
Machine Operator Dies After Becoming Caught in a Shirt Pressing Machine – Massachusetts
Case: 02-MA-002-01
Release Date: December 30, 2003
SUMMARY
On February 26, 2002, a 44-year-old female machine operator (the victim) was fatally injured when she became caught in the shirt pressing machine she was operating. The victim reached down into an opening in the loading table, became stuck, and called to a co-employee for help. While the co-employee was attempting to help the victim, the shirt pressing machine cycled, releasing the shirt from the pressing area, crushing the victim’s right arm, right shoulder, neck and chest. Additional co-workers were also unable to free the victim from the machine and a call was then placed for emergency assistance. Personnel from the local and state police and the fire department were notified and responded to the scene within minutes. The Jaws of Life was used to free the victim from the shirt pressing machine and she was rushed to a local hospital were she was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
- ensure that accessible and exposed mechanical hazards of a shirt pressing machine are controlled
- ensure that shirt pressing machines are equipped with emergency stops
- periodically perform equipment hazard analyses to ensure equipment is safe to operate
- train equipment operators and employees on all aspects of the equipment, including functions that don’t pertain to daily operation
- develop, implement, and enforce a comprehensive safety and health program that includes, but is not limited to, hazard recognition, safety training, and protocols to safely complete tasks
In addition, shirt pressing machine manufacturers should:
- design machines so moving parts are not exposed and accessible and emergency stops are linked to the pneumatic system
- explore the possibility of reducing the force used to transfer the buck to and from the loading table and pressing head area
INTRODUCTION
On February 26, 2002, the Massachusetts FACE Program was notified by a local police department through the 24-hour Occupational Fatality Hotline that, on the same day, a 44-year-old female shirt pressing machine operator was fatally injured when she was crushed inside a shirt pressing machine at a dry cleaners. An investigation was immediately initiated. On March 13, 2002 the Massachusetts FACE Program Director and an investigator traveled to the dry cleaner’s location where the victim’s employer was interviewed. The police report, death certificate, corporate information and the Occupational Safety and Health Administration (OSHA) fatality/catastrophe report were reviewed during the course of the investigation.
The employer, a dry cleaner, had been in business for approximately 44 years at the time of the incident. The company employed five people, all of whom had worked at the dry cleaner for at least eight years. The victim had been employed with the dry cleaner for 19 years, and one employee had worked for the dry cleaner for the entire 44 years the company had been in business.
Employee training was primarily on-the-job, except when new equipment was purchased. It was reported by the employer that in 1993, upon delivery of the shirt pressing machine involved in the incident, the manufacturer provided training to the owner and employees on how to operate the machine. The company did not have a safety and health committee, but it has been an active member in a local dry cleaners association where safety was an underlying priority. There was no union representation at this company.
INVESTIGATION
The hours of operation for the dry cleaner were 6:00 a.m. to 6:00 p.m., Monday through Saturday, and closed on Sunday. The victim’s arrival time at work was between 7:00 a.m. and 7:20 a.m. The shirt pressing task was typically performed five hours per day, 7:30 a.m. – 12:30 p.m., and it was estimated that approximately 1,000 shirts were pressed each week.
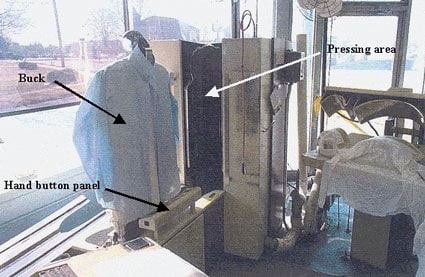
The shirt pressing machine involved in the incident was a cabinet style, with a single buck and vacuum, that had been purchased new in 1993 (Figure 1). The buck is a padded chest and torso section of a mannequin, which shirts are placed when pressed (Figure 1). The vacuum within the buck draws the shirts closely to the buck so that wrinkles will be reduced when pressed. The machine also utilized electrical power and pneumatic and steam pressures. The pneumatic pressure was used to create the vacuum within the buck and to move the buck into the machine pressing area. Steam was used to soften the shirt material so it could be reshaped during the pressing process.
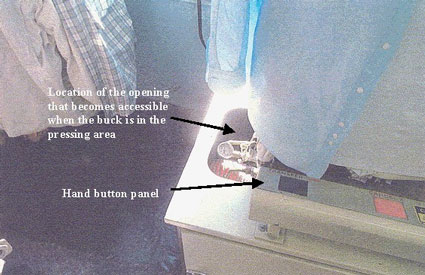
The machine was equipped with an adjustable pressing cycle timer, which could be adjusted to between zero and 99 seconds. The timed cycle starts when the pressing heads close, and ends once the timer reaches zero and the pressing heads open. During the site visit, the employer reported that the cycle of the shirt pressing machine involved in the incident was approximately 45 seconds. According to the manufacturer’s operator manual, the normal pressing cycle setting was 20 seconds, which coincides with the police incident report. When the buck is inside the pressing head area, an exposed opening is left in the loading table that measured approximately 10-inches wide by 48-inches long.
The shirt pressing machine’s power on-off switch was located directly to the right of the operator’s area. The machine also had three hand buttons located on a button panel (Figure 1) and a foot pedal located on the floor of the operator’s station. When depressed, the foot pedal caused the buck sleeve extenders to extend out and closed a vacuum valve. The closed vacuum valve created the suction through the buck’s padding. Two of the three buttons located on the hand button panel were black transfer buttons. Transferring the buck into the pressing head area required the operator to depress and hold down the foot pedal and then depress both transfer hand buttons simultaneously. The machine operator had to keep both transfer hand buttons depressed until the buck transferred into the machine pressing head to complete a cycle. Releasing the foot pedal before simultaneously depressing both transfer hand buttons would end the cycle by causing the sleeve extenders to retract and the vacuum valve to open. If the foot pedal was released after the buck had traveled halfway to the pressing head area, the cycle would continue.
The third hand button on the operator’s button panel was a red cancel button. Depressing the cancel button would cancel the timed pressing cycle or the buck transfer. If the buck was transferring in towards the pressing heads, and the cancel button was depressed, then the buck’s direction would reverse and the buck would return to the start position. If the cancel button was depressed with the buck inside the machine pressing head area and the timing cycle started, then the timer would reset and the pressing heads would open. The shirt pressing machine also contained two vertical safety bars located on either side of the opening for the pressing head area. Depressing either one of the vertical safety bars when the buck was traveling towards the pressing head area would reverse the direction of the buck, returning it to the start position. At the end of the timed cycle, the buck exits the pressing head area and returns to the loading table automatically resetting the shirt pressing machine cycle. If for some reason the buck does not completely return to the loading table, the machine cycle will not reset.
On the day of the incident, the victim arrived to work at 7:20 a.m. Around 11:30 a.m., approximately four hours into the shirt pressing task, a co-worker, who worked next to the victim, heard the victim yell. The co-worker turned around and saw the victim reaching down into the opening in the loading table, which is exposed when the buck is inside the pressing head area. The co-worker went to assist the victim and while attempting to free her, the timed pressing cycle ended and the buck automatically exited the pressing head area and moved towards the loading table. The buck stopped when it struck the victim crushing her right arm, right shoulder, neck and chest against the machine. The co-worker called out to other employees for additional assistance. It was reported that the co-workers tried to free the victim by depressing the machine’s foot pedal and the hand buttons. Because the buck could not fully return to the loading table, the pneumatic pressure was not released, prohibiting the cycle from resetting and the coworkers from being able to manually move the buck.
A call was placed for emergency assistance, and personnel from the local and state police department responded to the scene within minutes. The police unsuccessfully attempted to free the victim by manually pushing the buck towards the pressing head area and then using a crowbar. Then personnel from the fire department responded with the Jaws of Life and freed the victim. The victim was then transported by ambulance, to a local hospital where she was pronounced dead.
It was stated by the employer during the site visit that periodically the victim’s bracelet would come off of her wrist and end up in the exposed loading table opening when the buck was inside the pressing head area. After the incident, the cavity was searched and nothing was found. It was unknown why the victim had reached into the exposed loading table opening. In addition, it was mentioned that when the employer arrived on site after the victim had been transported to the hospital, he opened an air valve, located behind the machine, which released the machine’s pneumatic pressure allowing the buck to be manually moved.
CAUSE OF DEATH
The medical examiner listed the immediate cause of death as acute respiratory arrest due to mechanical asphyxia.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that accessible and exposed mechanical hazards of a shirt pressing machine are controlled.
Discussion: During normal operation of the shirt pressing machine, an opening (10-inches wide by 48-inches long) in the loading table became accessible to employees when the buck was in the pressing head area. This opening in the loading table became a pinch point hazard to employees when the buck returned to its loading table start position covering the opening. In this case, a guard that eliminated employee access to the opening in the loading table when the buck was in the pressing head area would have eliminated the pinch point hazard and prevented the victim from becoming caught in the opening.
Recommendation #2: Employers should ensure that shirt pressing machines are equipped with emergency stops.
Discussion: In this case, if the machine were equipped with an emergency stop that immediately stopped all of the machine functions, including releasing the pneumatic pressure, it would have reduced the victim’s injuries. When considering altering a piece of equipment, such as adding a guard and/or an emergency stop, the equipment manufacturer and/or an engineer should be consulted.
Recommendation #3: Employers should periodically perform equipment hazard analyses to ensure equipment is safe to operate.
Discussion: The shirt pressing machine involved in the incident was manufactured and purchased in 1993 by the company involved in the incident and was operated for many years without incident. Employers might assume equipment that has been functioning without incident for a number of years is “safe” as designed by the manufacturer. Performing a machine specific hazard analysis might reveal potential hazards that have previously been unnoticed.
It is the employer’s responsibility to ensure a safe workplace for their employees. A hazard analysis is a way of focusing on job tasks to identify hazards to which employees might be exposed. Machine specific hazard analyses should be performed on all equipment, both new and older equipment, to identify potential and known hazards. Once uncontrolled hazards are identified, the employer should take steps to eliminate or control these hazards. In this case, a hazard analysis of the shirt pressing machine involved in the incident might have revealed the hazard of the exposed and accessible opening in the loading table, prompting the employer to take steps to control the hazard.
Recommendation #4: Employers should train equipment operators and employees on all aspects of the equipment, including functions that don’t pertain to daily operation.
Discussion: Training provided to employees had been on-the-job and by equipment manufacturers upon delivery of purchased equipment. In this case, training on the shirt pressing machine involved in the incident was last conducted nine years prior to the incident, in 1993, when the machine was delivered.
Employers should provide training, with annual refreshers, to all equipment operators and employees that work in close proximity to the equipment. Training on shirt pressing machines should include proper operation, all safety features and safety hazards of the machine, including the hazard of jewelry or loose fitting clothing potentially becoming caught while operating the machine. The training should also include functions that don’t pertain to daily operations, such as operation of air valves. In this incident, an air valve that was located behind the machine would have released the machine’s pneumatic pressure, allowing the buck to be moved manually. If the co-workers had the knowledge of the air valve’s location and function, the victim’s injuries might have been reduced.
Recommendation #5: Employers should develop, implement, and enforce a comprehensive safety and health program that includes, but is not limited to, hazard recognition, safety training, and protocols to safely complete tasks.
Discussion: A comprehensive safety and health program should be routinely updated with employees’ input, when safety concerns arise and when new equipment and new tasks are introduced into the workplace. When updating a comprehensive health and safety program, employees should participate by evaluating possible hazards associated with equipment and techniques involved in completing their tasks. Employees will know the most about the effectiveness, limitations, and inconveniences of the equipment and procedures to complete tasks. A summary of OSHA’s draft proposed safety and health program rule, which discusses employee training, has been included at the end of this report.
In this case, if the employer had a comprehensive health and safety program, the pinch point hazard of the accessible and exposed opening in the loading table might have been identified and controlled prior to the incident. In addition, to ensure employees are following the protocols that they were trained in, employers should performing periodic scheduled and unscheduled observations of employee performance and work with employees to eliminate any observed unsafe work practices immediately.
Recommendation #6: Shirt pressing machine manufacturers should design machines so moving parts are not exposed and accessible and emergency stops are linked to the pneumatic system.
Discussion: The shirt pressing machine involved in the incident had been designed with multiple safety features to prevent workers from becoming caught between the buck and the machine’s pressing head area. To fully protect workers, a safety feature should have been designed to prevent workers from becoming stuck between the buck and the loading table. A guard designed to cover the exposed and accessible opening in the loading table would have eliminated the pinch point hazard. At the time of the investigation, the employer had been in contact with the machine manufacturer, and they were working on developing additional guarding for the machine.
Shirt pressing machines and similar style equipment should be designed with emergency stops, which override all other switches on the machine. Emergency stops should be located close to the operator. An emergency stop for this machine could be designed to automatically release the pneumatic pressure when the emergency stop switch is engaged by an employee or if a pressure sensor detects resistance during the buck transfer, such as the buck striking an object. Releasing the pneumatic pressure would end the cycle allowing the buck to be moved manually. This type of emergency stop might have reduced the victim’s injuries.
Recommendation #7: Shirt pressing machine manufacturers should explore the possibility of reducing the force used to transfer the buck to and from the loading head and pressing head area.
Discussion: The force needed to transfer the buck into and out of the pressing area should be relatively constant for all shirts being pressed. Therefore, the manufacturer should explore the possibility of altering the transfer cycle to reduce the force used in transferring the buck. Combining a reduction of force used to transfer the buck with an emergency stop that would engage when the buck detects resistance (as described in recommendation # 5), could have reduced injuries in this case.
REFERENCES
- United States Department of Labor, Occupational Safety and Health Administration, Safety and Health Information Bulletins, Cabinet Press Pinch Point Hazard, SHIB 03-07-16 https://www.osha.gov/dts/shib/shib071603.html
- UNIPRESS, Instruction and Parts Manual, CSBV, January 1993
- United States Department of Labor, Occupational Safety and Health Administration, Job Hazard Analysis, Publication Number 3071, Government Printing Office.
- Code of Federal Regulations, 29 CFR 1910.212 Machinery and Machine Guarding, General requirements for all machines, Government Printing Office.
ILLUSTRATIONS
 |
|
Figure 1 – Shirt Pressing Machine
|
 |
|
Figure 2 – Location of the shirt pressing machine opening
|
|
SUMMARY OF OSHA’S DRAFT PROPOSED
SAFETY AND HEALTH PROGRAM RULE FOR EMPLOYERS (29 CFR 1900.1 Docket No. S&H-0027) |
|
Core elements
Basic obligations
Employee participation
Identify and assess hazards to which employees are exposed
Investigate safety and health events in the workplace
|
Safety and health program record keeping
Hazard prevention and control
Information and training
Program evaluation and maintenance
Multi-employer workplaces
|
| Date issued November 23, 1998. Full text available on https://www.osha.gov/dsg/topics/safetyhealth/nshp.html. (Link updated 3/20/2013) | |
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.