Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Recommendations for Postexposure Interventions to
Prevent Infection with Hepatitis B Virus, Hepatitis C Virus, or
Human Immunodeficiency Virus, and Tetanus in Persons Wounded
During Bombings and Other Mass-Casualty Events --- United States, 2008
Recommendations of the Centers for Disease Control and Prevention (CDC)
Prepared by
Louisa E. Chapman, MD1
Ernest E. Sullivent, MD2
Lisa A. Grohskopf, MD3
Elise M. Beltrami, MD4
Joseph F. Perz, DrPH5
Katrina Kretsinger, MD6
Adelisa L. Panlilio, MD4
Nicola D. Thompson, PhD5
Richard L. Ehrenberg, MD7
Kathleen F. Gensheimer, MD8,9
Jeffrey S. Duchin, MD10,11
Peter H. Kilmarx, MD3
Richard C. Hunt, MD2
1Immunization Services Division, National Center for Immunizations and Respiratory Diseases,
2Division of Injury Response, National Center for Injury Prevention and Control
3Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
4Division of Healthcare Quality Promotion, National Center for Preparedness, Detection, and Control of Infectious Diseases
5Division of Viral Hepatitis, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
6Division of Bacterial Diseases, National Center for Immunizations and Respiratory Diseases
7Office of Emergency Preparedness and Response, National Institute for Occupational Safety and Health
8Council of State and Territorial Epidemiologists, Atlanta, Georgia
9Maine Department of Health and Human Services, Augusta, Maine
10National Association of County and City Health Officials, Washington, DC
11Public Health -- King County, Seattle, Washington
The material in this report originated in the Coordinating Office for Terrorism Preparedness and Emergency Response, Rich Besser, MD, Director;
the National Center for Immunizations and Respiratory Diseases, Anne Schuchat, MD, Director; the National Center for HIV/AIDS, Viral Hepatitis,
STD and TB Prevention, Kevin A. Fenton, MD, PhD, Director; the National Center for Preparedness, Detection, and Control of Infectious Diseases,
Rima Khabbaz, MD, Director; the National Center for Injury Prevention and Control, Howard Frumkin, MD, Director, Division of Injury Response,
Richard Hunt, MD, Director; and the National Institute for Occupational Safety and Health, John Howard, MD, Director.
Corresponding preparer: Louisa Chapman, MD, National Center for Immunizations and Respiratory Diseases, CDC, Mailstop D-68, 1600 Clifton
Road, N.E., Atlanta, GA 30333. Telephone: 404-639-8921; Fax: 404-639-3500; E-mail: LChapman@cdc.gov.
Summary
This report outlines recommendations for postexposure interventions to prevent infection with hepatitis B virus,
hepatitis C virus, or human immunodeficiency virus, and tetanus in persons wounded during bombings or other events resulting
in mass casualties. Persons wounded during such events or in conjunction with the resulting emergency response might
be exposed to blood, body fluids, or tissue from other injured persons and thus be at risk for bloodborne infections. This
report adapts existing general recommendations on the use of immunization and postexposure prophylaxis for tetanus and
for occupational and nonoccupational exposures to bloodborne pathogens to the specific situation of a mass-casualty
event. Decisions regarding the implementation of prophylaxis are complex, and drawing parallels from existing guidelines
is difficult. For any prophylactic intervention to be implemented effectively, guidance must be simple, straightforward,
and logistically undemanding. Critical review during development of this guidance was provided by representatives of
the National Association of County and City Health Officials, the Council of State and Territorial Epidemiologists,
and representatives of the acute injury care, trauma and emergency response medical communities participating in
CDC's Terrorism Injuries: Information, Dissemination and Exchange (TIIDE) project. The recommendations contained in
this
report represent the consensus of U.S. federal public health officials and reflect the experience and input of public
health officials at all levels of government and the acute injury response community.
Introduction
Public health authorities must consider how to provide care to injured persons in the event of acts such as
bombings that result in mass casualties. During 1980--2005, of 318 acts of terrorism investigated by the Federal Bureau
of Investigation (FBI) in the United States or territories, 208 (65%) involved attempted bombings; of these 208
attempts, 183 (88%) succeeded. The majority of these acts were committed by domestic extremist groups that
intentionally targeted property and did not cause deaths or
injuries in persons; however, 19 bombings (10% of those that
were successful) resulted in 181 deaths and 1,967 injured
survivors. These figures do not include mass-casualty
incidents that occurred outside the United States and its territories or those that occurred on U.S. soil that were classified as
crimes, accidents, unintended negligence, or terrorist incidents other than bombings (e.g., the 2,972 persons killed as a result
of the terrorist attacks of September 11, 2001). A total of 1,967 (91%) persons
injured during terrorist bombings in the United States and approximately 12,000 (80%) persons injured during the terrorist attacks of September 11,
2001, survived (1).
Military health-care providers frequently must respond to mass-casualty events. During October 7,
2001--March 1, 2008, of 35,630 casualties incurred by U.S. Department of Defense forces involved in Operation Enduring
Freedom (OEF) in Afghanistan and Operation Iraqi Freedom in Iraq (OIF),
27,441(77%) resulted from mass-casualty
events. Explosive devices accounted for 23,277 (65%) of these
casualties. Of 27,441 persons wounded during OEF- and
OIF-related mass-casualty events, 24,433 (89%) survived (U.S. Department of Defense, unpublished data, 2008).
In August 2001, the Israeli health ministry announced that tissue from two suicide bombers had tested positive
for evidence of hepatitis B virus (HBV) (2). A 2002 case report from Israel described evidence of hepatitis B virus in a
bone fragment that had traumatically implanted into a bombing survivor
(3). Traumatically implanted bone fragments removed from five survivors of the 2005 London bombings were taken directly to forensic custody without testing
for bloodborne pathogens (4) These observations support the potential for explosions to result in transmission of
infections among persons injured during the event and indicate that emergency responders and health-care providers in the
United States need uniform guidance on prophylactic interventions appropriate for persons injured in bombings and
other events resulting in mass casualties. Wounds resulting from mass-casualty events require the same considerations
for management as similar injuries resulting from trauma cases not involving mass casualties, including the risk for
tetanus. In addition, exposure of wounds, abraded skin, or mucous membranes to blood, body fluids, or tissue from
other injured persons (including suicide bombers and bombing casualties) might carry a risk for infection with a
bloodborne virus. Injured survivors of mass-casualty events are at risk for infection with HBV, hepatitis C virus (HCV), or
human immunodeficiency virus (HIV) and for tetanus.
Decisions regarding the administration of prophylaxis after a mass-casualty event are complex, and drawing
direct parallels from existing guidelines regarding prophylaxis against bloodborne pathogens in occupational
or nonoccupational settings is difficult. Assessment of risk factors commonly used to estimate the need for
prophylactic intervention might not be possible in the setting of response to a mass-casualty event because responses to such
events might overwhelm local emergency response facilities, and medical response staff will be focused primarily on
rendering lifesaving trauma treatments. Because no uniform guidance existed for posstexposure interventions to prevent
bloodborne infections and tetanus among U.S. civilians or military personnel wounded during mass-casualty event, CDC convened
a Working Group comprising experts in injury response, immunizations, bloodborne infections, tetanus, and
federal-, state-, and local-level public health response to develop such guidance.
The recommendations in this report pertain only to bombings and other mass-casualty events and are not meant
to supplant existing recommendations for other settings. In a situation involving a substantial number of casualties,
the ability to assess medical and vaccination histories or the risks associated with the source of exposures might be limited,
as might the supply of biologics. For this reason, in certain instances, the recommendations provided in this report
differ from standard published recommendations for vaccination and prophylaxis in other settings. These recommendations
are not meant to supplant existing recommendations for other settings and apply only to the specific situation of an
event
involving mass casualties. In addition, the recommendations provided in this report are limited to issues regarding
initial postexposure management for bloodborne pathogens and tetanus prophylaxis. Other prophylactic measures that
might be appropriate (e.g., use of antibiotics for the prevention of bacterial infection) are not discussed in this report.
Federal law requires the use of a Vaccine Information Statement (VIS) before the administration of vaccines
against HBV or tetanus. VIS forms are available at
http://www.cdc.gov/vaccines/pubs/vis/default.htm. Whenever feasible, a
VIS form should be provided to patients or guardians before vaccination.
Individual states set forth their own legal requirements as to what constitutes the nature of informed consent
that might be required before certain medical interventions. In general, these statutes also provide for exemptions
in emergency circumstances. It is these state-specific laws that should guide response when informed consent would
be applicable, but the circumstances of response to a mass-casualty event might preclude adherence to
standard informed consent processes. Emergency responders and health-care providers should consult with their legal counsel
for guidance regarding the relevant laws of their jurisdictions in advance of any mass-casualty event.
Methods
This report was developed through consultation among persons with expertise in immunization and
other prophylactic interventions against bloodborne and other infections, physicians who specialize in acute
injury-care medicine (trauma and emergency medicine), and local, state, and federal public health epidemiologists. Thus,
the recommendations in this report represent the best consensus judgment of expert opinion.
This report adapts existing recommendations on the use of immunization and postexposure prophylaxis in response
to occupational and nonoccupational exposures to bloodborne pathogens in the United States to the specific
mass-casualty event setting while acknowledging the difficulty of drawing direct parallels. This adaptation also draws on guidance
and practices developed previously and in use in the United Kingdom and Israel
(2,5--7).
These recommendations were adopted through a process of expert consultation and consensus development.
First, CDC drafted proposed preliminary recommendations on the basis of relevant existing U.S. guidance and practices
of Israel and the United Kingdom (2,5--7). These proposed recommendations were discussed by representatives of the
U.S. and international trauma response community at a May 2006 meeting in Atlanta, Georgia; following this
discussion, the initial draft was revised. A working group then was convened comprising CDC staff members with expertise
in injury response, tetanus, viral hepatitis, HIV infection, immunization and postexposure prophylaxis, and
occupational safety and health, and representatives of the National Association of County and City Health Officials and the
Council of State and Territorial Epidemiologists with experience in local and state level public health response. This
group worked through the draft section by section to revise, update, and refine the recommendations; this revised
document was shared again with representatives of the U.S. and international trauma response community for additional
comment during a meeting in Atlanta, Georgia, in August 2007. Because this guidance met the requirements established by
the Office of Management and Budget (OMB) for a Highly Influential Scientific Assessment (HISA) (available at
http://www.whitehouse.gov/omb/memoranda/fy2005/m05-03.html), the recommendations underwent a final process
of external review in addition to undergoing internal CDC review for scientific content. As part of the OMB HISA
peer review, the document was posted on CDC's website for public comment. An external expert panel subsequently
reviewed and critiqued the document, the public comments, and CDC's response to those comments, and the document
was revised a final time in response to the external review
process.
Bloodborne Pathogens of Immediate Concern
Although transfusions and injuries from sharp objects (e.g., needlestick) have been associated with the transmission
of multiple different pathogens (8,9), three bloodborne pathogens merit specific consideration in mass-casualty
situations: HBV, HCV, and HIV. All three viruses are endemic at low levels in the United States and can be transmitted by
exposure of infectious blood to an open wound or, more rarely, to skin abrasions or through exposure to
intact mucous membranes. These viruses also can be transmitted by similar exposures to other body fluids or tissues
from infected persons. Infection risks and options for postexposure prophylaxis vary, depending on the virus and the type
of
injury and exposure. Because hepatitis A virus (HAV) is transmitted via the fecal-oral route and is not considered
a bloodborne pathogen (10), HAV prophylaxis is not recommended during a mass-casualty event.
The information typically used in occupational settings to guide prophylactic intervention decisions (including
the circumstances of the injury, background prevalence of disease, or risk for infection of the source of exposure) might
not be as clearly interpretable or as readily available in a mass-casualty setting. For example, both the extent
of exposed disrupted skin and the volume of blood contributing to the exposure might greatly exceed that of
usual occupational exposures. In addition, injured persons might be exposed to blood from multiple other persons or
to biologic material from the body of a bomber or another
injured person. The HBV, HCV, and HIV status of the
source(s) usually will be unknown, and timely ascertainment might not be practical. If the circumstance in which each victim
was injured can be characterized, this information can be used to assess the likelihood that an injured person was exposed
to another person's blood. However, when such information is not readily available for persons injured during
blast-related mass-casualty events, such blood exposure should be assumed.
Hepatitis B Virus
The prevalence of chronic HBV infection in the United States is approximately 0.4%. Prevalence varies by
race, ethnicity, age group, geographic location, and individual history of risk behaviors
(11).
Newly acquired HBV infection often is asymptomatic; only 30%--50% of children aged >5 years and adults
have initial clinical signs or symptoms (11). The fatality rate among persons with reported cases of acute
symptomatic hepatitis B is 0.5%--1.0% (11). No specific treatment
exists for acute hepatitis B. Acute hepatitis B infection fails
to resolve and instead progresses to chronic HBV infection in approximately 90% of those infected as infants, 30%
of children infected at age <5 years, and <5% of persons
infected at age >5 years (11). Overall, approximately 25%
of persons who become chronically infected during childhood and 15% of those who become chronically infected
after childhood die prematurely from cirrhosis or liver cancer
(11). Therapeutic agents approved by the U.S. Food and
Drug Administration (FDA) for treating chronic hepatitis B can achieve sustained suppression of HBV replication
and remission of liver disease for certain persons
(11).
HBV is transmitted by percutaneous or mucosal exposure to infectious blood or body fluids. Although hepatitis
B surface antigen (HBsAg) has been detected in multiple body fluids, only serum, semen, and saliva have
been demonstrated to be infectious (11). Serum has the highest concentration of HBV, with lower concentrations in
semen and saliva. HBV remains viable for 7 days or longer on environmental surfaces at room temperature
(11). Among susceptible health-care personnel, the risk for HBV infection after a needlestick injury involving an HBV-positive
source is 23%--62% (12). Prompt and appropriate postexposure prophylaxis (PEP) intervention reduces this risk.
Many infections that occurred before widespread vaccination of health-care personnel probably resulted from
unapparent exposures (e.g., inoculation into cutaneous scratches,
lesions, or mucosal surfaces) (12).
Both passive-active PEP with hepatitis B immune globulin (HBIG) combined with hepatitis B vaccine and active
PEP with hepatitis B vaccine alone have been demonstrated to be highly effective in preventing transmission after
exposure to HBV (12). HBIG alone has been demonstrated to be effective in preventing HBV transmission. However, since
hepatitis B vaccine became available, HBIG is used typically (and preferentially) as an adjunct to vaccination
(11). The major determinant of effectiveness of PEP is early administration of the initial dose of vaccine (or HBIG). The effectiveness
of PEP diminishes the longer after exposure it is initiated
(12). Studies are limited on the maximum interval after
exposure during which PEP is effective, but the interval is unlikely to exceed 7 days for perinatal and needlestick exposures
(12). No data are available on the efficacy of HBsAg-containing combination vaccines when used to complete the
vaccine series for PEP, but the efficacy of combination vaccines is expected to be similar to that of single-antigen vaccines
because the HBsAg component induces a comparable antibody response
(12). Antiviral PEP is not available for HBV.
A policy of liberal use of hepatitis B vaccine for PEP after bombings or in other mass-casualty situations
is recommended because of the high concentration of HBV in blood of infected persons, the durability of HBV in
the environment, and the efficacy and relative ease of administration of vaccine
(11). Such use is consistent with existing recommendations for administering the hepatitis B vaccine series as PEP for persons (e.g., health-care personnel or
sexual assault victims) exposed to a source with unknown HBV infection status
(11,12). In general, PEP for HBV will be warranted for previously unvaccinated persons if wounds, nonintact skin, or intact mucous membranes might have
been
exposed to blood or body fluids from another person or persons. In a mass-casualty setting, failure to provide hepatitis
B vaccination when needed could result in preventable illness, whereas unnecessary vaccination is unlikely to cause
harm (11). Completion of primary vaccination at the time of discharge or during follow-up visits should be ensured for
all persons who receive an initial hepatitis B vaccine dose as part of the acute response to a
mass-casualty event.
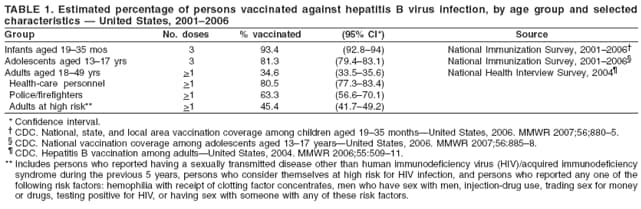
If hepatitis B vaccine is in short supply, assessing how likely a person is to have been vaccinated previously might
be necessary. In general, hepatitis B vaccination rates are highest among children aged <17 years (80%--90%) and
health-care personnel (approximately 80%) (Table 1)
(13--15) (see Pathogen-Specific Management Recommendations).
Hepatitis C Virus
The prevalence of chronic HCV infection in the United States is approximately 1.3%
(16). Prevalence varies by race/ethnicity, age group, geographic location, and individual history of risk behaviors
(16,17).
Persons with acute HCV infection typically either are asymptomatic or have a mild clinical illness. Antibody to
HCV (anti-HCV) can be detected in 80% of patients within 15 weeks after exposure and in 97% of patients by 6
months after exposure. Chronic HCV infection develops in 75%--85% of infected persons. The majority remain
asymptomatic until onset of cirrhosis or end-stage liver disease, which develops within 20--30 years in approximately 10%--20%
of infected persons (17).
HCV is transmitted primarily through exposure to large amounts of blood or repeated direct percutaneous
exposures to blood (i.e., transfusion or injection-drug use). HCV is not transmitted efficiently through occupational exposures
to blood; the average incidence of anti-HCV seroconversion after accidental percutaneous exposure from an
HCV-positive source is 1.8% (range: 0--7%), with one study indicating that transmission occurred only from
hollow-bore needles (17). Transmission rarely occurs through mucous membrane exposures to blood, and in only one instance
was transmission in a health-care provider attributed
to exposure of nonintact skin to blood (18). The risk for
transmission from exposure to fluids or tissues other than HCV-infected blood has not been quantified but is expected to be low.
The exact duration of HCV viability in the environment is unknown but is at least 16--23 hours
(19,20).
Immune globulin and antiviral agents are not recommended for PEP after exposure to HCV-positive blood. No
vaccine against HCV exists. In the absence of PEP for HCV, recommendations for postexposure management are
intended to achieve early identification of infection and, if present, referral for evaluation of treatment options. No guidelines
exist for administration of therapy during the acute phase of HCV infection. However, limited data indicate that
antiviral therapy might be beneficial when started early in the course of HCV infection. When HCV seroconversion is
identified early, the person should be referred for medical management to a knowledgeable
specialist (12,17).
Testing is not routinely recommended in the absence of a risk factor for infection or a known exposure to an
HCV-positive source (17). However, current public health practice often does include advising testing for potential
exposures to unknown sources (e.g., playground incidents involving needlestick or health-care exposures involving possible
needle or syringe reuse or inadequately disinfected equipment). In the setting of a bombing or other mass-casualty event,
both the extent of exposed disrupted skin and the volume of blood contributing to the exposure might greatly exceed that
of usual occupational exposures. Thus, baseline and follow-up HCV testing should be considered for persons
injured during bombings or other mass-casualty events whose penetrating injuries or nonintact skin are suspected to have
come into contact with another person's blood or body fluids (see Pathogen-Specific Management Recommendations).
Human Immunodeficiency Virus
The overall prevalence of HIV infection in the United States was estimated to be 311.5 per 100,000
population (0.31%) in 2005, with wide geographic variability (range: 26.4 per 100,000 population [0.03%] [North
Dakota]--2,060 per 100,000 population [2.06%] [Washington, DC])
(21). Prevalence might vary greatly among
subpopulations within the same communities (e.g., residents of a nursing home compared with residents of transitional
housing associated with a drug treatment program). The principal means of transmission in the United States is through
sexual contact or through sharing of injection-drug use equipment with an infected person
(21). Exposures also occur in occupational settings (principally among health-care personnel) and infrequently can result in transmission.
Guidelines
for the use of antiretroviral PEP in both occupational and nonoccupational settings have been published previously
(22--24), but these documents do not specifically address situations involving mass casualties.
Potentially infectious materials include blood and visibly bloody body fluids, semen, and vaginal
secretions. Cerebrospinal fluid, synovial fluid, pleural fluid, peritoneal fluid, pericardial fluid, and amniotic fluid also
are considered infectious, but the transmission risk associated with them is less well defined. Feces, nasal secretions,
saliva, sputum, sweat, tears, urine, and vomitus are not considered infectious unless visibly bloody. Exposures that pose a
risk for transmission include percutaneous injuries, contact of mucous membranes, or contact of nonintact skin
with potentially infected fluids (22--24).
In studies of health-care personnel, the average risk for HIV transmission has been estimated to be
approximately 0.3% (95% confidence interval [CI] = 0.2%--0.5%) after a percutaneous exposure to HIV-infected blood
and approximately 0.09% (95% CI = 0.01%--0.5%) after a mucous membrane exposure. Transmission risk from
nonintact skin exposure has not been quantified but is estimated to be less than that for mucous membrane exposure.
Risk following percutaneous exposure is correlated positively with exposure to a larger quantity of blood, direct penetration
of a vein or artery, a deep tissue injury, or exposure
to blood from a source person with terminal illness
(25), presumably related to high viral load.
Use of PEP with antiretroviral medications, initiated as soon as possible after exposure and continuing for 28 days,
has been associated with a decreased risk for infection following percutaneous exposure in health-care settings
(22). PEP also is recommended following nonoccupational sexual and injection-drug use--related
exposures (24). Because of the potential toxicities of antiretroviral drugs, PEP is recommended unequivocally only for exposures to sources known to
be HIV-infected. The decision to use PEP following unknown-source exposures is to be made on a case-by-case
basis, considering the information available about the type of exposure, known risk characteristics of the source, and
prevalence in the setting concerned.
In the majority of instances involving bombings or other mass-casualty events, the working group concluded that
the risk for exposure to HIV-infected materials probably is low and that therefore PEP is not indicated. On this basis, PEP
is not routinely recommended for treating persons injured in mass-casualty settings in the United Kingdom
(7). For the same reason, HIV PEP should not be administered universally in mass-casualty settings in the United States
unless recommended by the local public health
authority. Such instances might occur for mass-casualty events in
certain specific settings judged by public health authorities to be associated with higher risk for HIV exposure (e.g., a
research facility that contained a large archive of HIV-infected blood specimens). In the rare situation in which PEP
is recommended, it should be initiated as soon as possible after exposure, and specimens from the exposed person
should be collected for baseline HIV testing. However, PEP should not be delayed for the results of testing. If PEP is
used, certain other laboratory studies also are indicated. Consultation from health-care professionals knowledgeable about
HIV infection is ideal, and is particularly important for pediatric patients and pregnant women. All persons for whom
HIV PEP has been initiated should be referred to a clinician experienced in HIV care for follow up.
Tetanus
Clostridium tetani, the causative agent of tetanus, is ubiquitous in the environment and distributed worldwide.
The organism is found in soil and in the intestines of animals and humans. When spores of
C. tetani are introduced into the anaerobic or hypoaerobic conditions found in wounds or devitalized tissue, they germinate to vegetative bacilli
that elaborate toxin and cause disease. This now infrequent but often fatal disease has been associated with injuries
to otherwise healthy persons, particularly during military conflicts. During 1998--2000, the case-fatality ratio
for reported tetanus in the United States was 18%
(26). Although tetanus is not transmitted from person to
person, contamination of wounds with debris might increase the risk for tetanus among persons injured in
mass-casualty settings. Proper wound care and debridement play a critical role in tetanus prevention.
Serologic tests indicate that immunity to tetanus toxin is not acquired naturally. However, protection against tetanus
is achievable almost universally by use of highly immunogenic
and safe tetanus toxoid--containing vaccines. The
disease now occurs almost exclusively among persons who were not vaccinated adequately or whose vaccination histories
are
unknown or uncertain (27,28). Universal primary vaccination, with subsequent maintenance of adequate antitoxin
levels by means of appropriately timed boosters, protects persons among all age groups.
The age distribution of recent cases and the results of serosurveys indicate that many U.S. adults are not
protected against tetanus (29). The proportions of persons lacking protective levels of circulating antitoxins against tetanus
increase with age; at least 40% of persons aged
>60 years might lack protection. In the United States, tetanus is primarily
a disease of older adults (27,28). Children are much more likely to have received age-appropriate vaccination; rates
for receipt of 3 doses among children aged 19--35 months exceed 96%
(28). During 1992--2000, only 15 cases of
tetanus were reported in the United States among children aged <15 years. Parental philosophic or religious objection
to vaccination accounted for the absence of immune
protection for 12 (80%) affected children
(30). Foreign-born immigrants, especially those from regions other than North America or Europe, also might be
relatively undervaccinated (29,31).
Available evidence indicates that complete primary vaccination with tetanus toxoid provides long-lasting
protection. After routine childhood tetanus vaccination, the Advisory Committee on Immunization Practices (ACIP)
recommends routine booster vaccination with tetanus
toxoid--containing vaccines every 10 years. For clean and minor wounds,
a booster dose is recommended if the patient has not received a dose within 10 years. For all other wounds, a booster
is appropriate if the patient has not received tetanus toxoid during the preceding 5 years.
In the setting of acute response to a mass-casualty event, failure to provide a tetanus vaccination when needed
could result in preventable illness, whereas unnecessary vaccination is unlikely to cause harm
(26--29,32,33). A substantial proportion of patients in this setting might be unable to provide a history of vaccination or history of
contraindications to tetanus toxoid--containing vaccines, and the majority of wounds sustained will be considered tetanus-prone
because they are likely to be exposed to dirt or feces. Thus, a wounded adult patient who cannot confirm receipt of a
tetanus booster during the preceding 5 years should be vaccinated with tetanus and diphtheria toxoids vaccine (Td) or
tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis vaccine (Tdap); adults aged
>65 years should receive Td (26). Similarly, a child with an uncertain vaccination history should receive a tetanus booster as age-indicated by the
standard childhood immunization table (pediatric diphtheria and tetanus toxoids and acellular pertussis vaccine [DTaP] if
aged <7 years, Td if aged 7--10 years, and Tdap if aged
>11 years) (32,34).
ACIP recommends that patients without a complete primary tetanus series who sustain a tetanus-prone
wound routinely receive passive immunization with tetanus
immune globulin (TIG) and tetanus toxoid
(33). In the setting of acute response to a mass-casualty event, many wounded patients probably will be unable to confirm previous
vaccination histories, and thus TIG normally would be indicated. However, this might not be feasible in a mass-casualty setting
if supplies of TIG are limited. All decisions to administer TIG depend on the number of casualties and the
readily available supply of TIG. If the supply of TIG is adequate, consideration might be given to providing both tetanus
toxoid and passive immunization with TIG at the time of management of tetanus-prone wounds. TIG is
indicated if completion of a primary vaccination series is uncertain for an adult or if prior receipt of age-appropriate vaccinations
is uncertain for a child. If TIG is in short supply, it should be reserved for patients least likely to have received
adequate primary vaccination. In general, this group includes persons aged
>60 years and immigrants from regions other
than North America or Europe who might be less likely to have adequate antitetanus antibodies and who thus would
derive the most benefit from TIG (32).
The TIG prophylactic dose that is recommended currently for wounds is 250 units administered
intramuscularly (IM) for adult and pediatric patients. When tetanus toxoid and TIG are administered concurrently, separate
syringes and separate sites should be used
(35). In circumstances in which passive protection is clearly indicated but TIG
is unavailable, intravenous immune globulin may be substituted for TIG. Postexposure chemoprophylaxis
with antimicrobials against tetanus is not recommended.
ACIP recommends that adults and adolescents with a history of uncertain or incomplete primary vaccination
complete a 3-dose primary series for tetanus, diphtheria, and pertussis
(26,30--34). In the setting of acute response to a
mass-casualty event, completion of the primary vaccination series of any vaccine provided initially during acute
response during follow-up visits should be ensured at the time of discharge for inadequately vaccinated patients of all ages.
Special
precautions regarding management of pregnant women in the setting of emergency delivery have been identified
(see Special Situations).
Recommendations
Risk Assessment
To determine appropriate actions in response to evaluation of casualties of bombings or other mass-casualty
events, health-care providers should
assess individual exposure risk by categorizing the
patient into one of three exposure risk categories
(Box 1) that are numbered sequentially from the highest (category 1) to the lowest (category 3) level of exposure risk and assign
each person to the highest level risk category for which he/she qualifies,
identify the appropriate risk category- and pathogen-specific management recommendation(s) (Box 1), and
determine the appropriate action to take (see Pathogen-Specific Management Recommendations) in
response to management recommendations.
When evaluating management choices for casualties of bombings or other mass-casualty events, health-care
providers should assume that exposure to blood from other injured persons is likely unless available information on
the circumstances of injury suggests otherwise. Blast injuries result occasionally in traumatic implantation of bone or
other biologic material that is alien to the wounded person. Testing of such matter is not recommended as a useful adjunct
for clinical management of wounded persons. Public health authorities can provide assistance in assessing exposure risk
for affected groups of injured persons. Tetanus risk is not dependent upon blood exposure.
Pathogen-Specific Management Recommendations
Hepatitis B Virus
Unless an injured person who is unable to communicate an accurate medical history or for whom medical records
are not readily available is accompanied by a person able to function as a health-care proxy, responders should assume
the absence of a reliable hepatitis B vaccination history and no contraindication to vaccination with hepatitis B vaccine
(see Contraindications and Precautions). If administration of hepatitis B vaccine to a large number of persons after a
mass-casualty event is anticipated to result in shortages of hepatitis B vaccine products, or if such shortages already
exist, assistance with vaccine supply is available (see Vaccine Supply).
Recommendation: Intervene:
Persons for whom neither a reliable history of completed vaccination against HBV nor a known contraindication
to vaccination against HBV exist should receive the first dose of the HBV vaccine series as soon as possible
(preferably within 24 hours) and not later than 7
days after the event.
Persons who receive or are identified as candidates for a dose of hepatitis B vaccine while undergoing evaluation
or treatment in immediate response to a mass-casualty event should be discharged with referrals for follow-up
and written information on predischarge treatment to facilitate the ability of primary health-care providers to
evaluate and, if appropriate, initiate or complete age-appropriate vaccinations or vaccination series (Appendix 1).
Recommendation: No action:
No action is necessary to prevent HBV infection.
Hepatitis C Virus
Recommendation: Consider testing:
Testing should be considered when an HCV-infected source is known or thought to be likely on the basis of
the setting in which the injury occurred or exposure to blood or biologic material from a bomber or multiple
other injured persons is suspected.
Public health authorities can provide assistance in
assessing exposures and therefore treatment for affected groups
of injured persons. A decision to perform testing of specific persons might be made on the basis of the judgment of
the treating physician and the preferences of the individual patient; testing during a follow-up referral might be a
more feasible logistical option in the setting of response to a mass-casualty event.
If a decision is made to perform testing:
baseline testing for anti-HCV and alanine aminotransferase (ALT) should be performed within 7--14 days of
the exposure;
follow-up testing for anti-HCV and ALT should be performed 4--6 months after exposure to assess
seroconversion, preferably arranged as part of discharge planning;
HCV RNA testing should be performed at 4--6 weeks if an earlier diagnosis of HCV infection is desired; and
positive anti-HCV with low signal-to-cutoff value should be confirmed using a more specific supplemental
assay before communicating the results to the
patient; and
persons who are tested or are identified as a candidate for testing regarding exposure to HCV while
undergoing evaluation or treatment in immediate response to a mass-casualty event should be discharged with a referral
for follow-up and written information on pre-discharge
treatment (Appendix 1).
Recommendation: Generally no action:
Exposure of mucous membranes to blood from a source with unknown HCV status generally poses a minor risk
for infection and does not require further action.
However, in settings in which exposure to an HCV-infected source is known or thought to be highly likely,
testing for early identification of HCV infection following mucous membrane exposure may be considered. The decision
to perform testing should be made on the basis of the judgment of the treating physician and the preference of
the individual patient.
Recommendation: No action
No action is necessary to prevent HCV infection.
Human Immunodeficiency Virus
Recommendation: Generally no action:
In general, HIV PEP is not warranted. HIV PEP might be considered only in settings in which exposure to an
HIV-infected source is known or thought to be highly likely (e.g., a blast injury incident that occurred in a
research facility that contained a large archive of HIV infected blood specimens).
HIV PEP should not be administered universally in response to mass-casualty events unless recommended by
the local public health authority.
In the rare event that HIV PEP is considered, it should be initiated as soon as possible after exposure.
The patient should be counseled about the availability of PEP and informed of the potential benefits and risks and
the need for prompt initiation to maximize potential effectiveness. If PEP is thought to be indicated on the basis
of exposure risk, administration should not be delayed for HIV test results. Specific guidance on how to
administer HIV PEP in unusual circumstances when it is warranted is available (see Special Situations).
Persons who receive or are identified as candidates for HIV PEP while undergoing evaluation or treatment
in immediate response to a mass-casualty event should be discharged with referrals for urgent follow-up.
Written information on predischarge treatment should be provided to facilitate a primary health-care provider's ability
to evaluate and, if appropriate, complete age-appropriate vaccinations or vaccination series
(Appendix 1).
In all health-care settings, opt-out screening for HIV (performing HIV screening after notifying the patient that
the test will be performed, with assent inferred unless the patient declines or defers testing) is recommended for
all patients aged 13--64 years. In the setting of response to a mass-casualty event, testing during a follow-up
referral might be a more feasible logistic option unless a decision to administer PEP has been made
(35).
Recommendation: No action:
No action is necessary to prevent HIV infection.
Tetanus
All persons who sustain tetanus-prone injuries in mass-casualty settings should be evaluated for the need for
tetanus prophylaxis. Tetanus-prone injuries include but are not limited to puncture and other penetrating wounds with
the potential to result in an anaerobic environment (wounds resulting from projectiles or by crushing) and
wounds, avulsions, burns, or other nonintact skin that might be contaminated with feces, soil or saliva.
All persons who are not accompanied by either medical records or a health-care proxy and whose ability
to communicate an accurate medical history is uncertain for any reason should be deemed to lack a reliable tetanus
toxoid vaccination history and to have no contraindication to vaccination with tetanus toxoid (see Contraindications
and Precautions). If compliance with recommendations is anticipated to result in a shortage of tetanus toxoid products
or TIG, assistance with product supplies is available (see Vaccine Supply).
Recommendation: Intervene:
Appropriate wound care and debridement are critical to tetanus prevention.
Age-appropriate vaccines should be used if possible. However, in a mass-casualty setting, this might not be
possible, and any tetanus vaccine formulation might be used, because the tetanus toxoid content is adequate for
tetanus prophylaxis in any age group. In this setting, the benefit of supplying tetanus prophylaxis outweighs the
potential for adverse reactions from formulations from a different age indication.
Adult patients who cannot readily confirm receipt of a tetanus booster during the preceding 5 years and who do
not have known contraindication to tetanus vaccination should be vaccinated with Tdap (or with Td if Tdap
is unavailable) or with Td if aged >65 years.
Pediatric patients with uncertain vaccination history and with no known contraindication to tetanus
vaccination should receive a tetanus booster according to the following schedule:
--- DTaP if aged <7 years
--- Td if aged 7--10 years
--- Tdap (or Td if Tdap is unavailable) if aged >11 years.
In a mass-casualty situation, unusually high demand might result in shortages of age-specific vaccine
formulations, and logistic considerations might make differentiating patients by age category prohibitive. If supplies of DTaP
are inadequate, heath-care providers might consider substituting Tdap or Td for DTaP
because the amount of tetanus toxoid in all formulations is adequate to induce an immune response in a child. Similarly, if supplies of Td
are inadequate, health-care providers might consider substituting Tdap for Td for persons aged
>65 years. Pediatric DTaP generally is not indicated in persons aged
>7 years; the increased diphtheria toxoid content is associated
with higher rates of local adverse reactions in older persons
(26,32). However, in a mass-casualty setting, other
options might not exist.
TIG might be indicated if completion of a primary vaccination series is uncertain for an adult, or prior
receipt of age-appropriate vaccinations is uncertain for a child.
--- If TIG is in short supply, use of TIG should be
reserved first for persons aged >60 years and for
immigrants from regions other than North America or Europe. All decisions to administer TIG depend on the number
of casualties and the readily available supply of TIG.
--- The recommended prophylactic dose of TIG is 250 units IM for adult and pediatric patients. When
tetanus toxoid and TIG are administered concurrently, separate syringes and separate sites should be used
(34).
Persons who receive or are identified as candidates for tetanus toxoid--containing products or TIG
while undergoing evaluation or treatment in immediate response to a mass-casualty event should be discharged
with referrals for follow-up if possible. Written information on predischarge treatment should be provided to facilitate
the ability of primary health-care providers to evaluate and, if appropriate, complete
age-appropriate vaccinations or vaccination series (Appendix 1).
Recommendation: No action:
No action is necessary to prevent tetanus. Exposure to blood or other bodily fluids generally is not considered a
risk factor for tetanus.
However, responders or persons engaged in debris clean up and construction are candidates for prophylaxis even
if they do not sustain any wounds. When feasible, as a routine public health measure, tetanus toxoid vaccination
with Tdap or Td should be offered to all persons whose last tetanus toxoid--containing vaccine was
received >10 years previously and who either are
responders or are engaged in either debris clean-up or construction and who
thus might be expected to encounter further risk for exposure
(36--39).
Vaccine and Antitoxin Supply
Adherence to these recommendations might increase the acute demand for tetanus toxoid--containing vaccine,
TIG, and hepatitis B vaccine beyond the available local supply. In that event, local authorities might have to rely on local
and state health departments, mutual aid agreements, or commercial vendors to supplement the supply of needed biologic
or pharmaceutical products. If a local authority's capacity to respond to an emergency is exceeded and other local
or regional resources are inadequate, local and state public health jurisdictions can, through their
established communication channels for health emergencies, work with CDC and others as appropriate to assist with
product shortages.
CDC's Strategic National Stockpile (SNS) maintains bulk quantities of pharmaceutical and
nonpharmaceutical medical supplies for use in a national emergency. Tetanus toxoid, tetanus immune globulin, and hepatitis B vaccine
are not included in the stockpile formulary. However, SNS has purchasing agreements for acquiring medical materials
in large quantities, subject to commercial availability. CDC maintains stockpiles of pediatric vaccine products purchased
by the Vaccines for Children Program that might be used to assist state, territorial, and tribal health departments
in meeting emergent local demands for vaccines. CDC also can work with manufacturers and with state and local
health authorities to assist with supply of vaccines that are not available in either the SNS or other CDC vaccine stockpiles.
Counseling
Hepatitis B and C Viruses
Persons undergoing postexposure management for possible exposure to HBV- or HCV-infected blood do not need
to take any special precautions to prevent secondary transmission during the follow-up period
(12,17). The exposed person does not need to modify sexual practices or refrain from becoming pregnant. An exposed nursing mother might
continue to breastfeed. However, exposed persons should refrain from donating blood, plasma, organs, tissue, or
semen until follow-up testing by the health-care provider has excluded seroconversion
(12,17).
Human Immunodeficiency Virus
Persons known to be exposed to HIV should refrain from blood, plasma, organ, tissue, or semen donation until
follow-up testing by the health-care provider has excluded seroconversion. In addition, measures to prevent sexual
transmission (e.g., abstinence or use of condoms) should be taken, and breastfeeding should be avoided until HIV infection has
been ruled out (22).
Special Situations
When HIV PEP is Initiated
HIV PEP should be considered only under exceptional circumstances. In the rare event that HIV PEP is considered,
it should be initiated as soon as possible after exposure. The patient should be counseled about the availability of PEP
and informed about the potential benefits and risks and the need for prompt initiation to maximize potential effectiveness.
If PEP is thought to be indicated on the basis of exposure risk, administration should not be delayed for HIV test results.
In the rare event that HIV PEP is administered, specimens should be collected for baseline HIV testing on all
patients provided with PEP using a blood or oral fluid rapid test if available; otherwise, conventional testing should be
used. Testing should be discussed with the patient if the patient's medical condition permits. Procedures for testing should
be in accordance with applicable state and local laws. PEP can be initiated and test results reviewed at follow-up. If
the HIV test result is positive, PEP can be discontinued and the patient referred to a clinician experienced with HIV care
for treatment.
If PEP is administered, the health-care provider also should obtain baseline complete blood count, renal
function, hepatic function tests, and, in women, a pregnancy test. Because efavireniz might be teratogenic, it should not
be administered until pregnancy test results are available
(12,22). Otherwise, test results need not be available
before PEP initiation but should be reviewed in follow-up.
Selection of antiretroviral regimens should aim for simplicity and tolerability. Because of the complexity of selection
of HIV PEP regimens, consultation with persons having expertise in antiretroviral therapy and HIV transmission
is strongly recommended. Resources for consultation are available from the following sources:
local infectious diseases, hospital epidemiology, or
occupational health consultants;
local, state, or federal public health authorities;
previously published guidance (see Information Sources).
Nevirapine should not be included in HIV PEP regimens because of potential severe hepatic and cutaneous
toxicity. Efavirenz should not be used if pregnancy is known or suspected because of potential teratogenicity
(12,22).
PEP should be started as soon after exposure as possible and continue for 4 weeks. For ambulatory patients, a
starter pack of 5--7 days of medication should be provided, if possible. Alternatively, for hospitalized patients, the first
dose should be taken in the emergency department, and follow-up orders should be written for completion of the course
in the hospital.
Patients on PEP should be reassessed for adherence, toxicity, and for follow-up of HIV testing (if rapid testing was
not available at baseline) within 72 hours by an infectious disease consultant. Patients continuing on PEP should
have follow-up laboratory evaluation as recommended previously
(22--24), including a complete blood count and renal
and hepatic function tests at baseline and at 2 weeks postexposure, and HIV testing at baseline, 6 weeks,
3 months, and 6 months postexposure.
Persons begun on HIV PEP should be discharged with written instructions and a referral to ensure follow-up care
with a clinician experienced with HIV care and
information on the age-appropriate dose and schedule (Appendix 1).
Simultaneous Administration
When tetanus toxoid and TIG are administered concurrently, separate syringes and separate anatomic sites should
be used (40). Hepatitis B vaccine and tetanus
toxoid--containing vaccines might be administered at the same time
using separate syringes and separate sites
(36).
Treatment with an antimicrobial agent generally is not a contraindication to vaccination
(40). Antimicrobial agents have no effect on the responses to vaccines against tetanus or hepatitis B.
Administration of Blood Products
The administration of hepatitis B vaccine or tetanus
toxoid--containing products does not need to be deferred
in persons who have received a blood transfusion or other blood products.
Pregnancy
Pregnancy is not a contraindication to vaccination against hepatitis B. Limited data suggest that a developing fetus
is not at risk for adverse events when hepatitis B vaccine is administered to a pregnant woman. Available vaccines
contain noninfectious HBsAg and should cause no risk for
infection to the fetus (11).
Pregnancy is not a contraindication for HIV PEP. However, use of efavirenz should be avoided when pregnancy
is known or suspected (11,22).
Pregnant adolescents and adults who received the most recent tetanus toxoid--containing vaccine
>5 years previously generally should receive Td in preference to Tdap when possible
(41).
Responders and Other Personnel
Responders and persons engaged in debris removal or construction often are at risk for incurring wounds
throughout the duration of response and clean up work. As a routine public health measure, health-care providers should
offer tetanus toxoid vaccination to all response workers who do not have a reliable history of receipt of a tetanus
toxoid--containing vaccine during the preceding 10 years, regardless of whether the health-care visit was for a wound
(38,39). Such persons might encounter potential exposure situations throughout the duration of their work in response to
a mass-casualty situation.
Health-care personnel, emergency response, public safety and other workers (e.g., construction workers and
equipment operators) who are injured and exposed to blood while providing assistance after a mass-casualty event should
be managed according to existing guidelines and standards for the management of occupational exposures
(10,22,42). Health-care personnel and first responders whose activities involve contact with blood or other body fluids should
have been previously vaccinated against HBV and tetanus
(12,22).
Contraindications and Precautions
Hepatitis B Vaccine
Hepatitis B vaccination is contraindicated for persons with a history of anaphylactic allergy to yeast or any
vaccine component (11). On the basis of CDC's Vaccine Study Datalink data, the estimated incidence of anaphylaxis
among children and adolescents who received hepatitis B vaccine
is 1 case per 1.1 million vaccine doses distributed (95% CI
= 0.1--3.9) (11). Persons with a history of serious adverse events (e.g., anaphylaxis) after receipt of hepatitis B
vaccine should not receive additional doses. Vaccination is not contraindicated in persons with a history of multiple
sclerosis, Guillain-Barré syndrome, autoimmune disease (e.g., systemic lupus erythematosis or rheumatoid arthritis), or
other chronic diseases (11).
Antiretroviral Therapy
Nevirapine should not be included in HIV PEP regimens because of potential severe hepatic and cutaneous
toxicity. Efavirenz should not be used if pregnancy is known or suspected because of potential teratogenicity
(12,22).
Preparations Containing Tetanus Toxoid
The only contraindication to preparations containing tetanus toxoid (TT, Td, or Tdap) is a history of a neurologic
or severe allergic reaction following a previous dose. Local side effects alone do not preclude continued use
(26,30,31). If a person has a wound that is neither clean nor minor and for which tetanus prophylaxis is indicated, but also
a contraindication to receipt of tetanus toxoid--containing preparations, only passive immunization using human
TIG should be administered.
Reporting Adverse Events
Vaccine Adverse Events Reporting System
Any clinically significant adverse events that occur after administration of any vaccine should be reported to
the Vaccine Adverse Events Reporting System (VAERS) even if causal relation to vaccination is uncertain. The
National Childhood Vaccine Injury Act requires health-care providers to report to VAERS any event listed by the
vaccine manufacturers as a contraindication to subsequent doses of the vaccine or any event listed in the Reportable Events
Table (available at http://vaers.hhs.gov/reportable.htm) that occurs within the specified period after vaccination. VAERS reporting forms and information can be requested 24 hours a day at telephone 800-822-7967 or by accessing VAERS
at http://vaers.hhs.gov. Web-based reporting also is available, and providers are encouraged to report adverse
events electronically at
http://secure.vaers.org/VaersDataEntryintro.htm.
Reporting Adverse Events Associated With Antiretroviral Drugs and TIG
Unusual or severe toxicities believed to be associated with use of antiretroviral agents or TIG should be reported
to FDA's MEDWATCH program (http://www.fda.gov/medwatch) at MedWatch, HF-2, Food and Drug
Administration, 5600 Fishers Lane, Rockville, MD 20857;
telephone 800-332-1088.
National Vaccine Injury Compensation Program
The National Vaccine Injury Compensation Program (NVICP) was established by the National Childhood
Vaccine Injury Act and became operational on October 1, 1988. Intended as an alternative to civil litigation under
the traditional tort system (in that negligence need not be proven), NVICP is a no-fault system in which persons thought
to have suffered an injury or death as a result of administration of a covered vaccine may seek compensation. Claims may
be filed on behalf of infants, children and adolescents, or by adults receiving VICP-covered vaccines. Other
legal requirements (e.g., the statute of limitations for filing an injury or death claim) must be satisfied to
pursue compensation. Claims arising from covered vaccines must be adjudicated through the program before civil litigation
can be pursued. The program relies on a Reportable Events Table listing the vaccines covered by the program and
the injuries, disabilities, illnesses, and conditions (including death) for which compensation might be awarded.
Additional information about NVICP is available at
http://www.hrsa.gov/vaccinecompensation or from the National Vaccine
Injury Compensation Program, Health Resources and Services Administration, Parklawn Building, Room 11C-26,
5600 Fishers Lane, Rockville, MD 20857; telephone 800-338-2382.
Information Sources
Recommendations for immediate prophylactic interventions have been summarized
(Table 2). Recommendations for issues that might arise in association with immediate prophylactic intervention also have been summarized
(Table 3).
In addition to the guidance provided in these recommendations, information on specific vaccines or other
prophylactic interventions also is available (Box
2). ACIP recommendations regarding vaccine use are published by
MMWR. Electronic subscriptions are available free of charge at
http://www.cdc.gov/subscribe.html. Printed subscriptions
are available at Superintendent of Documents, U.S. Government Printing Office, Washington, D.C.
20402-9235, telephone 202-512-1800.
Acknowledgments
Contributors to this report included the National Association of County and City Health Officials, the Council of State and
Territorial Epidemiologists, the Terrorism Injuries: Information Dissemination and Exchange (TIIDE) partnership, and the following persons:
Italo Subbarao, DO, Center for Public Health Preparedness and Disaster Response, American Medical Association; Richard Sattin, MD, Division
of Injury Response, National Center for Injury Prevention and Control; Richard McCluskey, MD, Coordinating Office for Terrorism
Preparedness and Emergency Response; Jeanne Santoli, MD, Immunization Services Division, National Center for Immunizations and Respiratory
Diseases; William Atkinson, MD, Immunization Services Division, National Center for Immunizations and Respiratory Diseases, CDC.
Siegel-Itzkovich J. Israeli minister orders hepatitis B vaccine for survivors of suicide bomb attacks. BMJ 2001;323:417.
Braverman I, Wexler D, Oren M. A novel mode of infection with hepatitis B: penetrating bone fragments due to the explosion of a suicide
bomber. Isr Med Assoc J 2002;4:528--9.
Wong J M-l, Marsh D, Abu-Sitta G, et al. Biological foreign body implantation in victims of the London July 7th suicide bombings. J
Trauma 2006;60:402--4.
Israel Ministry of Health. Hepatitis B vaccination protocol in survivors of mass casualty bombings. Israel Ministry of Health Medical
Guidelines 2001(35)/1/13(Communique 57/2001).
Israel Ministry of Health. Hepatitis B vaccination protocol in survivors of mass casualty bombings--revision. Israel Ministry of Health
Medical Guidelines 2001(35)/2/13(Communique 72/2001).
Health Protection Agency. Post exposure prophylaxis against hepatitis B for bomb victims and immediate care providers. Consideration of
other blood borne viruses (hepatitis C and HIV). London, United Kingdom: Health Protection Agency; 2005.
Jagger J, De Carli G, Perry J, Puro V, Ippolito G. Occupational exposure to bloodborne pathogens: epidemiology and prevention. In: Wenzel R,
ed. Prevention and control of nosocomial infections. 4th ed. Baltimore, MD: Lippincott, Williams and Wilkins; 2003.
Alter HJ, Stramer SL, Dodd RY. Emerging infectious diseases that threaten the blood supply. 1. Semin Hematol 2007;44:32--41.
Armstrong GL, Wasley A, Simard EP, McQuillan GM, Kuhnert WL, Alter MJ. The prevalence of hepatitis C virus infection in the United
States, 1999 through 2002. Ann Intern Med 2006;144:705--14.
Beltrami EM, Kozak A, Williams IT, et al. Transmission of HIV and hepatitis C virus from a nursing home patient to a health care worker. Am
J Infect Control 2003;31:168--75.
Kamili S, Krawczynski K, McCaustland K, Li X, Alter MJ. Infectivity of hepatitis C virus in plasma after drying and storing at room
temperature. Infect Control Hosp Epidemiol 2007;28:519--24.
Patel PR, Larson AK, Castel AD, et al. Hepatitis C virus infections from a contaminated radiopharmaceutical used in myocardial perfusion
studies. JAMA 2006;296:2005--11.
CDC. HIV/AIDS surveillance report, cases of HIV infection and AIDS in the United States and dependent areas, 2005. Vol 17. Revised June
2007. Atlanta, GA: US Department of Health and Human Services, Public Health Service, CDC; 2007.
Srivastava P, Brown K, Chen J, Kretsinger K, Roper M. Trends in tetanus epidemiology in the United States, 1972--2001 [Presentation].
Presented at the 39th National Immunization Conference, Washington, DC; March 21--24, 2005. Available at
http://cdc.confex.com/cdc/nic2005/techprogram/paper_7813.htm.
McQuillan GM, Kruszon-Moran D, Deforest A, et al. Serologic
immunity to diphtheria and tetanus in the United States. Ann Intern
Med 2002;136:660--6.
Fair E, Murphy T, Golaz A, Wharton M. Philosophic objection to vaccination as a risk factor for tetanus among children younger than 15
years. Pediatrics 2002;109:E2.
Talan DA, Abrahamian FM, Moran GJ, et al. Tetanus immunity and physician compliance with tetanus prophylaxis practices among
emergency department patients presenting with wounds. Ann Emerg Med 2004;43:305--11.
CDC. Update: NIOSH warns of hazards of flood cleanup work.
Atlanta, GA: US Department of Health and Human Services, CDC;
1997. NIOSH publication no. 94-123. Available at
http://www.cdc.gov/niosh/flood.html.
Occupational Safety and Health Administration. Fact sheets on natural disaster recovery: flood cleanup. Washington, DC: US Department
of Labor, Occupational Safety and Health Administration; 2008. Available at
http://www.osha.gov/OshDoc/floodCleanup.html.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.

![TABLE 2. Summary of recommendations for immediate prophylactic intervention
Type of injury or
blood exposure HBV* HCV† HIV§ Tetanus
Category 1. Penetrating
injury/nonintact skin¶
Category 2. Mucous
membranes††
Category 3. Superficial
exposure of intact
skin††
For persons for whom
no reliable history of
hepatitis B vaccination
exists and for whom no
contraindication to
vaccine is known,
initiate hepatitis B
vaccine series,
preferably within 24
hours and not later than
7 days.
For persons for whom
no reliable history of
hepatitis B vaccination
exists and for whom no
contraindication to
vaccine is known,
initiate hepatitis B
vaccine series,
preferably within 24
hours and not later than
7 days.
No action
No prophylaxis
recommended.Consider
testing (immediately or
during a follow-up
referral) if exposure is
to a known or likely
HCV-infected source or
multiple sources. If
testing is performed,
obtain baseline (within
7-14 days) and followup
(4–6 months) anti-
HCV and ALT.
Generally no action.
Testing for early
identification of HCV
infection following
mucous membrane
exposure should be
considered only in
settings in which
exposure to an HCVinfected
source is
known or thought to be
highly likely.
No action
Generally, no PEP** is
warranted; consider
only if exposure is to a
known or highly likely
HIV-infected source.
Generally, no PEP** is
warranted. Consider
only if exposure is to a
known or highly likely
HIV-infected source.
No action
Clean and debride
wound as
appropriate.Give ageappropriate
tetanus
toxoid vaccine if date of
receipt of last dose is
unknown and no known
history of vaccine
contraindication exists.
May consider administering
TIG (in addition to
tetanus toxoid) if no
reliable history of
tetanus primary series
exists (always use
separate syringes and
separate administration
sites). If TIG is in short
supply, persons aged
>60 yrs and immigrants
from regions other than
Europe or North
America are most likely
to derive benefit.
No action
No action
* Hepatitis B vaccine.
† Hepatitis C vaccine.
§ Human immunodeficiency virus.
¶ Penetration of skin by a sharp object that was in contact with blood, tissue, or other potential infectious body fluid (i.e., semen, vaginal fluid,
cerebrospinal fluid, synovial fluid, pleural fluid, peritoneal fluid, pericardial fluid, amniotic fluid or any other visibly bloody body fluid or tissue) before
penetration. Nonintact skin exposure is defined as contact of nonintact skin with any of these potentially infectious tissues or fluids
** Postexposure prophylaxis. HIV PEP rarely is indicated. If PEP is indicated, the following procedures should be undertaken: 1) PEP should be started
as soon as possible after exposure, without waiting for HIV test results; 2) PEP should be continued for 4 weeks; 3) Specimens should be collected
for baseline testing, including HIV, complete blood count, liver function, creatinine, and pregnancy tests; 4) testing should be conducted in accordance
with applicable state and local laws; 5) expert consultation should be obtained; sources of expert consultation include local persons with infectious
diseases, hospital epidemiology, or occupational health expertise; local, stage, or federal public health authorities; PEPline (available 24 hours/day via
telephone 1-888-448-4911 [preferred] or online at http://www.nccc.ucsf.edu/Hotlines/PEPline.html; or the HIV/AIDS Rx information service at http://
aidsinfo.nih.gov; 6) PEP should be continued for 4 weeks; 7) the patient should be discharged with written information, a 5–7 day supply of medication,
and a follow-up appointment; and. 8) an HIV specialist should reassess the patient’s condition within 72 hours.
†† Contact of mucous membranes (i.e., eyes, nose, mouth, or inner surfaces of the gut or genital areas) with blood, tissue, or other potential infectious
body fluid (i.e., semen, vaginal fluid, cerebrospinal fluid, synovial fluid, pleural fluid, peritoneal fluid, pericardial fluid, amniotic fluid or any other visibly
bloody body fluid or tissue).
†† Superficial exposure of intact skin (but not of mucous membranes) with blood, tissue, or other potential infectious body fluid (i.e., semen, vaginal fluid,
cerebrospinal fluid, synovial fluid, pleural fluid, peritoneal fluid, pericardial fluid, amniotic fluid or any other visibly bloody body fluid or tissue).](figures/r706a1t2.gif)
![TABLE 3. Summary of recommendations for issues in special situations potentially associated with immediate prophylactic
intervention
Issue/Situation HBV* HCV† HIV§ Tetanus
Vaccine supply
shortage
Counseling
HIV PEP** is initiated
Local public health
departments, mutual aid
agreements, or
commercial vendors
should be relied on.If
local capacity is
exceeded, local public
health authorities should
work through established
communication
channels with CDC and
others.
Exposed persons
should refrain from
donating blood, plasma,
organs, tissue, or
semen.
NA
NA¶
Exposed persons
should refrain from
donating blood, plasma,
organs, tissue, or
semen.
NA
NA
Exposed persons
should refrain from
donating blood, plasma,
organs, tissue, or
semen. In addition,
persons known to be
exposed to HIV should
avoid breastfeeding and
organ/tissue donation
and take precautions to
avoid sexual transmission
until HIV infection
has been ruled out.
HIV PEP rarely is
indicated. If it is,
recommended
procedures should be
followed.††
Age-appropriate
vaccines are preferred.
If age-appropriate
vaccine supply is
expended, any tetanus
vaccine formulation
may be used, as the
tetanus toxoid content
is adequate for tetanus
prophylaxis in any age
group. In this setting,
the benefit of supplying
tetanus prophylaxis
outweighs the potential
for adverse reactions
from formulations from
a different age indication.
Local public health
departments, mutual aid
agreements, or
commercial vendors
should be relied on. If
local capacity is
exceeded, local public
health authorities should
work through established
communication
channels with CDC and
others.
NA
* Hepatitis B vaccine.
† Hepatitis C vaccine.
§ Human immunodeficiency virus.
¶ Not applicable.
** Postexposure prophylaxis.
†† If PEP is indicated, the following procedures should be undertaken: 1) PEP should be started as soon as possible after exposure, without waiting for
HIV test results; 2) PEP should be continued for 4 weeks; 3) specimens should be collected for baseline testing, including HIV, complete blood count,
liver function, creatinine, and pregnancy tests; 4) testing should be conducted in accordance with applicable state and local laws; 5) expert
consultation should be obtained; sources of expert consultation include local persons with infectious diseases, hospital epidemiology, or occupational
health expertise; local, stage, or federal public health authorities; PEPline (available 24 hours/day at telephone 1-888-448-4911 [preferred] or at http://
www.nccc.ucsf.edu/Hotlines/PEPline.html; or the HIV/AIDS Rx information service, available at http://aidsinfo.nih.gov; 6) PEP should be continued for
4 weeks; 7) the patient should be discharged with written information, a 5–7 day supply of medication, and a follow-up appointment; and 8) an HIV
specialist should reassess the patient’s condition within 72 hours.](figures/r706a1t3.gif)