
A 33-Year-Old Textile Worker Dies After Being Pinned by a Bobbin Lift/Dump – North Carolina
NIOSH In-house FACE Report 2000-24
Summary
A 33-year-old textile worker (the victim) died after being pinned between a bobbin lift/dump and a guardrail upright. The victim was operating the bobbin lift/dump in the yarn preparation department of the plant. Empty bobbins were collected in hoppers that were manually pushed up a ramp onto the lift/dump. The lift/dump was then raised and rotated in a counterclockwise direction, dumping the bobbins into a hopper equipped with a belt conveyor that transferred the bobbins to another area of the plant. A guardrail was placed 4 inches in front of the lift dumper. The machine was operated by reaching through the guardrail and pushing the control lever to the left or right to raise or lower the lift/dump. When released, the control lever would return to center. The lift/dump would not move unless the control lever was placed in the raise or lower position. Shortly after 11 p.m., a plant employee walking through the department spotted the victim, who was pinned in a kneeling position between the lift/dump and the guardrail. The employee did not know how to operate the machine but went to the department supervisor to tell him about the victim. A second employee entered the area, spotted the victim, then raised the lift/dump and pulled the victim clear of the machine. The supervisor ran to the victim, then returned to his office and called 911. The Emergency Medical Service (EMS) responded and transported the victim to the hospital where he was pronounced dead.
NIOSH investigators concluded that to help prevent similar incidents, employers should:
- evaluate existing machine guarding to identify potential pinch points and modify guarding to eliminate identified pinch points
- continuously stress the importance of strict adherence to established safe work procedures
- evaluate the practice of allowing workers to work alone in their work areas
Introduction
On July 28, 2000, a 33-year-old textile worker (the victim) died after being pinned between a bobbin lift/dump and a guardrail. On July 31, 2000, officials of the North Carolina Occupational Safety and Health Administration (NCOSHA) notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), of the incident. On August 17, 2000, a DSR safety specialist conducted an investigation of the incident. The incident was reviewed with the NCOSHA compliance officer and city detective assigned to the case and the company’s manager of safety, security, and environment. The incident site was photographed ,and photographs taken immediately after the incident were obtained from the employer.
The employer was a textile mill that manufactured denim fabric and had been in operation since 1905. The mill employed 1,400 workers and normally operated 24 hours a day, seven days a week. The employer had a comprehensive safety and health program and full-time safety director. Documented training was provided on the job. The employer had performed job safety analysis on all tasks performed by workers. Regular safety meetings were conducted in each plant department, and monthly safety meetings were conducted for department heads. All near-miss incidents and incidents requiring first aid were investigated by the plant management committee, who met monthly to review all mill operations. The mill was audited yearly by the corporate safety director. The victim had worked at the mill for approximately 4 months. He had initially been hired as a temporary employee but after 90 days was brought on full time. He had been operating the lift/dump for approximately 3 months.
Back to Top
Investigation
The textile mill had over a million square feet of production area and 343,000 square feet of warehousing. Two million pounds of cotton, which arrived in bales weighing approximately 500 pounds, were processed in the mill on a weekly basis. The cotton fibers were spun into yarn used to produce one million linear yards of the denim fabric per week.
After the bales were opened, equipment picked up the cotton from the bales and transported the stock to cleaning equipment where the cotton fibers were blended and opened, allowing the removal of trash and short fibers. The fibers were then further cleaned, blended, straightened, and condensed into a rope-yarn form. The yarn was wound tightly onto fiberboard bobbins that were 1 foot long and 1½ inches in diameter. The bobbins of yarn were then wound onto larger packages of yarn needed for weaving the fabric. The empty bobbins were loaded into hoppers and manually pushed up a ramp onto the bobbin lift/dump. The lift/dump was raised and rotated in a counterclockwise direction, dumping the empty bobbins into a hopper equipped with a belt conveyor that transferred the bobbins onto a roller conveyor which transported them back to the start of the process to be rewound with yarn.
|
|
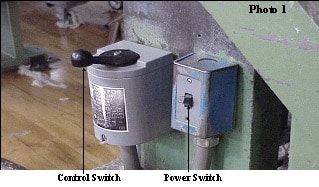
Photo 1. Control lever used to operate the machine.
|
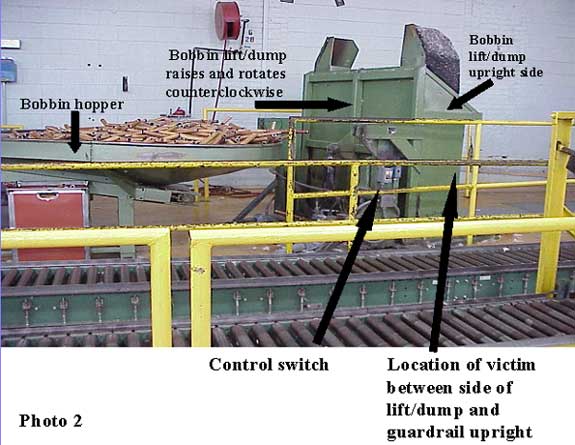
On the day of the incident the victim was working the 6 p.m.-to-6 a.m. shift operating the lift/dump in the yarn preparation department of the plant. A guardrail was placed 4 inches in front of the lift dump as a barrier between the machine operator and the moving parts of the machine. The machine was operated by reaching through the guardrail and pushing the control lever to the left or right to raise or lower the lift/dump (Photo 1). When released, the control lever would return to center; however, the lift/dump would not move unless the control lever was placed in the raise or lower position. At 11 p.m., the three other workers in the department went on break. The victim was scheduled for his break at midnight. Shortly after 11 p.m., a plant employee walking through the department spotted the victim in a kneeling position facing the guardrail and pinned between the side of the lift/dump and the guardrail upright (Photo 2). The employee did not know how to operate the machine but went to the department supervisor to report the incident. A second employee entered the area, spotted the victim, raised the lift/dump to free the victim, and pulled him clear of the machine. The supervisor called the security guard at the front gate, who was an emergency medical technician (EMT), and instructed him to proceed to the department. The security guard contacted a second guard in the plant and told him to also proceed to the area. The supervisor went to the victim, then returned to his office and called 911. The security guard from the front gate arrived at the victim first and detected a faint pulse and shallow breathing. When the victim stopped breathing and a pulse could no longer be detected, the EMT initiated cardiopulmonary resuscitation (CPR) and continued it until the Emergency Medical Service (EMS) responded. EMS personnel transported the victim to the hospital where he was pronounced dead.
It could not be determined why the victim was in the position in which he was found. An investigation by OSHA and the plant management committee could not determine why the victim had placed himself between the guardrail and the machine. The lift/dump had dumped the hopper of bobbins into the bobbin hopper and was being lowered when it pinned the victim between the side of the lift/dump and the guardrail upright. When tested, the machine functioned properly. The lift/dump would only raise or lower when the control lever was maneuvered to the respective positions.
Additionally, a 36-inch long metal rod with a hooked end was present at the machine to be used to rake any bobbins out from under the machine or out of the dumper. There were no bobbins present on the floor in the area where the victim was found.
|
|
Photo 2. Location of lift/dump and guardrail upright where the victim was pinned.
|
Back to Top
Cause of Death
The attending physician listed the cause of death as asphyxiation due to compression of the chest.
Recommendations and Discussion
Recommendation #1: Employers should evaluate existing machine guarding to identify potential pinch points and modify guarding to eliminate any identified pinch points.
Discussion: The machine involved in this incident was guarded in front to provide a barrier between the moving parts of the machine and the machine operator; however, a potential pinch point existed between the guardrail and the side of the lift/dump. When the victim placed himself between the guardrail and the side of the machine and lowered the dumper, he was pinned between the two surfaces.
Employers should evaluate machine guarding to determine if any potential pinch points are created by the guarding, then modify the guarding to eliminate any pinch points. Machine manufacturers can be contacted to determine if retrofit guarding may have been developed for their products. Since the incident, the employer has made modifications to the machine. A shatterproof plexiglas barrier was mounted directly to the front of the machine. The controls could be accessed by a cutout in the plexiglas. This eliminated any space between the machine and the barrier. The control switch was changed from a one-handed control to a control that required the use of two hands for operation. Additionally, the work station was redesigned to allow the operator more room around the perimeter of the machine.
Recommendation #2: Employers should continuously stress the importance of strict adherence to established safe work procedures.
Discussion: Documentation showed that the victim had received training in the safe operation of the machine. Safe work procedures required that machine operators contact maintenance if they encountered problems with the machine they were operating. Maintenance records indicated that the victim had adhered to these procedures in the past. As previously stated, it could not be determined why the victim placed himself in the position he was in. Employers should continuously stress the importance of strict adherence to established safe work procedures and should monitor employees to determine adherence to these procedures.
Recommendation #3: Employers should evaluate the practice of allowing workers to work alone in their designated areas.
Discussion: The other employees in the department had gone on break and the victim was working alone in his designated area when he became pinned by the machine and was unable to free himself. Employers should evaluate a policy requiring multiple employees to be present in any area where potential hazards might exist. These employees should remain in constant visual or verbal contact with each other. Breaks could be scheduled in such a manner as to allow this. This would allow employees to provide assistance to each other should a problem arise and would provide workers the opportunity to ensure their coworkers are adhering to safe operating procedures at all times.