
Railcar Worker Dies After Being Crushed by a Reach Stacker Lifting a Wind Tower Section - Colorado
NIOSH In-house FACE Report 2011-01
November 7, 2011
Summary
On October 27, 2010, a 21-year-old worker died after being crushed between the tire of a reach stacker (powered industrial truck) and a railcar. Wind turbine tower sections weighing up to 54 tons each were being loaded onto railcars by the use of two reach stackers, one connected to each end of the tower section by web slings. Four workers were involved in the loading operation: two reach stacker operators and two spotters/riggers. When the incident occurred, one rigger was on the railcar, while the other (the victim) had moved to the ground and was walking between the reach stacker and the railcar. When the rigger on the railcar signaled a reach stacker operator to release the tension on the sling, the operator, unaware of the victim’s location, moved the reach stacker forward, crushing the spotter/rigger against the railcar. The rigger on the railcar saw the incident and immediately signaled for the operator to back away from the railcar. The operator backed away, dismounted his machine, and then attempted to resuscitate the victim. The company emergency response team and city paramedics were called. Emergency personnel arrived within minutes and performed CPR, but were unable to revive the victim. A few minutes later city paramedics arrived at the scene, but were also unable to revive the victim. The victim was pronounced dead at the hospital due to a crushing injury to the upper torso.
Key contributing factors identified in this investigation were unrecognized hazards that include use of a loading procedure that placed workers on foot in areas near operating mobile equipment with limited clearance, use of a loading procedure that required workers to manually disconnect slings from hoisted loads, and nearby equipment that limited the operator’s ability to visually detect the presence of workers on foot.
NIOSH investigators concluded that to help prevent similar occurrences, employers should
- Develop, implement, and enforce a comprehensive safety and health management program that includes hazard analysis, training in hazard recognition, and the avoidance of unsafe conditions.
- Identify and evaluate hazards and develop and implement safe work procedures, engineering controls, and practices to control these hazards.
- Provide worker training that includes hazard recognition and avoidance of unsafe conditions.
- Conduct regular site safety and health inspections to identify new or previously unrecognized hazards, ensure worker adherence to proper procedures, and evaluate the efficacy of hazard controls.
- Employers should consider adding language to contracts that addresses safety and health issues to ensure adequate communication of all tasks between the manufacturing company and the contractor, including the designation of roles and responsibilities, identification of hazards, and establishment of safe work procedures.
- Investigate equipping the mobile equipment, such as reach stackers, with additional visual or sensing devices to enhance the operator’s ability to detect the presence of workers on foot near the machine. This includes technologies such as cameras, radar, and/or sonar to alert the operator to the presence of workers in “blind areas,” as well as tag-based warning systems, which can detect workers wearing tags.
Introduction
On October 27, 2010, a 21-year-old worker died after being crushed between the tire of a reach stacker and a railcar. That same day, compliance safety and health officers from the U. S. Department of Labor, Occupational Safety and Health Administration (OSHA), began an investigation of the incident. On November 3, 2010, the National Institute for Occupational Safety and Health (NIOSH) was notified of the fatal incident by the OSHA Area Office and began its investigation. On December 14, 2010, NIOSH met with OSHA to review the OSHA findings.
On April 6, 2011, a NIOSH investigation team visited the manufacturer’s site and also met with the transportation services company to witness and review railcar loading operations, review procedures, and interview employees. NIOSH also reviewed the actions that both companies had taken to prevent similar incidents.
Employer Description
Employees of two companies were involved in this incident: an international wind turbine manufacturing company and a contract transportation services (railcar) company. The manufacturing company fabricates wind energy towers and ships them in sections, usually by railcar and more recently by truck. At the time of this incident, the manufacturing company had been in operation at this site for less than a year. The facility encompasses nearly 13 million square feet of plant space and 8 miles of on-site railway tracks. The company employs over 450 workers and processes over 220,000 tons of steel per year.
The transportation services company, headquartered out of state, is experienced in loading and transporting wind turbine components that require specialized transport and handling fixtures. The company had been in business for 9 years at the time of the incident. The company employs approximately 50-100 full-time workers at any one time, manages a fleet of more than 500 leased railcars, moves over 10,000 components per year, and is responsible for nearly 3,000 shipments annually. Employees of both companies are non-union.
Written Safety Programs and Training
At the time of the fatal incident, the manufacturing company had a written safety and health program and a full-time on-site health, safety, and environment manager. This program delineated contractor responsibilities, including specific health and safety requirements. The manufacturing company had a forklift trainer, and the two reach stacker operators involved in the incident had received training on the reach stacker; however, they had not received specific training on safe operations when workers on foot are near the machines. The company had developed a general safety orientation for contractors, but neither the victim nor the other spotter/rigger had participated in this orientation. When loading operations began several months earlier at the site, the original transportation services crew received general safety orientation training from the manufacturing company, although reach stacker operations and the use of rigging or slings was not covered. Employees who were interviewed by OSHA and NIOSH reported that morning briefings (conducted by both the manufacturer and the contractor) prior to and on the day of the incident were generally broad and typically did not address specific safety procedures and coordination regarding the task(s) to be conducted.
Representatives of the transportation services company stated that they had a written safety and health program and provided training in accordance with OSHA requirements.
At the time of this incident, the contractor did not have a full-time safety professional, and the lead man/foreman of each project acted as the company’s on-site safety representative.
Victim
The victim was 21 years old and had worked for the transportation services company for 6 months. He normally worked in the contractor’s fabrication shop, was not familiar with loading operations, and had no experience with railcar loading. He had received general safety training but, prior to arriving at the manufacturing facility, had not received any specific safety training, such as rigging or spotting, the use of associated hardware, or working around the mobile equipment. The training was undocumented.
Equipment
Reach stackers (a type of powered industrial truck) are routinely used in sea port and rail loading facilities because of their high stacking capacity and their ability to place loads at further distances from the machine when compared to forklifts. This ability allows for easier hoisting of loads onto railcars (see Figure 1). Reach stackers with the following specifications were used in the loading operations during this incident:
- Engine: 6 cylinder diesel
- Max Lift Capacity: 45,000 kg (49.6 tons)
- Wheels: 18.00 x 25/40 (5½ feet diameter)
The reach stackers involved in the incident were not equipped with an optional rearward TV-camera with a monitor inside the cab or a camera that would indicate blind spots in the front of the vehicle. The reach stackers did not have any other proximity sensing devices or warning systems in place.
Other equipment involved included:
- Railcar
- Wind tower sections weighing from 27 to 54 tons and measuring from 48 ft long x 12 ft diameter to 80 ft long x 7.55 ft diameter each
- Slings/rigging hardware
 |
|
Figure 1. Reach stacker with attachment used to assist in lateral, rotating, tilting, and leveling of the load |
Weather
It was daylight at the time of incident. The temperature was approximately 41ºF, humidity was 31%, and the wind had sustained speeds of up to 29 miles per hour, which is within the manufacturing company guidelines.
Investigation
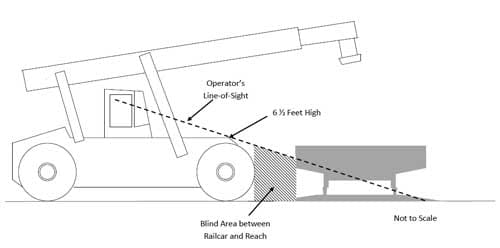
At the time of the incident, the victim was working as a spotter/rigger for loading and securing wind tower sections onto railcars. The wind tower sections vary in size from 80 feet long by 7½ feet in diameter to 48 feet long by 12 feet in diameter. The tower sections vary in weight from 27 to 54 tons. The tower sections were transported to the railcar loading area and hoisted onto the railcar by two reach stackers-one attached to each end of the section by a synthetic web sling. Four workers were involved in the loading operation: two workers from the manufacturing company operated the reach stackers and two workers from the transport services company were spotter/riggers. The spotter/riggers guided the reach stackers by hand signal in hoisting and lowering the section onto the railcar. Once a section had been placed on the railcar, the spotters/riggers would detach the sling on one end, step off the railcar, and walk between the reach stackers and the railcar toward the other end to repeat the process. This was a common practice followed by the contractor’s workers during the loading operation. When this incident occurred, one rigger was still on the railcar while the victim had moved to the ground and was walking toward the other end of the railcar. At this time, the distance between the front of the reach stacker and the railcar was between 3 and 6 feet. Both reach stacker operators and the rigger on the railcar lost visual contact with the victim. The operator could not see the victim from the cab since the front end of the reach stacker is about 6½ feet high and thus created a blind area immediately in front of the machine (see Figure 2). When the rigger on the railcar signaled the reach stacker operator to release the tension on the sling so that it could be removed from the tower section, the operator moved the reach stacker forward, crushing the victim between the reach stacker tire (about 5½ feet in diameter) and the railcar. Immediately, the reach stacker operator saw the rigger on the railcar signal for him to back away from the railcar (see Figure 3).

Based on interviews, manufacturing company employees believed the contractor’s workers were experienced with railcar loading activities and that the procedures being followed were standard industry practices. Morning meetings were held between the manufacturing company and the contractor employees to discuss daily operations. According to employee interviews, these brief meetings consisted of broad safety topics and general cautions such as “be safe” and “watch out” for each other.
The manufacturer had conducted a job hazard analysis of the railcar loading operation 4 months prior to this incident. Hazards, such as suspended loads and equipment blind areas, were considered, and control measures were identified that included cautioning workers to “stay back from suspended loads” and “be aware of surroundings.” Control measures identified for the reach stacker operators included providing operator training to “be aware of blind areas.”
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in the injury or fatality. NIOSH investigators identified the following unrecognized hazards as key contributing factors in this incident:
- Use of a loading procedure that placed workers on foot in areas near operating mobile equipment with limited clearance.
- Use of a loading procedure that required workers to manually disconnect slings from hoisted loads.
- Equipment in areas where the operator’s ability to visually detect the presence of workers on foot near the equipment was limited.a
aBlind area, also referred to as a blind spot is an area around the equipment that is not visible to the operator when stationed at the controls.
Back to Top
Cause of Death
The medical examiner listed the cause of death as crushing injuries to the chest.
Recommendations/Discussion
Note: Corrective actions by employers are highlighted in italics in the discussion section for each recommendation.
Recommendation #1: Employers should develop, implement, and enforce a comprehensive safety and health management program that includes hazard analysis, training in hazard recognition, and the avoidance of unsafe conditions.
Discussion: A comprehensive written occupational safety and health management program should be developed by employers for all workers. The program should include, at a minimum, roles and responsibilities, an explanation of the workers’ rights to protection in the workplace, safe work practices workers are expected to adhere to, emergency procedures, specific safety protection for all tasks performed, ways to identify and avoid hazards, reporting and evaluation of near misses, and who workers should contact when safety and health issues or questions arise.1
Effective safety and health management programs are important in reducing the extent and severity of work-related injuries and illnesses.2 OSHA issued voluntary safety and health program management guidelines in 1989 to encourage employers to do more to protect their employees.3 These guidelines reflect the best management practices of successful companies and encourage employers to institute and maintain a program that provides systematic policies, procedures, and practices that are adequate to recognize and protect their employees from occupational safety and health hazards. The guidelines identify four major elements of an effective program: management commitment and employee involvement, worksite analysis, hazard prevention and controls, and safety and health training. As of the date of this FACE report, OSHA is developing an injury and illness prevention program that follows these principles.4
For a program to be effective, it should meet certain criteria, including:5
- Require positive supervisory safety performance
- Involve middle management
- Have top management visibly showing their commitment
- Have employee participation
- Be flexible
- Be perceived as positive and not punitive
When NIOSH visited the facility in April 2011, the manufacturing company had made significant changes in their safety program, designed to create a positive safety culture following the principles discussed above. The safety program was revamped and made available to all employees and included posting the results of their safety activities, such as, the identification of hazards and their resolution. From top management to floor workers, all employees were now visibly involved with the safety program. Each person’s role was clearly defined and each one was held accountable. Safety teams were reenergized with active employee participation. The transportation services company changed their loading procedure, hired a full-time safety officer, more clearly defined the lines of authority, improved safety inspections and training, and made it clear to all employees that anyone could stop a job if they witness an unsafe practice or condition.
Recommendation #2: Employers should identify and evaluate hazards and develop and implement safe work procedures, engineering controls, and practices to control these hazards.
Discussion: As part of an effective safety and health management program, employers should conduct a worksite hazard survey to identify the potential hazards that workers are exposed to so that appropriate preventive measures for these hazards can be identified and appropriate control measures implemented.
Although a job hazard analysis had been performed by the manufacturing company, the potential for injury to spotters/riggers while walking between the reach stackers and the railcar and under suspended loads may not have been fully appreciated. The control measure identified by the analysis-cautioning workers to stay back from suspended loads and to be aware of surroundings-directly addressed these hazards. However, additional protection could have been provided by other measures, such as revision of the loading procedures to eliminate or minimize the need for workers on foot to be near mobile equipment and the use of sensing technology to alert equipment operators to the presence of workers in “blind areas.”
Once a section had been placed on the railcar, the spotters/riggers would detach the web sling on one end, step off the railcar, and walk between the reach stackers and the railcar toward the other end to repeat the process. This was a common practice followed by the contractor’s workers during the loading operation. OSHA 29 CFR 1910.178 (m)(2) states that no person shall be allowed to stand or pass under the elevated portion of any fork truck or other specialized industrial truck, whether loaded or empty. OSHA 29 CFR 1910.178 (m)(1) states that a fork truck or other specialized industrial truck shall not be driven up to anyone standing in front of a bench or other fixed object.
After the incident the manufacturing company implemented the use of J-hooks instead of slings (see Figure 4 and 5). The use of J-hooks eliminated the need for a spotter/rigger to release the slings from each end of the wind tower section. The spotter/rigger could approach the railcar after the reach stackers had moved away from the railcar, reducing the possibility of injury by eliminating the need to walk under the load or between the reach stacker and the railcar. A new detailed procedure was developed between the manufacturing company and the transportation services company for loading wind tower sections. The new procedure included the following instructions:
- Mandatory radio check before beginning work.
- Designated flagman at each loading/unloading area wearing a yellow vest, while other personnel wear orange vests.
- The reach stacker operator will not move unless he/she can see the designated flagman and has acknowledged a verbal or hand signal communication to make the move.
- The designated flagman directs all movements of the lift equipment.
- When rigging or unrigging a component, the reach stacker operator must place the transmission and parking brake in a condition that is locked against any movement.
- The only movement allowed once the designated flagman signals to lock the reach stacker is movement of the boom and side-shift.
- The reach stacker must stay in this condition until the designated flagman signals that it is okay to unlock and move.
- Communication from the designated flagman must specifically request locked position and the operator must acknowledge.
- Forward or reverse travel can only be directed while the flagman is on the ground.
- No walking under the lift equipment boom when rigged to a component.
- No walking between the reach stacker and any obstruction (for example, railcar, other component, or other lift equipment) unless the space between the two is at least 20 feet and the lift equipment is stationary.
- No walking or standing within 10 feet in front of or behind stationary lift equipment.
- The operator must be able to see designated flagmen at all times.
- No walking within 50 feet of moving lift equipment when in the path of travel.
- Before each new task, all personnel should review the best locations for the designated flagman to position themselves to guide the lift equipment into place.
- The designated flagman should stay to the side of the railcar and a safe distance (a minimum of 10 feet) away from the lift equipment.
- Forklifts and man-baskets will be used to rig both in the yard and on the railcars.
- When loading bulkhead railcars a ladder may be used. When a ladder is used, both workers will be on the railcar, either climbing or holding the ladder. No movement will be permitted by the lift equipment unless both the flagman and rigger are visible and the prescribed locking procedure is observed.
- Any time a new process is required or a new person begins work, a complete briefing of the work tasks including all of these safety procedures must be reviewed.
- All new personnel on the manufacturing company’s property will be required to participate in the manufacturing company’s basic safety orientation.
 |
 |
|
Figures 4 and 5. J-hook now used as part of the new lifting operation |
|
Recommendation #3: Employers should provide worker training that includes hazard recognition and the avoidance of unsafe conditions.
Discussion: An effective occupational safety and health management program includes training to ensure that all employees, including managers, supervisors, and contract workers, understand the hazards to which they may be exposed and how to prevent harm to themselves and others.
Reach stacker operators had received operator training four months prior to the incident, but the training did not specify that spotters/riggers should not to walk between the reach stackers and the railcar. OSHA 29 CFR 1910.178 (l)(4)(ii)(A) states that refresher training in relevant topics shall be provided when the operator has been observed to operate the vehicle in an unsafe manner. It was a common practice for the spotters/riggers to walk between the reach stackers and the railcar.
The victim, who normally worked in the contractor’s fabrication shop, was not familiar with loading operations and had no experience with railcar loading. He had received general safety training, but prior to arriving at the manufacturing facility, had not received specific safety training such as rigging or spotting, the use of associated hardware, or safe procedures for working around the reach stackers. ASME B30.26 (Rigging Hardware) and ASME B30.9 (Slings) both require training in the selection, inspection, cautions to personnel, effects of the environment, and rigging practices for employees using this type of equipment.
Hazard recognition training should be based on an evaluation of the tasks workers will perform for all recognized hazards. These identified hazards and their controls should be incorporated into hazard recognition training. The training should also include specific instructions that workers should not risk physical harm to accomplish tasks. Training in recognizing and avoiding hazards should be provided to all workers, coupled with employer assessments, so that workers are competent in the recognition of hazards and safe work practices.
After the incident, the manufacturing company implemented a systematic process for finding the causes of problems, annual safety awareness training, behavior-based safety (BBS) training, daily tool box briefings, one-on-one dialogues with workers, and implementation of an extensive safety orientation for contractors. The transportation services company provided refresher training for all their supervisors, improved worker training to meet OSHA requirements, and ensured that workers were briefed at the site on the specific procedures they needed to follow.
Recommendation #4: Employers should conduct regular site safety and health inspections to identify new or previously unrecognized hazards, ensure worker adherence to proper safety procedures, and evaluate the efficacy of hazard controls.
Discussion: Regularly scheduled inspections are essential to an effective safety and health program. Close examination of the workplace and review of work practices for adherence to safety policy and procedures can identify unsafe/safe behaviors and emerging hazards before injury can occur. A safety inspection checklist should be used to record the location of all hazards, any necessary corrective action, and the target date for completion by prioritizing the items on the list. Items from previous inspections not yet corrected should be addressed as well.
Regular, frequent, and thorough self-inspections also serve to enhance awareness and identify needs for further training. Employee input in designing checklists and by participating in inspections is also useful and helps establish a strong safety culture.
While the focus of a self-inspection program is usually on identifying and eliminating hazards, it may also be used to identify and correct unsafe behaviors. Behavior-based safety involves the practical application of safety procedures based on the real-world behaviors of employees in work situations.6 A BBS program combines research and intervention and integrates all factors of an organization in an effort to create a safe environment and to improve its safety culture.7
The manufacturing company now involves top management, supervisors, and employees in performing safety walkthroughs and safety inspections and reporting known hazards and near misses. Area supervisors work with workers to resolve issues and ensure that all issues are followed to resolution. The transportation services company is focused on complying with all OSHA required inspections (e.g., crane, forklifts, and rigging), and their top management is remaining onsite for the first two days of each new loading operation and visiting every two months thereafter. The lead person at each project acts as the safety person and conducts daily safety inspections. Their safety officer performs safety audits of all worksites.
Recommendation #5: Employers should consider adding language to contracts that addresses safety and health issues to ensure adequate communication of all tasks between the manufacturing company and the contractor, including the designation of roles and responsibilities, identification of hazards, and establishment of safe work procedures.
Discussion: Morning meetings were held between the manufacturing company and the contractor to discuss daily operations. According to employee interviews, these brief meetings consisted of broad safety topics and general cautions such as “be safe” and “watch out” for each other. Roles and responsibilities for workers were not always clearly designated.
Morning meetings, safety briefings or tool-box talks should be held between the manufacturing company and the contractor to discuss daily operations. Topics that should be covered include the specific hazards of the day’s work activities, how to perform the job safely, the proper use of safety equipment, and communication techniques to be used. Other topics may include a review of past incidents or near misses, any unsafe acts or conditions observed during the past week and how they were corrected, new equipment on the job, or any upcoming job activities.
Roles and responsibilities for workers need to be clearly designated and discussed, including lines of authority and oversight, and who workers should contact regarding hazards. Worker input should be frequently solicited regarding any concerns they may have or safety and health topics that could be discussed.
After the incident, both the manufacturing company and the transportation services company revised their daily morning meetings to include discussion of specific procedures and the hazards and safe practices to follow in detail. Communication, safety equipment to use, and roles and responsibilities are also addressed.
Recommendation #6: Employers should investigate equipping the mobile equipment, such as reach stackers, with additional visual or sensing devices to enhance the operator’s ability to detect the presence of workers on foot near the machine. This includes technologies such as cameras, radar, and/or sonar to alert the operator to the presence of workers in “blind areas,” as well as tag-based warning systems, which can detect workers wearing tags.
Discussion: A variety of vision enhancement and/or object and personnel detection systems are available that can help vehicle and mobile equipment operators detect the presence of people or objects in the equipment’s blind area. Strategically mounted video cameras could provide the operator with a clear view of the blind area around their equipment. Many of these camera systems are currently in use in both construction and non-construction applications. NIOSH has conducted research on a number of these systems.8-11
Currently, many commercial and personal vehicles are equipped with object proximity sensors that sound an alarm and, in some cases, have visual indicators to alert the driver when an object or person is near the vehicle. It is recommended that, when new trucks and equipment are purchased, visual and/or object sensing devices should be purchased as well. These sensing devices can also be installed on older trucks and equipment.
The manufacturing company has installed green lights on each side of the reach stackers that flash when the reach stackers are in a stationary, secure and locked out condition. They are also investigating the use of visual and/or object sensing devices for their reach stackers.
Additional Resources Related To The Industry
OSHA’s Safety and Health Management Systems eTool https://www.osha.gov/SLTC/etools/safetyhealth/index.html
OSHA’s Small Business Handbook, OSHA 2209-02R, 2005 https://www.osha.gov/Publications/smallbusiness/small-business.pdf
OSHA ’s Small Business resources page https://www.osha.gov/dcsp/smallbusiness/index.html
NIOSH’s Small Business Assistance and Outreach Program https://www.cdc.gov/niosh/programs/sbao/
Job Hazard Analysis, OSHA 3071-2002 (revised), 2002pdf iconexternal icon https://www.osha.gov/Publications/osha3071.pdf
NIOSH Alert: Preventing Injuries and Deaths of Workers Who Operate or Work Near Forklifts, NIOSH Publication 2001-109, June 2001 https://www.cdc.gov/niosh/docs/2001-109/
Laborer’s Health & Safety Fund of North America: Internal Traffic Control Plans, OSH-0025E, May 2005 http://www.workzonesafety.org/files/documents/training/fhwa_wz_grant/itcp.pdf
References
- OSHA [2007]. Training standards policy statement.external icon Washington, DC: U.S. Department of Labor, Occupational Safety and Health Administration
[https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=
INTERPRETATIONS&p_id=25658].
- ANSI/AIHA Z10-2005, Occupational Health and Safety Management Systems [2005].
- OSHA [no date]. Voluntary Protection Programexternal icon [https://www.osha.gov/dcsp/vpp/index.html].
- OSHA [2010]. Injury and Illness Prevention Programexternal icon
[https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=
FEDERAL_REGISTER&p_id=21614].
- Petersen D [2001]. Safety management: a human approach, 3rd edition. Des Plaines, IL: American Society of Safety Engineers.
- Geller ES [2004]. Behavior-based safety: a solution to injury prevention: behavior-based safety empowers employees and addresses the dynamics of injury prevention.,J Risk Insur, October [http://findarticles.com/p/articles/mi_m0BJK/is_12_15/ai_n6239831/]. (Link no longer available 4/4/2013)
- Krause TR [1997]. The behavior-based safety process: managing involvement for an injury-free culture, 2nd edition. New York: Van Nostrand Reinhold.
- NIOSH [2007]. Recommendations for evaluating and implementing proximity warning systems on surface mining equipment. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, NIOSH Publication 2007-146 [https://www.cdc.gov/niosh/mining/works/coversheet202.html (Link Updated 10/4/2012)].
- Fosbroke DE [2004]. NIOSH reports studies on heavy equipment blind spots and internal traffic control. Unpublished paper presented at the 2004 Roadway Work Zone Safety & Health Conferencepdf iconexternal icon, Baltimore [http://www.workzonesafety.org/files/documents/news_events/wz_conference_2004/
heavy_equipment.pdf].
- Ruff T [2006]. Evaluation of a radar-based proximity warning system for off-highway dump trucks. Accid Anal Prev 38:92-98.
- Ruff T [2003]. Report of Investigations RI 9660. Evaluation of systems to monitor blind areas behind trucks used in road construction and maintenance: phase 1. By Todd M. Ruff. Cincinnati, OH: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, NIOSH Publication 2003-113.
Investigator Information
The investigation was conducted by Paul Moore, Chief, Fatality Investigations Team, NIOSH Division of Safety Research; Max Kiefer, Director; James Helmkamp, Senior Epidemiologist; and Edgar Reyes, Senior Safety Engineer, NIOSH Western States Office. This report was authored by Edgar Reyes.
Acknowledgement
The NIOSH FACE Program would like to acknowledge assistance from OSHA for providing information for this investigation.
Disclaimer
Mention of any company or product does not constitute endorsement by the National Institute for Occupational Safety and Health (NIOSH). In addition, citations to Web sites external to NIOSH do not constitute NIOSH endorsement of the sponsoring organizations or their programs or products. Furthermore, NIOSH is not responsible for the content of these Web sites.
|
Fatality Assessment and Control Evaluation (FACE) Program The National Institute for Occupational Safety and Health (NIOSH), an institute within the Centers for Disease Control and Prevention (CDC), is the federal agency responsible for conducting research and making recommendations for the prevention of work-related injury and illness. In 1982, NIOSH initiated the Fatality Assessment and Control Evaluation (FACE) Program. FACE examines the circumstances of targeted causes of traumatic occupational fatalities so that safety professionals, researchers, employers, trainers, and workers can learn from these incidents. The primary goal of these investigations is for NIOSH to make recommendations to prevent similar occurrences. These NIOSH investigations are intended to reduce or prevent occupational deaths and are completely separate from the rulemaking, enforcement and inspection activities of any other federal or state agency. Under the FACE program, NIOSH investigators interview persons with knowledge of the incident and review available records to develop a description of the conditions and circumstances leading to the deaths in order to provide a context for the agency’s recommendations. The NIOSH summary of these conditions and circumstances in its reports is not intended as a legal statement of facts. This summary, as well as the conclusions and recommendations made by NIOSH, should not be used for the purpose of litigation or the adjudication of any claim. For further information, visit the program website at www.cdc.gov/niosh/face/ or call toll free at 1-800-CDC-INFO (1-800-232-4643). |