnosis? Based on what criteria?

Figure A

Figure B
Answer to Case #46
This was a case of angiostrongyliasis, caused by Angiostrongylus cantonensis. Rats are the natural definitive host and pass first-stage larvae (L1) in their feces. When ingested by appropriate molluscan intermediate hosts (snails or slugs), the larvae undergo further development to the infective third-stage larvae (L3). Humans become infected by eating unwashed vegetables that have been contaminated by infected snails, slugs or other paratenic hosts, such as crabs, crayfish, fish, amphibians, or reptiles. Some researchers believe that the L3 larvae can be found in the slime trails of infected snails or slugs.
In human infections, the larvae typically enter the brain and develop into immature adult worms which can result in the clinical syndrome called eosinophilic meningitis. Larval forms of other nematodes (i.e., Baylisascaris and Toxocara) can sometimes be found in the brain, but are much smaller (<50 to 70 micrometers in diameter) and do not have differentiation of the reproductive systems (i.e., uterine tubes or testes).
Diagnostic features can include finding nematodes in brain tissue. The following features may be observed in histological sections:
- a smooth, thin cuticle.
- prominent lateral cords, sometimes dome-shaped.
- a characteristic intestine with few cells, prominent nuclei, and brownish-yellow granules in the cells depending on the stain.
- polymyarian (many muscle cells) and coelomyarain (muscle cells extends well into the body cavity) musculature.
- large size. The worms in the images for this case are immature adults. In Figure A below, you can see the uterine tubes but no eggs or larvae inside them.
We have added arrows to the images to better show some of these key features. It should be noted that although the usual geographical distribution of this parasite is Asia, Australia, islands in the Pacific, and Madagascar, the rat definitive hosts can easily be transported by ship to other areas, and if snails and slugs are present, transmission can occur. We are increasingly aware of angiostrongyliasis being reported in Caribbean countries, and undoubtedly this reflects movement of infected rats to these areas. Figure C below shows adult worms taken from a rat (Rattus rattus) found in the town where this case occurred. The worm on the left is a male and the larger worm on the right is a female where the typical barber-pole-like dark intestine can be seen through the translucent body.
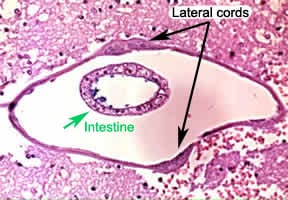
Figure A
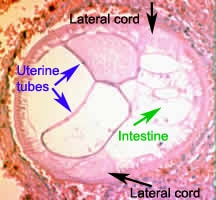
Figure B

Figure C
More on: Angiostrongyliasis
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
