
Worker Killed in Wood-dust Fire Sparked by Faulty Fuse
Oregon Case Report: 13OR021
Release Date: February 9 , 2006
Summary
On August 11, 2003, a 50-year-old production worker was seriously burned, and died 5 days later, from a fire that resulted when wood dust exploded at a wood-flour mill. On the previous day, the worker was shown a makeshift fuse that had been installed in the fuse box. A nonrenewable cartridge fuse had been repaired by taping a renewable fuse element to the outside. The worker pulled out the fuse and inspected it, then replaced it in the fuse box. On the day of the incident, an explosion occurred when the worker started up the machines in the mill for the morning shift. The makeshift fuse generated a spark on startup, which ignited wood dust that had settled in the fuse box. The first explosion raised clouds of dust, which also exploded. At least three explosions in succession carried the fire to the adjacent storage area where the production worker was standing alone. He sustained second- and third-degree burns to his upper body and arms, and breathed toxic, superheated air. When the local fire department arrived, the victim was awake, alert, and oriented. He was transported to a local hospital, and transferred to the Oregon Burn Center for treatment, where he later died.
|
|
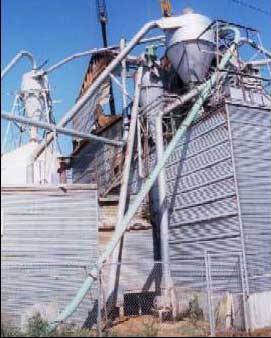
The top of the factory roof was destroyed in the wood-dust explosion.
Photo courtesy of the local fire department. |
Recommendations
- Protection devices for electrical current, such as fuses, should not be altered or bypassed.
- Good housekeeping is critical in wood-products manufacturing to maintain a dust-free environment.
- A safety program is essential at a manufacturing site to ensure employee safety training, hazard identification, and documented inspections.
Introduction
On August 11, 2003, a 50-year-old production worker was seriously burned, and died 5 days later, from a fire that resulted when stored wood flour exploded at a wood-flour mill. OR-FACE was notified of the incident on August 19, 2003. An OR-FACE investigator interviewed the fire department battalion chief and deputy fire marshal in person on August 27, 2003. A registered consulting engineer with a mechanical specialty conducted an investigation for the insurer. Oregon OSHA also investigated the incident. This report is based on materials obtained from fire authorities, plus reports from the insurance investigation, OR-OSHA, and the medical examiner.
The employer is a wood-flour mill that grinds paper-mill waste into a fine powder, and bags and stores it as a marketable product for a variety of industrial applications. The building where the incident occurred was built to older construction standards, and not for the purpose for which it was presently used. A structural modification violated the National Electrical Code (Class II/Div. 1) by exposing the fuse-panel room to combustible dust. In addition, a rubber seal on the fuse box intended to prevent dust from penetrating the box was not in place. Most of the electrical equipment in the factory was old and not up to code, making replacement parts difficult to obtain. The general manager, located in another state, was aware of the antiquated equipment at the mill, but was unaware of applicable safety regulations. The last documented safety inspection at the mill was in 2000.
Three employees worked at the mill, running two shifts at the time of the incident. The employees had worked together at the mill for 9 years. They did not maintain a safety program, or perform safety training or routine inspections to identify hazards related to the building, machinery, or operations. None were trained in applicable safety regulations that apply to wood-flour manufacturing. All three workers made repairs to equipment, including electrical equipment, for which they were not specifically trained or supervised.
One year prior to this incident, a worker was killed in a similar explosion and fire at an adjacent wood-products factory. Dust explosions are a known hazard in wood-products and other organic materials manufacturing that produce dust particles.
Investigation
On the day prior to the incident, the production worker was shown a fuse that had been repaired by a coworker during the previous shift. Apparently, the appropriate replacement fuse was not available (or there was trouble getting it to work properly), and the coworker had taped a renewable fuse link to the outside of the melted, nonrenewable fuse cartridge. The production worker removed the rigged fuse to inspect it, and then reinserted it into the fuse holder.
At 7 a.m. on the following day, the production worker started up the plant operation. Working alone, he began switching on the equipment in a standard start-up sequence. Switches were located in a large storage area adjacent to the fuse-panel room. The rigged fuse was connected to a three-phase 440-volt/30 amp electrical motor for a fan that collected dust emissions from the milling process. The motor was later inspected and found to be fully operational. The rigged fuse had evidently made good contact with the fuse holder earlier, but when removed and reinserted it remained loose enough to allow the renewable fuse link to “chatter” against the ends of the housing, due to vibrations from running equipment in the factory. When the worker hit the switch for the fan, an electric arc was generated across the poor connection between the makeshift fuse and the fuse holder. The wood dust that had accumulated inside the fuse panel ignited and exploded.
The concussion from the initial blast caused wood dust on other surfaces in the area to become airborne, creating a rapid succession of at least three explosions that combined into one very loud, superheated explosion. The required isolation of the fuse-panel room was compromised by a large hole in the wall (1 ft x 3 ft), created during an earlier installation of an I-beam to support the main flour bin. The hole had allowed wood dust to collect on surfaces in the fuse-panel room. When the explosion occurred, the hole also allowed the blast to reach directly where the worker was standing. The upper portion of his body was severely burned, and he inhaled toxic, superheated air.
The production worker walked out of the building to an adjacent business, where he was found by emergency responders. He was awake, alert, and oriented, but had sustained second- and third-degree burns to his upper body and arms. The victim was transported to a local hospital, and transferred to the Oregon Burn Center for treatment, where he died 5 days later.
 |
|
A melted fuse was repaired by taping a renewable fuse link on the outside. |
Cause of Death
Second- and third-degree burns over half of body
Recommendations/Discussion
Recommendation #1: Protection devices for electrical current, such as fuses, should not be altered or bypassed.
The poor contact between the makeshift fuse and the fuse holder was a primary risk in this incident. Fuse holders are designed to ensure tight electrical contact with the fuse end to prevent arcing. The makeshift fuse used in this incident defeated this design. In a renewable fuse, the fuse link is enclosed, and any sparks that might occur are contained. One-time-use fuses must be replaced with a new fuse once expended. A supply of appropriate fuses and circuit-breaker replacements should be maintained for each circuit in a facility.
Recommendation #2: Good housekeeping is critical in wood-products manufacturing to maintain a dust-free environment.
This incident emphasizes the danger of dust as a combustible material with explosive potential. Electrical safety codes explicitly address the hazards of combustible wood flour and other organic dust. In addition to following codes to isolate electrical equipment from dust accumulation, employers should also conduct regular inspections and remove dust with a vacuum.
Recommendation #3: A safety program is essential at a manufacturing site to ensure employee safety training, hazard identification, and documented inspections.
Safety concerns should be adequately addressed before production activities begin and relevant safety codes related to buildings and operations should not be abrogated for production needs. Regularly scheduled safety inspections should be incorporated in the training and ongoing activities of all supervisors and employees. Codes and regulations help to identify and prevent hazards that might otherwise accumulate through aging equipment, inadequate maintenance, and remodeling. A documented program of training, hazard assessment, preventive maintenance, and housekeeping could have helped to prevent this fatal incident. In this instance, only trained employees should repair or modify electrical equipment.
References
- Bean, T.L. (1992). OSHA’s wood dust exposure standard. Ohio State University. Available online: http://ohioline.osu.edu/aex-fact/0595_1.htmlexternal icon
- Gregory Machinery. (n.d.). Dust extraction. Online information resource on health and safety hazards of wood dust, and dust-extraction equipment: http://www.gregmach.com/new_machinery/dust_extraction/important_info.htm (Link updated 04/02/2007 – no longer available 3/26/2013)
- North Carolina Division of Occupational Safety and Health (n.d.). Combustible dust poses a dangerous, explosive threat in the workplace [NCDOL Industry Alert]. Available online: www.nclabor.com/osha/etta/CombDust.pdfpdf iconexternal icon
- Oregon Occupational Safety and Health Division (2003). Put it in writing: The complete guide to OR-OSHA’s written requirements for the workplace [Pub 3300]. Available online: http://www.cbs.state.or.us/external/osha/external icon
Oregon FACE Program
To contact Oregon State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
CROET at OHSU performs OR-FACE investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research. The goal of these evaluations is to prevent fatal work injuries in the future by studying the work environment, the worker, the task, the tools, the fatal energy exchange, and the role of management in controlling how these factors interact.
Oregon FACE reports are for information, research, or occupational injury control only. Safety and health practices may have changed since the investigation was conducted and the report was completed. Persons needing regulatory compliance information should consult the appropriate regulatory agency.
