Healthy People 2000 Progress Review
Educational and Community-based Programs
Date: November 3, 1999
Time: 2-4:30 p.m. EST
This progress review will be broadcasted from Food and Drug Administration (FDA), Gaithersburg, Maryland. Details on how to review the broadcast are provided on the Public Health Training Network home page.
Dr. David Satcher, Assistant Secretary for Health and Surgeon General, will be joined by a panel of experts representing the public and private health sectors. Claude Earl Fox, M.D., Administrator of Health Resources and Services Administration (HRSA); Kathy Cahill, M.P.H., Associate Director for Policy, Planning and Evaluation, CDC, and Dr. Edward Sondik, Director of the National Center for Health Statistics, Centers for Disease Control and Prevention (CDC), will review the progress towards the targets for the objectives in the Educational and Community-based Programs area of Healthy People 2000. Participants, listed in the agenda will then engage in a discussion that covers four educational and community-based settings: school, worksite, healthcare, and community.
Program Objectives
- Assess progress made in achieving the Healthy People objectives for Educational and Community-Based Programs (ECBP).
- Highlight effective programs that had an impact on progress, and understand barriers that have hindered improvement.
- Gain an understanding of the Healthy People 2010 ECBP objectives for schools, worksites, healthcare sites, and the community-at-large.
- Participate with Dr. Satcher and leaders from government and the private sector in discussing how the 2010 objectives can be translated into opportunities for action.
Briefing Book Materials
Data Section
Presentation
Edward J. Sondik, PH.D.
Director, National Center for Health Statistics
Thank you Dr. Satcher. Good afternoon. Today we’re reviewing the progress in our efforts to educate children and adults in healthy living, through the schools, the work place, the community, and in the family. In most of the previous Healthy People reviews, we measured the outcome of actions taken to improve the public’s health and prevent disease. For this review we’re looking more closely at the progress in building the structure and process necessary to take action. There is some good news to report, particularly in the growth of health education programs at worksites, where we all spend so much time. But for aspects of this topic, progress–or lack of it–has been hard to document. While a few objectives are tracked annually, most have less frequent data collection, which can change in scope or definition. Yet with these limitations, some clear patterns emerge.
Let’s begin with education…
Head Start gives pre-school children a “head start” in many aspects of life, but throughout the 1990’s, enrollment has dropped. The percent of low-income children entering kindergarten or first grade who received Head Start services decreased from 58% in 1992 to 49% in 1996. On the other hand, enrollment in preschool of children with disabilities has increased, as efforts to mainstream children with disabilities and refit schools to meet their needs has increased.
Head Start eligibility is based on Federal poverty guidelines. As shown in this slide, the proportion of children under the age of 6 has declined since 1994. This means there are now fewer children eligible for Head Start.
Now at the other end of the education spectrum, high school completion has shown virtually no improvement over the decade and remains below the target. Except for a slight increase among Hispanic youth, high school completion rates were stable between 1992 and 1997. Rates remain considerably lower for Hispanic students and somewhat lower for black students than the overall average. This is a serious deficiency when education has been shown to be highly correlated with poorer health outcomes.
CDC has identified 8 specific elements, which must be present to constitute comprehensive school health education. These elements include trained health teachers, a designated coordinator, and coverage of key behavioral areas. Data show that three out of four schools have at least one required health class and two out of three schools have evaluated their health education program in the past 2 years. But less than a third report the involvement of parents, health officials, and other concerned community members in school health education programs. Only 2 percent of schools meet all 8 of the CDC criteria for a comprehensive school health education.
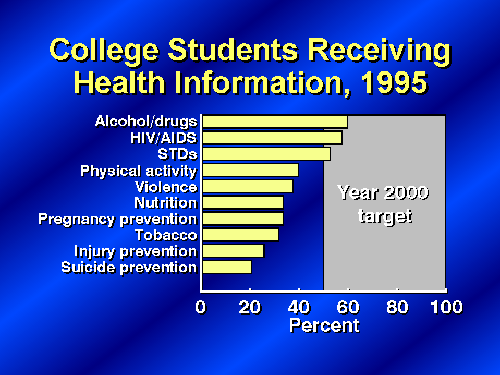
Now, at the college level, health education is also less than comprehensive. Data from 1995 indicate that a majority of students are receiving information at some time during their college career on health topics such as alcohol and drug use and STD prevention, including HIV–which, on the positive side, exceeded the targets established for these topics. But far fewer are receiving information on topics ranging from physical activity and fitness to violence and injury prevention–knowledge which can promote a longer, healthier life.
But education and information do not always translate directly or immediately to behavioral change. For example, there has been very little change in the past decade in binge drinking by college students, even though most students have been informed about the dangers of alcohol abuse. Binge drinking is defined as 5 or more drinks on one occasion in the past 2 weeks. This example illustrates the complex relationship between educational programs and behavioral change.

To further illustrate that point, in an earlier slide we saw that only about 20 percent of college students received information on suicide prevention. Yet, suicide rates in college-aged youth have been declining since the mid 1990’s. From 1994 to 1998, suicide rates for those 15-24 years old have dropped by 22 percent. This drop parallels a nationwide trend of decreasing rates of firearm deaths.
Not only is health promotion important in our schools, but for real progress to be made, health promotion must be a force on the job and in the community. Research has shown that the doctor’s office, local health facilities, and programs offered through the local health departments play key roles in educating the public about health promotion and disease prevention.
And there has been solid gains in worksite health promotion. People working for large companies have found more worksite health promotion activities in place. In fact, the proportion of worksites with 50 or more employees that offer health promotion programs has increased almost 40 percent since 1985.
For community-based programs to succeed, they must match or reflect the characteristics of the community. The data show that a substantial number of local health departments are providing culturally and linguistically appropriate programs for selected preventive services. Data also indicate that programs in immunization and infectious disease, maternal and infant health, and STD’s including HIV are most likely to be delivered in ways sensitive to the culture and language of minority populations served by local health departments. Additional data we have on the NCHS web site show the extent to which local health departments have programs in these four areas.
As we see on this slide, there are fewer culturally and linguistically appropriate programs for these several topics, including injuries and mental health. In Healthy People 2010 we have both an opportunity and a critical need to improve in this area of educational and community-based programs. As our population grows more diverse it will be even more essential to ensure that there are a range of programs which can effectively reach and speak to various groups in our society.
A substantial proportion of hospitals and HMO’s provided health promotion programs at the community level. We’ve all seen some examples of these programs, for example relating to diabetes or hypertension prevention and control. This is an important aspect of health in the community, but one where we lack up-date data. We do have current data for a related objective in this area–the proportion of older Americans participating in organized health promotion activities. Preliminary data for 1998 indicate that the level of participation has not improved from the 12 percent recorded earlier in the decade.
The new Healthy People 2010 objectives call for improved tracking of community-based programs. The Association of State and Territorial Directors of Health Promotion and Public Education is currently developing a survey that will provide useful baseline information.
Finally, the family is clearly at the center of learning experiences. It’s the place where most of us choose our behaviors and shape our values. But the family is often overlooked as a source of health promotion information. Families with children 10 years or older are somewhat less likely today than just a few years ago to discuss health issues. The latest preliminary data for 1998 do show an increase in family discussions in the areas of alcohol and drugs, but there’s also been a substantial drop in discussions of nutrition and physical activity–just at the time we’ve seen overweight prevalence increase and physical activity decline for children and adults.
I mentioned data challenges in the beginning of this presentation–the lack of current, comprehensive, and comparable data in many important areas. A lack of data at the state and local levels are even more problematic. In Healthy People 2010 this problem is well recognized. The challenge of developing appropriate, timely data at the national through the community level are all addressed. Several objectives have been constructed to stimulate data collection, in more areas and with greater frequency. We know that we can improve only if we know where deficiencies exist and progress has lagged. Education and community based programs offer a critical opportunity for promoting health and presenting disease, but only if we fully understand the present can we fully utilize its potential. Thank you. Dr. Satcher.
- Office of Disease Prevention and Health Promotion
- Healthy People 2000 Web Page
- National Center for Chronic Disease Prevention and Health Promotion
- Youth Risk Behavior Survey
- Behavioral Risk Factor Surveillance System
- Directors of Health Promotion and Education
- Society for Public Health Education
- Department of Education National Center for Education Statistics
- National Association of County and City Health Officials