
Road Paving Crew Member Dies After Being Run Over By A Dump Truck
MinnesotaFACE InvestigationMN9219
January 5, 1993
SUMMARY
A 27-year-old male member of a road paving crew (victim) died of injuries he received as a result of being run over by a dump truck. The victim, a truck driver, was positioned on the outside of his dump truck on the passenger side between the cab and the rear tandem wheels; it is unknown whether he was lying under the truck or whether he was squatting next to the truck. Some tools found next to him after the incident indicate that he may have been attempting to adjust the truck brakes. A roller operator who needed the truck moved in order to continue his tasks entered the truck on the driver’s side. He moved the truck forward approximately 15 feet and, in the process, ran over the victim. MN FACE investigators concluded that, in order to prevent similar occurrences, the following guidelines should be followed:
- use of a lockout-tagout system should be required when vehicles are left unattended or undergoing repair/adjustment; and
- wheels of vehicles undergoing repair or adjustment should be chocked to help prevent unintentional movement of the vehicle.
INTRODUCTION
MN FACE investigators were notified by MN OSHA of a October 14, 1992, road construction fatality occurring on that same day. An employer interview and site investigation were conducted October 15, 1992. Police and coroner reports were requested.
The victim had worked as a truck driver for a paving company employing 24 workers for two seasons, each seven and one-half months long. Safety training for drivers included a written Department of Transportation test and a driver’s test with a trained observer. A safety consultant visited the company once a month and presented general safety and federal and state Department of Transportation compliance lectures to the employees. These visits were usually between one and one-half to two hours long. The company had verbal safety guidelines but no written safety rules or procedures.
INVESTIGATION
A road paving crew was laying blacktop in two lanes of a four-lane residential city roadway. Dump trucks were being used to haul blacktop to a paver which was situated on a north-south bound road. Trucks waiting to dump their load of blacktop were parked on the east-west bound road around the corner from the paver. The victim’s dump truck was parked in the inner lane of this east-west bound road and faced west. A roller approached the truck in this lane from the west. See Figure 1 below.
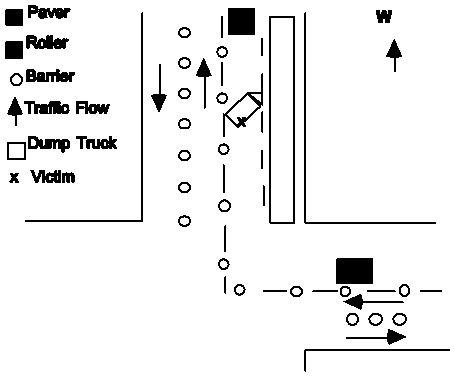
Figure 1.
Tack had been sprayed in the outer lane of the work area, represented by hatching in the diagram. Tack is a sticky liquid spray used between two layers of blacktop for better adhesion. Trucks were able to drive on the tacked area of the road if necessary, but to avoid getting the roller sticky, it could not travel on tacked areas.
While the victim’s truck remained idling, he left the cab to apparently check something underneath it or to adjust its brakes. A hammer and the wrench used for brake adjustment were found near him after the incident. He was positioned between the cab and the rear tandem wheels of the truck on the passenger side.
The roller approaching from the west was unable to pass the truck because it could not proceed in the tacked lane. The operator approached the idling truck on the driver’s side, entered the cab, and released the park brake. He did not see the victim who was located on the passenger side of the truck. He put the truck into gear and drove it forward approximately 15 feet to make enough clearance in the inner lane for the roller to pass. The truck driver was run over and killed in the process.
Another nearby truck driver saw the victim come out from under the moving truck and immediately dialed 911 from his cellular radio. Resuscitative attempts by first responders on site included CPR, but the victim died en route to the emergency room.
CAUSE OF DEATH
The cause of death as listed on the death certificate was multiple traumatic injuries.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Use of a lockout-tagout system should be required when vehicles are left unattended or undergoing repair/adjustment.
Discussion: It was quick and easy for the roller operator to enter and move the truck in this incident. If measures had been taken to make the unintentional movement of the truck difficult this fatality may not have occurred. Turning the engine off and removing the keys would have prevented the roller operator from moving the truck. A tagout indicating that work was being performed on the truck would have warned the roller operator against moving the truck. In addition, a general safe work practice for the entire road crew might be that only “assigned” vehicles are operated by individuals (i.e., workers do not move others rigs).
Recommendation #2: Wheels of vehicles undergoing repair/adjustment should be chocked to help prevent unintentional movement of the vehicle.
Discussion: Chocking the wheels of the truck could have been a visible signal to other workers that work was being performed on it and that it was not to be moved until further approval was granted. In addition, it would have been necessary for the operator to remove the chocking and he would have seen the victim before moving the truck.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.