 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Recommendations for Prevention and Control of Hepatitis C Virus (HCV) Infection and HCV-Related Chronic DiseaseTerms and Abbreviations Used in This Publication Acute hepatitis C Newly acquired symptomatic hepatitis C virus (HCV) infection. ALT Alanine aminotransferase. Anti-HCV Antibody to HCV that develops in response to HCV infection; detectable in persons with acute, chronic, and resolved infection. AST Aspartate aminotransferase. Chronic (persistent) HCV infection Persistent infection with HCV; characterized by detection of HCV RNA greater than or equal to 6 months after newly acquired infection. Chronic hepatitis C Liver inflammation in patients with chronic HCV infection; characterized by abnormal levels of liver enzymes. CSTE Council of State and Territorial Epidemiologists. DNA Deoxyribonucleic acid. EIA Enzyme immunoassay. FDA U.S. Food and Drug Administration. HBV Hepatitis B virus. HCC Hepatocellular carcinoma. HCV Hepatitis C virus. HCV-positive Positive for anti-HCV as verified by supplemental testing or positive for HCV RNA. HCV RNA Hepatitis C virus ribonucleic acid. HIV Human immunodeficiency virus. IG Immune globulin. IM Intramuscular. IV Intravenous. MSM Men who have sex with men. NHANES III Third National Health and Nutrition Examination Survey. NIH National Institutes of Health. Positive predictive value Probability that a positive screening test is truly positive; dependent on prevalence of disease in a population. Qualitative RT-PCR for HCV RNA Test to detect HCV RNA by amplification of viral genetic sequences. Quantitative assays for HCV RNA Tests to detect HCV RNA concentration (viral load) by amplification of viral genetic sequences or by signal amplification. Resolved HCV infection Recovery following hepatitis C virus infection; characterized by sustained disappearance of serum HCV RNA and normalization of liver enzymes. RIBATM Recombinant immunoblot assay. RNA Ribonucleic acid. RT-PCR Reverse transcriptase polymerase chain reaction. STD Sexually transmitted disease. Supplemental anti-HCV test Additional test (i.e.,RIBATM) used to verify a positive anti-HCV result obtained by EIA. Expert Consultants Harvey J. Alter, M.D., Department of Transfusion Medicine, National Institutes of Health, Bethesda, Maryland; Tomas Aragon, M.D., M.P.H., San Francisco Department of Health, San Francisco, California; James P. AuBuchon, M.D., Department of Pathology, Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire; Geoff Beckett, M.P.H., Maine Department of Health, Augusta, Maine; Celso Bianco, M.D., New York Blood Center, New York, New York; Robin Biswas, M.D., U.S. Food and Drug Administration, Bethesda, Maryland; Robert L. Carithers, Jr., M.D., University of Washington School of Medicine, Seattle, Washington; William Cassidy, M.D., Louisiana State University Medical Center, Baton Rouge, Louisiana; Jeffery P. Davis, M.D., Wisconsin Department of Health and Human Services, Madison, Wisconsin; Katherine Davenny, M.P.H., National Institute on Drug Abuse, National Institutes of Health, Bethesda, Maryland; Roger Y. Dodd, Ph.D., American Red Cross, Bethesda, Maryland; Cherie S. Evans, M.D., Blood Bank of Alameda-Contra Costa Counties, Oakland, California; Harold J. Fallon, M.D., School of Medicine, University of Alabama, Birmingham, Alabama; Michael E. Fleenor, M.D., Jefferson County Department of Health, Birmingham, Alabama; Lewis M. Flint, M.D., Tulane University School of Medicine, New Orleans, Louisiana; Ted G. Ganiats, M.D., University of California San Diego, La Jolla, California; Kathy Getz, Council of State and Territorial Epidemiologists, Atlanta, Georgia; H. Hunter Handsfield, M.D., Seattle-King County Department of Health, Seattle, Washington; Richard E. Hoffman, M.D., M.P.H., Colorado Department of Public Health and Environment, Denver, Colorado; F. Blaine Hollinger, M.D., Baylor College of Medicine, Houston, Texas; Harriet Homan, Multnomah County Health Department, Portland, Oregon; Jay H. Hoofnagle, M.D., M.P.H., National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland; Leslye Johnson, Ph.D., National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, Maryland; Franklyn N. Judson, M.D., Denver Department of Public Health, Denver, Colorado; Richard J. Kagan, M.D., Department of Surgery, University of Cincinnati, Cincinnati, Ohio; Louis Katz, M.D., Mississippi Valley Regional Blood Center, Davenport, Iowa; Newton Kendig, M.D., Federal Bureau of Prisons, Washington, DC; Peter R. Kerndt, M.D., Los Angeles County Health Services, Los Angeles, California; Marcelle Layton, M.D., Bureau of Communicable Disease, New York City Department of Health, New York, New York; Karen L. Lindsay, M.D., University of Southern California School of Medicine, Los Angeles, California; Michael K. Lindsay, M.D., Department of Obstetrics and Gynecology, Emory University School of Medicine, Atlanta, Georgia; Michael Meit, M.A., M.P.H., National Association of County and City Health Officials, Washington, DC; Robert W. Moon, M.P.H., Health Systems Bureau, Montana Department of Public Health and Human Services, Helena, Montana; Karen Mottram, Tacoma-Pierce County Health Department, Tacoma, Washington; Jeanne C. Mowe, M.D., American Association of Tissue Banks, McLean, Virginia; Victor J. Navarro, M.D., Yale University School of Medicine, New Haven, Connecticut; Richard Needle, M.D., National Institute on Drug Abuse, National Institutes of Health, Rockville, Maryland; George Nemo, Ph.D., National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland; Okay Odocha, M.D., F.A.C.S., Howard University, Washington, DC; Peter L. Page, M.D., American Red Cross, Arlington, Virginia; Brian J. G. Pereira, M.D., New England Medical Center, Boston, Massachusetts; Randall S. Pope, Michigan Department of Community Health, Lansing, Michigan; David Rimland, M.D., Veterans Affairs Medical Center, Decatur, Georgia; Anthony Rodriguez, M.D., Gay and Lesbian Medical Association, Abington, Pennsylvania; Jon Rosenberg, California Department of Health Services, Berkeley, California; Kate Rothko, M.D., Veterans Administration Medical Center, Washington, DC; Patricia L. Ryder, M.D., M.P.H., Pinellas County Health Department, St. Petersburg, Florida; Eugene R. Schiff, M.D., University of Miami School of Medicine, Miami, Florida; Leonard B. Seeff, M.D., National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland; Richard Steece, Ph.D., Association of State and Territorial Public Health Laboratory Directors, Pierre, South Dakota; Litjen J. Tan, Ph.D., American Medical Association, Chicago, Illinois; Norah Terrault, M.D., M.P.H., University of California San Francisco, San Francisco, California; David Thomas, M.D., The Johns Hopkins University School of Medicine, Baltimore, Maryland; John Ticehurst, M.D., U.S. Food and Drug Administration, Kensington, Maryland; James C. Turner, M.D., Department of Student Health, University of Virginia, Charlottesville, Virginia; Ramona Walker, San Diego Blood Bank, San Diego, California; Steven Wiersma, M.D., Florida Department of Health, Tallahassee, Florida; Richard Whitley, M.D., University of Alabama, Birmingham, Alabama; Rebecca Wurtz, M.D., Evanston Hospital, Evanston, Illinois. Agency Liaison Participants: William B. Baine, M.D., Agency for Health Care Policy and Research, Bethesda, Maryland; David Cade, Health Care Financing Administration, Baltimore, Maryland.; James Cheek, M.D., Indian Health Service, Albuquerque, New Mexico; Warren Hewitt, M.S. and Lucille Perez, M.D., Substance Abuse and Mental Health Services Administration, Bethesda, Maryland; James Riddle, D.O.M., M.P.H., U.S. Department of Defense, Washington, DC; Jose L. Sanchez, M.D., M.P.H., Center for Health Promotion and Preventive Medicine, United States Army, Aberdeen Proving Ground, Maryland.; Maria Sjogren, M.D., Walter Reed Army Medical Center, United States Army, Washington, DC; David Trump, M.D., M.P.H., U.S. Department of Defense, Washington, DC; Virginia Wanamaker, Health Care Financing Administration, Baltimore, Maryland. The following CDC staff members prepared this report: Miriam J. Alter, Ph.D. Harold S. Margolis, M.D. and Beth P. Bell, M.D., M.P.H. Steven D. Bice, M.Ed. Joanna Buffington, M.D., M.P.H. Mary Chamberland, M.D. Patrick J. Coleman, Ph.D. Beverley A. Cummings, M.P.H. Catherine M. Dentinger, M.S. Richard S. Garfein, Ph.D. Wesley Hodgson, M.P.A. Kirsten Braatz Ivie, M.P.H. Mack G. Kelly Rima Khabbaz, M.D. Rob Lyerla, Ph.D. Lisa D. Mahoney, M.P.H. Eric E. Mast, M.D., M.P.H. Linda A. Moyer Keith M. Sabin, Ph.D., M.P.H., M.S. Craig N. Shapiro, M.D. Linda V. Venczel, Ph.D. Annemarie Wasley, Sc.D. Ian A. Williams, Ph.D., M.S. with support from Steven C. Bloom Monica Brittian Kimberly A. Clark Diane Ivey Carlisle A. Quantrell Delray Smith Goldie S. Tillman Division of Viral and Rickettsial Diseases National Center for Infectious Diseases in consultation with Helene D. Gayle, M.D., M.P.H. National Center for HIV, STD, and TB Prevention and Edward L. Baker, M.D., M.P.H. Public Health Practice Program Office Summary These recommendations are an expansion of previous recommendations for the prevention of hepatitis C virus (HCV) infection that focused on screening and follow-up of blood, plasma, organ, tissue, and semen donors (CDC. Public Health Service inter-agency guidelines for screening donors of blood, plasma, organs, tissues, and semen for evidence of hepatitis B and hepatitis C. MMWR 1991;40{No. RR-4};1-17). The recommendations in this report provide broader guidelines for a) preventing transmission of HCV; b) identifying, counseling, and testing persons at risk for HCV infection; and c) providing appropriate medical evaluation and management of HCV-infected persons. Based on currently available knowledge, these recommendations were developed by CDC staff members after consultation with experts who met in Atlanta during July 15-17, 1998. This report is intended to serve as a resource for health-care professionals, public health officials, and organizations involved in the development, delivery, and evaluation of prevention and clinical services. INTRODUCTION Hepatitis C virus (HCV) infection is the most common chronic bloodborne infection in the United States. CDC staff estimate that during the 1980s, an average of 230,000 new infections occurred each year (CDC, unpublished data). Although since 1989 the annual number of new infections has declined by greater than 80% to 36,000 by 1996 (1,2), data from the Third National Health and Nutrition Examination Survey (NHANES III), conducted during 1988-1994, have indicated that an estimated 3.9 million (1.8%) Americans have been infected with HCV (3). Most of these persons are chronically infected and might not be aware of their infection because they are not clinically ill. Infected persons serve as a source of transmission to others and are at risk for chronic liver disease or other HCV-related chronic diseases during the first two or more decades following initial infection. Chronic liver disease is the tenth leading cause of death among adults in the United States, and accounts for approximately 25,000 deaths annually, or approximately 1% of all deaths (4). Population-based studies indicate that 40% of chronic liver disease is HCV-related, resulting in an estimated 8,000-10,000 deaths each year (CDC, unpublished data). Current estimates of medical and work-loss costs of HCV-related acute and chronic liver disease are greater than $600 million annually (CDC, unpublished data), and HCV-associated end-stage liver disease is the most frequent indication for liver transplantation among adults. Because most HCV-infected persons are aged 30-49 years (3), the number of deaths attributable to HCV-related chronic liver disease could increase substantially during the next 10-20 years as this group of infected persons reaches ages at which complications from chronic liver disease typically occur. HCV is transmitted primarily through large or repeated direct percutaneous exposures to blood. In the United States, the relative importance of the two most common exposures associated with transmission of HCV, blood transfusion and injecting-drug use, has changed over time (Figure_1) (2,5). Blood transfusion, which accounted for a substantial proportion of HCV infections acquired greater than 10 years ago, rarely accounts for recently acquired infections. Since 1994, risk for transfusion-transmitted HCV infection has been so low that CDC's sentinel counties viral hepatitis surveillance system* has been unable to detect any transfusion-associated cases of acute hepatitis C, although the risk is not zero. In contrast, injecting-drug use consistently has accounted for a substantial proportion of HCV infections and currently accounts for 60% of HCV transmission in the United States. A high proportion of infections continues to be associated with injecting-drug use, but for reasons that are unclear, the dramatic decline in incidence of acute hepatitis C since 1989 correlates with a decrease in cases among injecting-drug users. Reducing the burden of HCV infection and HCV-related disease in the United States requires implementation of primary prevention activities to reduce the risk for contracting HCV infection and secondary prevention activities to reduce the risk for liver and other chronic diseases in HCV-infected persons. The recommendations contained in this report were developed by reviewing currently available data and are based on the opinions of experts. These recommendations provide broad guidelines for a) the prevention of transmission of HCV; b) the identification, counseling, and testing of persons at risk for HCV infection; and c) the appropriate medical evaluation and management of HCV-infected persons. BACKGROUND Prospective studies of transfusion recipients in the United States demonstrated that rates of posttransfusion hepatitis in the 1960s exceeded 20% (6). In the mid-1970s, available diagnostic tests indicated that 90% of posttransfusion hepatitis was not caused by hepatitis A or hepatitis B viruses and that the move to all-volunteer blood donors had reduced risks for posttransfusion hepatitis to 10% (7-9). Although non-A, non-B hepatitis (i.e., neither type A nor type B) was first recognized because of its association with blood transfusion, population-based sentinel surveillance demonstrated that this disease accounted for 15%-20% of community-acquired viral hepatitis in the United States (5). Discovery of HCV by molecular cloning in 1988 indicated that non-A, non-B hepatitis was primarily caused by HCV infection (5,10-14). Epidemiology Demographic Characteristics HCV infection occurs among persons of all ages, but the highest incidence of acute hepatitis C is found among persons aged 20-39 years, and males predominate slightly (5). African Americans and whites have similar incidence of acute disease; persons of Hispanic ethnicity have higher rates. In the general population, the highest prevalence rates of HCV infection are found among persons aged 30-49 years and among males (3). Unlike the racial/ethnic pattern of acute disease, African Americans have a substantially higher prevalence of HCV infection than do whites (Figure_2). Prevalence of HCV Infection in Selected Populations in the United States The greatest variation in prevalence of HCV infection occurs among persons with different risk factors for infection (15) (Table_1). Highest prevalence of infection is found among those with large or repeated direct percutaneous exposures to blood (e.g., injecting-drug users, persons with hemophilia who were treated with clotting factor concentrates produced before 1987, and recipients of transfusions from HCV-positive donors) (12,13,16-22). Moderate prevalence is found among those with frequent but smaller direct percutaneous exposures (e.g., long-term hemodialysis patients) (23). Lower prevalence is found among those with inapparent percutaneous or mucosal exposures (e.g., persons with evidence of high-risk sexual practices) (24-28) or among those with small, sporadic percutaneous exposures (e.g., health-care workers) (29-33). Lowest prevalence of HCV infection is found among those with no high-risk characteristics (e.g., volunteer blood donors) (34; personal communication, RY Dodd, Ph.D., Head, Transmissible Diseases Department, Holland Laboratory, American Red Cross, Rockville, MD, July 1998). The estimated prevalence of persons with different risk factors and characteristics also varies widely in the U.S. population (Table_1) (3; 35-39; CDC, unpublished data). Transmission Modes Most risk factors associated with transmission of HCV in the United States were identified in case-control studies conducted during 1978-1986 (40,41). These risk factors included blood transfusion, injecting-drug use, employment in patient care or clinical laboratory work, exposure to a sex partner or household member who has had a history of hepatitis, exposure to multiple sex partners, and low socioeconomic level. These studies reported no association with military service or exposures resulting from medical, surgical, or dental procedures, tattooing, acupuncture, ear piercing, or foreign travel. If transmission from such exposures does occur, the frequency might be too low to detect. Transfusions and Transplants. Currently, HCV is rarely transmitted by blood transfusion. During 1985-1990, cases of transfusion-associated non-A, non-B hepatitis declined by greater than 50% because of screening policies that excluded donors with human immunodeficiency virus (HIV) infection and donors with surrogate markers for non-A, non-B hepatitis (5,42). By 1990, risk for transfusion-associated HCV infection was approximately 1.5%/recipient or approximately 0.02%/unit transfused (42). During May 1990, routine testing of donors for evidence of HCV infection was initiated, and during July 1992, more sensitive -- multiantigen
Receipt of clotting factor concentrates prepared from plasma pools posed a high risk for HCV infection (44) until effective procedures to inactivate viruses, including HCV, were introduced during 1985 (Factor VIII) and 1987 (Factor IX). Persons with hemophilia who were treated with products before inactivation of those products have prevalence rates of HCV infection as high as 90% (20-22). Although plasma derivatives (e.g., albumin and immune globulin {IG} for intramuscular {IM} administration) have not been associated with transmission of HCV infection in the United States, intravenous (IV) IG that was not virally inactivated was the source of one outbreak of hepatitis C during 1993-1994 (45,46). Since December 1994, all IG products -- IV and IM -- commercially available in the United States must undergo an inactivation procedure or be negative for HCV RNA (ribonucleic acid) before release. Transplantation of organs (e.g., heart, kidney, or liver) from infectious donors to the organ recipient also carried a high risk for transmitting HCV infection before donor screening (47,48). Limited studies of recipients of transplanted tissue have implicated transmission of HCV only from nonirradiated bone tissue of unscreened donors (49,50). As with blood-donor screening, use of anti-HCV-negative organ and tissue donors has virtually eliminated risks for HCV transmission from transplantation. Injecting and Other Illegal Drug Use. Although the number of cases of acute hepatitis C among injecting-drug users has declined dramatically since 1989, both incidence and prevalence of HCV infection remain high in this group (51,52). Injecting-drug use currently accounts for most HCV transmission in the United States, and has accounted for a substantial proportion of HCV infections during past decades (2,5,53). Many persons with chronic HCV infection might have acquired their infection 20-30 years ago as a result of limited or occasional illegal drug injecting. Injecting-drug use leads to HCV transmission in a manner similar to that for other bloodborne pathogens (i.e., through transfer of HCV-infected blood by sharing syringes and needles either directly or through contamination of drug preparation equipment) (54,55). However, HCV infection is acquired more rapidly after initiation of injecting than other viral infections (i.e., hepatitis B virus {HBV} and HIV), and rates of HCV infection among young injecting-drug users are four times higher than rates of HIV infection (19). After 5 years of injecting, as many as 90% of users are infected with HCV. More rapid acquisition of HCV infection compared with other viral infections among injecting-drug users is likely caused by high prevalence of chronic HCV infection among injecting-drug users, which results in a greater likelihood of exposure to an HCV-infected person. A study conducted among volunteer blood donors in the United States documented that HCV infection has been independently associated with a history of intranasal cocaine use (56). (The mode of transmission could be through sharing contaminated straws.) Data from NHANES III indicated that 14% of the general population have used cocaine at least once (CDC, unpublished data). Although NHANES III data also indicated that cocaine use was associated with HCV infection, injecting-drug use histories were not ascertained. Among patients with acute hepatitis C identified in CDC's sentinel counties viral hepatitis surveillance system since 1991, intranasal cocaine use in the absence of injecting-drug use was uncommon (2). Thus, at least in the recent past, intranasal cocaine use rarely appears to have contributed to transmission. Until more data are available, whether persons with a history of noninjecting illegal drug use alone (e.g., intranasal cocaine use) are likely to be infected with HCV remains unknown. Nosocomial and Occupational Exposures. Nosocomial transmission of HCV is possible if infection-control techniques or disinfection procedures are inadequate and contaminated equipment is shared among patients. Although reports from other countries do document nosocomial HCV transmission (57-59), such transmission rarely has been reported in the United States (60), other than in chronic hemodialysis settings (61). Prevalence of antibody to HCV (anti-HCV) positivity among chronic hemodialysis patients averages 10%, with some centers reporting rates greater than 60% (23). Both incidence and prevalence studies have documented an association between anti-HCV positivity and increasing years on dialysis, independent of blood transfusion (62,63). These studies, as well as investigations of dialysis-associated outbreaks of hepatitis C (64), indicate that HCV transmission might occur among patients in a hemodialysis center because of incorrect implementation of infection-control practices, particularly sharing of medication vials and supplies (65). Health-care, emergency medical (e.g., emergency medical technicians and paramedics), and public safety workers (e.g., fire-service, law-enforcement, and correctional facility personnel) who have exposure to blood in the workplace are at risk for being infected with bloodborne pathogens. However, prevalence of HCV infection among health-care workers, including orthopedic, general, and oral surgeons, is no greater than the general population, averaging 1%-2%, and is 10 times lower than that for HBV infection (29-33). In a single study that evaluated risk factors for infection, a history of unintentional needle-stick injury was the only occupational risk factor independently associated with HCV infection (66). The average incidence of anti-HCV seroconversion after unintentional needle sticks or sharps exposures from an HCV-positive source is 1.8% (range: 0%-7%) (67-70), with one study reporting that transmission occurred only from hollow-bore needles compared with other sharps (69). A study from Japan reported an incidence of HCV infection of 10% based on detection of HCV RNA by reverse transcriptase polymerase chain reaction (RT-PCR) (70). Although no incidence studies have documented transmission associated with mucous membrane or nonintact skin exposures, transmission of HCV from blood splashes to the conjunctiva have been described (71,72). The risk for HCV transmission from an infected health-care worker to patients appears to be very low. One published report exists of such transmission during performance of exposure-prone invasive procedures (73). That report, from Spain, described HCV transmission from a cardiothoracic surgeon to five patients, but did not identify factors that might have contributed to transmission. Although factors (e.g., virus titer) might be related to transmission of HCV, no methods exist currently that can reliably determine infectivity, nor do data exist to determine threshold concentration of virus required for transmission. Percutaneous Exposures in Other Settings. In other countries, HCV infection has been associated with folk medicine practices, tattooing, body piercing, and commercial barbering (74-81). However, in the United States, case-control studies have reported no association between HCV infection and these types of exposures (40,41). In addition, of patients with acute hepatitis C who were identified in CDC's sentinel counties viral hepatitis surveillance system during the past 15 years and who denied a history of injecting-drug use, only 1% reported a history of tattooing or ear piercing, and none reported a history of acupuncture (41; CDC, unpublished data). Among injecting-drug users, frequency of tattooing and ear piercing also was uncommon (3%). Although any percutaneous exposure has the potential for transferring infectious blood and potentially transmitting bloodborne pathogens (i.e., HBV, HCV, or HIV), no data exist in the United States indicating that persons with exposures to tattooing and body piercing alone are at increased risk for HCV infection. Further studies are needed to determine if these types of exposures and settings in which they occur (e.g., correctional institutions, unregulated commercial establishments), are risk factors for HCV infection in the United States. Sexual Activity. Case-control studies have reported an association between exposure to a sex contact with a history of hepatitis or exposure to multiple sex partners and acquiring hepatitis C (40,41). In addition, 15%-20% of patients with acute hepatitis C who have been reported to CDC's sentinel counties surveillance system, have a history of sexual exposure in the absence of other risk factors. Two thirds of these have an anti-HCV-positive sex partner, and one third reported greater than 2 partners in the 6 months before illness (2). In contrast, a low prevalence of HCV infection has been reported by studies of long-term spouses of patients with chronic HCV infection who had no other risk factors for infection. Five of these studies have been conducted in the United States, involving 30-85 partners each, in which average prevalence of HCV infection was 1.5% (range: 0% to 4.4%) (56,82-85). Among partners of persons with hemophilia coinfected with HCV and HIV, two studies have reported an average prevalence of HCV infection of 3% (83,86). One additional study evaluated potential transmission of HCV between sexually transmitted disease (STD) clinic patients, who denied percutaneous risk factors, and their steady partners (28). Prevalence of HCV infection among male patients with an anti-HCV-positive female partner (7%) was no different than that among males with a negative female partner (8%). However, female patients with an anti-HCV-positive partner were almost fourfold more likely to have HCV infection than females with a negative male partner (10% versus 3%, respectively). These data indicate that, similar to other bloodborne viruses, sexual transmission of HCV from males to females might be more efficient than from females to males. Among persons with evidence of high-risk sexual practices (e.g., patients attending STD clinics and female prostitutes) who denied a history of injecting-drug use, prevalence of anti-HCV has been found to average 6% (range: 1%-10%) (24-28,87). Specific factors associated with anti-HCV positivity for both heterosexuals and men who have sex with men (MSM) included greater numbers of sex partners, a history of prior STDs, and failure to use a condom. However, the number of partners associated with infection risk varied among studies, ranging from greater than 1 partner in the previous month to greater than 50 in the previous year. In studies of other populations, the number of partners associated with HCV infection also varied, ranging from greater than 2 partners in the 6 months before illness for persons with acute hepatitis C (41), to greater than or equal to 5 partners/year for HCV-infected volunteer blood donors (56), to greater than or equal to 10 lifetime partners for HCV-infected persons in the general population (3). Only one study has documented an association between HCV infection and MSM activity (28), and at least in STD clinic settings, the prevalence rate of HCV infection among MSM generally has been similar to that of heterosexuals. Because sexual transmission of bloodborne viruses is recognized to be more efficient among MSM compared with heterosexual men and women, why HCV infection rates are not substantially higher among MSM compared with heterosexuals is unclear. This observation and the low prevalence of HCV infection observed among long-term spouses of persons with chronic HCV infection have raised doubts regarding the importance of sexual activity in transmission of HCV. Unacknowledged percutaneous risk factors (i.e., illegal injecting-drug use) might contribute to increased risk for HCV infection among persons with high-risk sexual practices. Although considerable inconsistencies exist among studies, data indicate overall that sexual transmission of HCV appears to occur, but that the virus is inefficiently spread through this manner. More data are needed to determine the risk for, and factors related to, transmission of HCV between long-term steady partners as well as among persons with high-risk sexual practices, including whether other STDs promote transmission of HCV by influencing viral load or modifying mucosal barriers. Household Contact. Case-control studies also have reported an association between nonsexual household contact and acquiring hepatitis C (40,41). The presumed mechanism of transmission is direct or inapparent percutaneous or permucosal exposure to infectious blood or body fluids containing blood. In a recent investigation in the United States, an HCV-infected mother transmitted HCV to her hemophilic child during performance of home infusion therapy, presumably when she had an unintentional needle stick and subsequently used the contaminated needle in the child (88). Although prevalence of HCV infection among nonsexual household contacts of persons with chronic HCV infection in the United States is unknown, HCV transmission to such contacts is probably uncommon. In studies from other countries of nonsexual household contacts of patients with chronic hepatitis C, average anti-HCV prevalence was 4% (15). Although infected contacts in these studies reported no other commonly recognized risk factors for hepatitis C, most of these studies were done in countries where exposures commonly experienced in the past from contaminated equipment used in traditional and nontraditional medical procedures might have contributed to clustering of HCV infections in families (75,76,79). Perinatal. The average rate of HCV infection among infants born to HCV-positive, HIV-negative women is 5%-6% (range: 0%-25%), based on detection of anti-HCV and HCV RNA, respectively (89-101). The average infection rate for infants born to women coinfected with HCV and HIV is higher -- 14% (range: 5%-36%) and 17%, based on detection of anti-HCV and HCV RNA, respectively (90,96,98-104). The only factor consistently found to be associated with transmission has been the presence of HCV RNA in the mother at the time of birth. Although two studies of infants born to HCV-positive, HIV-negative women reported an association with titer of HCV RNA, each study reported a different level of HCV RNA related to transmission (92,93). Studies of HCV/HIV-coinfected women more consistently have indicated an association between virus titer and transmission of HCV (102). Data regarding the relationship between delivery mode and HCV transmission are limited and presently indicate no difference in infection rates between infants delivered vaginally compared with cesarean-delivered infants. The transmission of HCV infection through breast milk has not been documented. In the studies that have evaluated breastfeeding in infants born to HCV-infected women, average rate of infection was 4% in both breastfed and bottle-fed infants (95,96,99,100,105,106). Diagnostic criteria for perinatal HCV infection have not been established. Various anti-HCV patterns have been observed in both infected and uninfected infants of anti-HCV-positive mothers. Passively acquired maternal antibody might persist for months, but probably not for greater than 12 months. HCV RNA can be detected as early as 1 to 2 months. Persons with No Recognized Source for Their Infection. Recent studies have demonstrated that injecting-drug use currently accounts for 60% of HCV transmission in the United States (2). Although the role of sexual activity in transmission of HCV remains unclear, less than or equal to 20% of persons with HCV infection report sexual exposures (i.e., exposure to an infected sexual partner or to multiple partners) in the absence of percutaneous risk factors (2). Other known exposures (occupational, hemodialysis, household, perinatal) together account for approximately 10% of infections. Thus, a potential risk factor can be identified for approximately 90% of persons with HCV infection. In the remaining 10%, no recognized source of infection can be identified, although most persons in this category are associated with low socioeconomic level. Although low socioeconomic level has been associated with several infectious diseases and might be a surrogate for high-risk exposures, its nonspecific nature makes targeting prevention measures difficult. Screening and Diagnostic Tests Serologic Assays The only tests currently approved by the U.S. Food and Drug Administration (FDA) for diagnosis of HCV infection are those that measure anti-HCV (Table_2) (107). These tests detect anti-HCV in greater than or equal to 97% of infected patients, but do not distinguish between acute, chronic, or resolved infection. As with any screening test, positive predictive value of enzyme immunoassay (EIA) for anti-HCV varies depending on prevalence of infection in the population and is low in populations with an HCV-infection prevalence of less than 10% (1,34). Supplemental testing with a more specific assay (i.e., recombinant immunoblot assay {RIBATM}) of a specimen with a positive EIA result prevents reporting of false-positive results, particularly in settings where asymptomatic persons are being tested. Supplemental test results might be reported as positive, negative, or indeterminate. An anti-HCV-positive person is defined as one whose serologic results are EIA-test-positive and supplemental-test-positive. Persons with a negative EIA test result or a positive EIA and a negative supplemental test result are considered uninfected, unless other evidence exists to indicate HCV infection (e.g., abnormal ALT levels in immunocompromised persons or persons with no other etiology for their liver disease). Indeterminate supplemental test results have been observed in recently infected persons who are in the process of seroconversion, as well as in persons chronically infected with HCV. Indeterminate anti-HCV results also might indicate a false-positive result, particularly in those persons at low risk for HCV infection. Nucleic Acid Detection The diagnosis of HCV infection also can be made by qualitatively detecting HCV RNA using gene amplification techniques (e.g., RT-PCR) (Table_2) (108). HCV RNA can be detected in serum or plasma within 1-2 weeks after exposure to the virus and weeks before the onset of alanine aminotransferase (ALT) elevations or the appearance of anti-HCV. Rarely, detection of HCV RNA might be the only evidence of HCV infection. Although RT-PCR assay kits for HCV RNA are available for research purposes from various manufacturers of diagnostic reagents, none have been approved by FDA. In addition, numerous laboratories perform RT-PCR using in-house laboratory methods and reagents. Although not FDA-approved, RT-PCR assays for HCV infection are used commonly in clinical practice. Most RT-PCR assays have a lower limit of detection of 100-1,000 viral genome copies/mL. With adequate optimization of RT-PCR assays, 75%-85% of persons who are anti-HCV-positive and greater than 95% of persons with acute or chronic hepatitis C will test positive for HCV RNA. Some HCV-infected persons might be only intermittently HCV RNA-positive, particularly those with acute hepatitis C or with end-stage liver disease caused by hepatitis C. To minimize false-negative results, serum must be separated from cellular components within 2-4 hours after collection, and preferably stored frozen at -20 C or -70 C (109). If shipping is required, frozen samples should be protected from thawing. Because of assay variability, rigorous quality assurance and control should be in place in clinical laboratories performing this assay, and proficiency testing is recommended. Quantitative assays for measuring the concentration (titer) of HCV RNA have been developed and are available from commercial laboratories (110), including a quantitative RT-PCR (Amplicor HCV MonitorTM, Roche Molecular Systems, Branchburg, New Jersey) and a branched DNA (deoxyribonucleic acid) signal amplification assay (QuantiplexTM HCV RNA Assay {bDNA}, Chiron Corp., Emeryville, California) (Table_2). These assays also are not FDA-approved, and compared with qualitative RT-PCR assays, are less sensitive with lower limits of detection of 500 viral genome copies/mL for the Amplicor HCV MonitorTM to 200,000 genome equivalents/mL for the QuantiplexTM HCV RNA Assay (111). In addition, they each use a different standard, which precludes direct comparisons between the two assays. Quantitative assays should not be used as a primary test to confirm or exclude diagnosis of HCV infection or to monitor the endpoint of treatment. Patients with chronic hepatitis C generally circulate virus at levels of 105-107 genome copies/mL. Testing for level of HCV RNA might help predict likelihood of response to antiviral therapy, although sequential measurement of HCV RNA levels has not proven useful in managing patients with hepatitis C. At least six different genotypes and greater than 90 subtypes of HCV exist (112). Approximately 70% of HCV-infected persons in the United States are infected with genotype 1, with frequency of subtype 1a predominating over subtype 1b. Different nucleic acid detection methods are available commercially to group isolates of HCV, based on genotypes and subtypes (113). Evidence is limited regarding differences in clinical features, disease outcome, or progression to cirrhosis or hepatocellular carcinoma (HCC) among persons with different genotypes. However, differences do exist in responses to antiviral therapy according to HCV genotype. Rates of response in patients infected with genotype 1 are substantially lower than in patients with other genotypes, and treatment regimens might differ on the basis of genotype. Thus, genotyping might be warranted among persons with chronic hepatitis C who are being considered for antiviral therapy. Clinical Features and Natural History Acute HCV Infection Persons with acute HCV infection typically are either asymptomatic or have a mild clinical illness; 60%-70% have no discernible symptoms; 20%-30% might have jaundice; and 10%-20% might have nonspecific symptoms (e.g., anorexia, malaise, or abdominal pain) (13,114,115). Clinical illness in patients with acute hepatitis C who seek medical care is similar to that of other types of viral hepatitis, and serologic testing is necessary to determine the etiology of hepatitis in an individual patient. In less than or equal to 20% of these patients, onset of symptoms might precede anti-HCV seroconversion. Average time period from exposure to symptom onset is 6-7 weeks (116-118), whereas average time period from exposure to seroconversion is 8-9 weeks (114; personal communication, HJ Alter, M.D., Chief, Department of Transfusion Medicine, Clinical Center, National Institutes of Health, Bethesda, MD, September 1998). Anti-HCV can be detected in 80% of patients within 15 weeks after exposure, in greater than or equal to 90% within 5 months after exposure, and in greater than or equal to 97% by 6 months after exposure (14,114). Rarely, seroconversion might be delayed until 9 months after exposure (14,119). The course of acute hepatitis C is variable, although elevations in serum ALT levels, often in a fluctuating pattern, are its most characteristic feature. Normalization of ALT levels might occur and suggests full recovery, but this is frequently followed by ALT elevations that indicate progression to chronic disease (14). Fulminant hepatic failure following acute hepatitis C is rare (120,121). Chronic HCV Infection After acute infection, 15%-25% of persons appear to resolve their infection without sequelae as defined by sustained absence of HCV RNA in serum and normalization of ALT levels (122; personal communication, LB Seeff, M.D., Senior Scientist {Hepatitis C}, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD, July 1998). Chronic HCV infection develops in most persons (75%-85%)(14,122-124), with persistent or fluctuating ALT elevations indicating active liver disease developing in 60%-70% of chronically infected persons (12-15,116,122-124). In the remaining 30%-40% of chronically infected persons, ALT levels are normal. No clinical or epidemiologic features among patients with acute infection have been found to be predictive of either persistent infection or chronic liver disease. Moreover, various ALT patterns have been observed in these patients during follow-up, and patients might have prolonged periods (greater than or equal to 12 months) of normal ALT activity even though they have histologic-confirmed chronic hepatitis (14). Thus, a single ALT determination cannot be used to exclude ongoing hepatic injury, and long-term follow-up of patients with HCV infection is required to determine their clinical outcome or prognosis. The course of chronic liver disease is usually insidious, progressing at a slow rate without symptoms or physical signs in the majority of patients during the first two or more decades after infection. Frequently, chronic hepatitis C is not recognized until asymptomatic persons are identified as HCV-positive during blood-donor screening, or elevated ALT levels are detected during routine physical examinations. Most studies have reported that cirrhosis develops in 10%-20% of persons with chronic hepatitis C over a period of 20-30 years, and HCC in 1%-5%, with striking geographic variations in rates of this disease (124-128). However, when cirrhosis is established, the rate of development of HCC might be as high as 1%-4%/year. In contrast, a study of greater than 200 women 17 years after they received HCV-contaminated Rh factor IG reported that only 2.4% had evidence of cirrhosis and none had died (129). Thus, longer term follow-up studies are needed to assess lifetime consequences of chronic hepatitis C, particularly among those who acquired their infection at young ages. Although factors predicting severity of liver disease have not been well-defined, recent data indicate that increased alcohol intake, being aged greater than 40 years at infection, and being male are associated with more severe liver disease (130). In particular, among persons with alcoholic liver disease and HCV infection, liver disease progresses more rapidly; among those with cirrhosis, a higher risk for development of HCC exists (131). Furthermore, even intake of moderate amounts (greater than 10 g/day) of alcohol in patients with chronic hepatitis C might enhance disease progression. More severe liver injury observed in persons with alcoholic liver disease and HCV infection possibly is attributable to alcohol-induced enhancement of viral replication or increased susceptibility of cells to viral injury. In addition, persons who have chronic liver disease are at increased risk for fulminant hepatitis A (132). Extrahepatic manifestations of chronic HCV infection are considered to be of immunologic origin and include cryoglobulinemia, membranoproliferative glomerulonephritis, and porphyria cutanea tarda (131). Other extrahepatic conditions have been reported, but definitive associations of these conditions with HCV infection have not been established. These include seronegative arthritis, Sjogren syndrome, autoimmune thyroiditis, lichen planus, Mooren corneal ulcers, idiopathic pulmonary fibrosis (Hamman-Rich syndrome), polyarteritis nodosa, aplastic anemia, and B-cell lymphomas. Clinical Management and Treatment HCV-positive patients should be evaluated for presence and severity of chronic liver disease (133). Initial evaluation for presence of disease should include multiple measurements of ALT at regular intervals, because ALT activity fluctuates in persons with chronic hepatitis C. Patients with chronic hepatitis C should be evaluated for severity of their liver disease and for possible treatment (133-135). Antiviral therapy is recommended for patients with chronic hepatitis C who are at greatest risk for progression to cirrhosis (133). These persons include anti-HCV-positive patients with persistently elevated ALT levels, detectable HCV RNA, and a liver biopsy that indicates either portal or bridging fibrosis or at least moderate degrees of inflammation and necrosis. In patients with less severe histologic changes, indications for treatment are less clear, and careful clinical follow-up might be an acceptable alternative to treatment with antiviral therapy (e.g., interferon) because progression to cirrhosis is likely to be slow, if it occurs at all. Similarly, patients with compensated cirrhosis (without jaundice, ascites, variceal hemorrhage, or encephalopathy) might not benefit from interferon therapy. Careful assessment should be made, and the risks and benefits of therapy should be thoroughly discussed with the patient. Patients with persistently normal ALT values should not be treated with interferon outside of clinical trials because treatment might actually induce liver enzyme abnormalities (136). Patients with advanced cirrhosis who might be at risk for decompensation with therapy and pregnant women also should not be treated. Interferon treatment is not FDA-approved for patients aged less than 18 years, and more data are needed regarding treatment of persons aged less than 18 years or greater than 60 years. Treatment of patients who are drinking excessive amounts of alcohol or who are injecting illegal drugs should be delayed until these behaviors have been discontinued for greater than or equal to 6 months. Contraindications to treatment with interferon include major depressive illness, cytopenias, hyperthyroidism, renal transplantation, and evidence of autoimmune disease. Most clinical trials of treatment for chronic hepatitis C have been conducted using alpha-interferon (134,135,137,138). When the recommended regimen of 3 million units administered subcutaneously 3 times/week for 12 months is used, approximately 50% of treated patients have normalization of serum ALT activity (biochemical response), and 33% have a loss of detectable HCV RNA in serum (virologic response) at the end of therapy. However, greater than or equal to 50% of these patients relapse when therapy is stopped. Thus, 15%-25% have a sustained response as measured by testing for ALT and HCV RNA greater than or equal to 1 years after therapy is stopped, many of whom also have histologic improvement. For patients who do not respond by the end of therapy, retreatment with a standard dose of interferon is rarely effective. Patients who have persistently abnormal ALT levels and detectable HCV RNA in serum after 3 months of interferon are unlikely to respond to treatment, and interferon treatment should be discontinued. These persons might be considered for participation in clinical trials of alternative treatments. Decreased interferon response rates (less than 15%) have been found in patients with higher serum HCV RNA titers and HCV genotype 1 (the most common strain of HCV in the United States); however, treatment should not be withheld based solely on these findings. Therapy for hepatitis C is a rapidly changing area of clinical practice. Combination therapy with interferon and ribavirin, a nucleoside analogue, is now FDA-approved for treatment of chronic hepatitis C in patients who have relapsed following interferon treatment and might be approved soon for patients who have not been treated previously. Studies of patients treated with a combination of ribavirin and interferon have demonstrated a substantial increase in sustained response rates, reaching 40%-50%, compared with response rates of 15%-25% with interferon alone (139,140). However, as with interferon alone, combination therapy in patients with genotype 1 is not as successful, and sustained response rates among these patients are still less than 30%. Most patients receiving interferon experience flu-like symptoms early in treatment, but these symptoms diminish with continued treatment. Later side effects include fatigue, bone marrow suppression, and neuropsychiatric effects (e.g., apathy, cognitive changes, irritability, and depression). Interferon dosage must be reduced in 10%-40% of patients and discontinued in 5% -15% because of severe side effects. Ribavirin can induce hemolytic anemia and can be problematic for patients with preexisting anemia, bone marrow suppression, or renal failure. In these patients, combination therapy should be avoided or attempts should be made to correct the anemia. Hemolytic anemia caused by ribavirin also can be life-threatening for patients with ischemic heart disease or cerebral vascular disease. Ribavirin is teratogenic, and female patients should avoid becoming pregnant during therapy. Other treatments, including corticosteroids, ursodiol, and thymosin, have not been effective. High iron levels in the liver might reduce the efficacy of interferon. Use of iron-reduction therapy (phlebotomy or chelation) in combination with interferon has been studied, but results have been inconclusive. Because patients are becoming more interested in alternative therapies (e.g., traditional Chinese medicine, antioxidants, naturopathy, and homeopathy), physicians should be prepared to address questions regarding these topics. Postexposure Prophylaxis and Follow-Up Available data regarding the prevention of HCV infection with IG indicate that IG is not effective for postexposure prophylaxis of hepatitis C (67,141). No assessments have been made of postexposure use of antiviral agents (e.g., interferon) to prevent HCV infection. Mechanisms of the effect of interferon in treating patients with hepatitis C are poorly understood, and an established infection might need to be present for interferon to be an effective treatment (142). As of the publication of this report, interferon is FDA-approved only for treatment of chronic hepatitis C. The immediate postexposure setting provides opportunity to identify persons early in the course of their HCV infection. Studies indicate that interferon treatment begun early in the course of HCV infection is associated with a higher rate of resolved infection (143). However, no data exist indicating that treatment begun during the acute phase of infection is more effective than treatment begun early during the course of chronic HCV infection. In addition, as stated previously, interferon is not FDA-approved for this indication. Determination of whether treatment of HCV infection is more beneficial in the acute phase than in the early chronic phase will require evaluation with well-designed research protocols. PREVENTION AND CONTROL RECOMMENDATIONS Rationale Reducing the burden of HCV infection and HCV-related disease in the United States requires implementation of primary prevention activities that reduce risks for contracting HCV infection and secondary prevention activities that reduce risks for liver and other chronic diseases in HCV-infected persons. In addition, surveillance and evaluation activities are required to determine the effectiveness of prevention programs in reducing incidence of disease, identifying persons infected with HCV, providing appropriate medical follow-up, and promoting healthy lifestyles and behaviors. Primary prevention activities can reduce or eliminate potential risk for HCV transmission from a) blood, blood components, and plasma derivatives; b) such high-risk activities as injecting-drug use and sex with multiple partners; and c) percutaneous exposures to blood in health care and other (i.e., tattooing and body piercing) settings. Immunization against HCV is not available; therefore, identifying persons at risk but not infected with HCV provides opportunity for counseling on how to reduce their risk for becoming infected. Elements of a comprehensive strategy to prevent and control hepatitis C virus (HCV) infection and HCV-related disease
Secondary prevention activities can reduce risks for chronic disease by identifying HCV-infected persons through diagnostic testing and by providing appropriate medical management and antiviral therapy. Because of the number of persons with chronic HCV infection, identification of these persons must be a major focus of current prevention programs. Identification of persons at risk for HCV infection provides opportunity for testing to determine their infection status, medical evaluation to determine their disease status if infected, and antiviral therapy, if appropriate. Identification also provides infected persons opportunity to obtain information concerning how they can prevent further harm to their liver and prevent transmitting HCV to others. Factors for consideration when making decisions regarding development and implementation of preventive services for a particular disease include the public health importance of the disease, the availability of appropriate diagnostic tests, and the effectiveness of available preventive and therapeutic interventions. However, identification of persons at risk for HCV infection must take into account not only the benefits but also the limitations and drawbacks associated with such efforts. Hepatitis C is a disease of major public health importance, and suitable and accurate diagnostic tests as well as behavioral and therapeutic interventions are available. Counseling and testing can prevent disease transmission and progression through reducing high-risk practices (e.g., injecting-drug use and alcohol intake). However, the degree to which persons will change their high-risk practices based on knowing their test results is not known, and possible adverse consequences of testing exist, including disclosure of test results to others that might result in disrupted personal relationships and possible discriminatory action (e.g., loss of employment, insurance, and educational opportunities). Antiviral treatment is also available, and treatment guidelines have been developed. Such treatment is beneficial for many patients, although sustained response rates and mode of delivery are currently less than ideal. Persons at risk for HCV infection who receive health-care services in the public and private sectors should have access to counseling and testing. Facilities that provide counseling and testing should include services or referrals for medical evaluation and management of persons identified as infected with HCV. Priorities for implementing new counseling and testing programs should be based on providing access to persons who are most likely to be infected or who practice high-risk behaviors. PRIMARY PREVENTION RECOMMENDATIONS Blood, Plasma Derivatives, Organs, Tissues, and Semen Current practices that exclude blood, plasma, organ, tissue, or semen donors determined to be at increased risk for HCV by history or who have serologic markers for HCV infection must be maintained to prevent HCV transmission from transfusions and transplants (1). Viral inactivation of clotting factor concentrates and other products derived from human plasma, including IG products, also must be continued, and all plasma-derived products that do not undergo viral inactivation should be HCV RNA negative by RT-PCR before release. High-Risk Drug and Sexual Practices Health-care professionals in all patient care settings routinely should obtain a history that inquires about use of illegal drugs (injecting and noninjecting) and evidence of high-risk sexual practices (e.g., multiple sex partners or a history of STDs). Primary prevention of illegal drug injecting will eliminate the greatest risk factor for HCV infection in the United States (144). Although consistent data are lacking regarding the extent to which sexual activity contributes to HCV transmission, persons having multiple sex partners are at risk for STDs (e.g., HIV, HBV, syphilis, gonorrhea, and chlamydia). Counseling and education to prevent initiation of drug-injecting or high-risk sexual practices is important, especially for adolescents. Persons who inject drugs or who are at risk for STDs should be counseled regarding what they can do to minimize their risk for becoming infected or of transmitting infectious agents to others, including need for vaccination against hepatitis B (144-148). Injecting and noninjecting illegal drug users and sexually active MSM also should be vaccinated against hepatitis A (149). Prevention messages for persons with high-risk drug or sexual practices
use or high-risk sexual practices should be conducted in the setting in which the patient is identified. If counseling services cannot be provided on-site, patients should be referred to a convenient community resource, or at a minimum, provided easy-to-understand health-education material. STD and drug-treatment clinics, correctional institutions, and HIV counseling and testing sites should routinely provide information concerning prevention of HCV and HBV infection in their counseling messages. Based on the findings of multiple studies, syringe and needle-exchange programs can be an effective part of a comprehensive strategy to reduce the incidence of bloodborne virus transmission and do not encourage the use of illegal drugs (150-153). Therefore, to reduce the risk for HCV infection among injecting-drug users, local communities can consider implementing syringe and needle-exchange programs. Percutaneous Exposures to Blood in Health Care and Other Settings Health-Care Settings Health-care, emergency medical, and public safety workers should be educated regarding risk for and prevention of bloodborne infections, including the need to be vaccinated against hepatitis B (154-156). Standard barrier precautions and engineering controls should be implemented to prevent exposure to blood. Protocols should be in place for reporting and follow-up of percutaneous or permucosal exposures to blood or body fluids that contain blood. Health-care professionals responsible for overseeing patients receiving home infusion therapy should ensure that patients and their families (or caregivers) are informed of potential risk for infection with bloodborne pathogens, and should assess their ability to use adequate infection-control practices consistently (88). Patients and families should receive training with a standardized curriculum that includes appropriate infection-control procedures, and these procedures should be evaluated regularly through home visits. Currently, no recommendations exist to restrict professional activities of health-care workers with HCV infection. As recommended for all health-care workers, those who are HCV-positive should follow strict aseptic technique and standard precautions, including appropriate use of hand washing, protective barriers, and care in the use and disposal of needles and other sharp instruments (154,155). In chronic hemodialysis settings, intensive efforts must be made to educate new staff and reeducate existing staff regarding hemodialysis-specific infection-control practices that prevent transmission of HCV and other bloodborne pathogens (65,157). Hemodialysis-center precautions are more stringent than standard precautions. Standard precautions require use of gloves only when touching blood, body fluids, secretions, excretions, or contaminated items. In contrast, hemodialysis-center precautions require glove use whenever patients or hemodialysis equipment is touched. Standard precautions do not restrict use of supplies, instruments, and medications to a single patient; hemodialysis-center precautions specify that none of these items be shared among any patients. Thus, appropriate use of hemodialysis-center precautions should prevent transmission of HCV among chronic hemodialysis patients, and isolation of HCV-positive patients is not necessary or recommended. Routine precautions for the care of all hemodialysis patients
Other Settings Persons who are considering tattooing or body piercing should be informed of potential risks of acquiring infection with bloodborne and other pathogens through these procedures. These procedures might be a source of infection if equipment is not sterile or if the artist or piercer does not follow other proper infection-control procedures (e.g., washing hands, using latex gloves, and cleaning and disinfecting surfaces). SECONDARY PREVENTION RECOMMENDATIONS Persons for Whom Routine HCV Testing Is Recommended Testing should be offered routinely to persons most likely to be infected with HCV who might require medical management, and testing should be accompanied by appropriate counseling and medical follow-up. In addition, anyone who wishes to know or is concerned regarding their HCV-infection status should be provided the opportunity for counseling, testing, and appropriate follow-up. The determination of which persons at risk to recommend for routine testing is based on various considerations, including a known epidemiologic relationship between a risk factor and acquiring HCV infection, prevalence of risk behavior or characteristic in the population, prevalence of infection among those with a risk behavior or characteristic, and the need for persons with a recognized exposure to be evaluated for infection. Persons who should be tested routinely for hepatitis C virus (HCV) infection based on their risk for infection
Persons who should be tested routinely for HCV-infection based on a recognized exposure Persons Who Have Ever Injected Illegal Drugs Health-care professionals in primary-care and other appropriate settings routinely should question patients regarding their history of injecting-drug use, and should counsel, test, and evaluate for HCV infection, persons with such histories. Current injecting-drug users frequently are not seen in the primary health-care setting and might not be reached by traditional media; therefore, community-based organizations serving these populations should determine the most effective means of integrating appropriate HCV information and services into their programs. Testing persons in settings with potentially high proportions of injecting-drug users (e.g., correctional institutions, HIV counseling and testing sites, or drug and STD treatment programs) might be particularly efficient for identifying HCV-positive persons. HCV testing programs in these settings should include counseling and referral or arrangements for medical management. However, limited experience exists in combining HCV programs with existing HIV, STD, or other established services for populations at high risk for infection with bloodborne pathogens. Persons at risk for HCV infection through limited or occasional drug use, particularily in the remote past, might not be receptive to receiving services in such settings as HIV counseling and testing sites and drug and STD treatment programs. In addition, whether a substantial proportion of this group at risk can be identified in these settings is unknown. Studies are needed to determine the best approaches for reaching persons who might not identify themselves as being at risk for HCV infection. Persons with Selected Medical Conditions Persons with hemophilia who received clotting factor concentrates produced before 1987 and long-term hemodialysis patients should be tested for HCV infection. Educational efforts directed to health-care professionals, patient organizations, and agencies who care for these patients should emphasize the need for these patients to know whether they are infected with HCV and encourage testing for those who have not been tested previously. Periodic testing of long-term hemodialysis patients for purposes of infection control is currently not recommended (61). However, issues surrounding prevention of HCV and other bloodborne pathogen transmission in long-term hemodialysis settings are currently undergoing discussion, and updating recommendations for this setting is under development. Persons with persistently abnormal ALT levels are often identified in medical settings. As part of their medical work-up, health-care professionals should test routinely for HCV infection persons with ALT levels above the upper limit of normal on at least two occasions. Persons with other evidence of liver disease identified by abnormal serum aspartate aminotransferase (AST) levels, which is common among persons with alcohol-related liver disease, should be tested also. Prior Recipients of Blood Transfusions or Organ Transplants Persons who might have become infected with HCV through transfusion of blood and blood components should be notified. Two types of approaches should be used -- a) a targeted, or directed, approach to identify prior transfusion recipients from donors who tested anti-HCV positive after multiantigen screening tests were widely implemented (July 1992 and later); and b) a general approach to identify all persons who received transfusions before July 1992. A targeted notification approach focuses on a specific group known to be at risk, and will reach persons who might be unaware they were transfused. However, because blood and blood-component donor testing for anti-HCV before July 1992 did not include confirmatory testing, most of these notifications would be based on donors who were not infected with HCV because their test results were falsely positive. A general education campaign to identify persons transfused before July 1992 has the advantage of not being dependent on donor testing status or availability of records, and potentially reaches persons who received HCV-infected blood from donors who tested falsely negative on the less sensitive serologic test, as well as from donors before testing was available.
Blood-collection establishments and transfusion services should work with local and state health agencies to coordinate this notification effort. Health-care professionals should have information regarding the notification process and HCV infection so that they are prepared to discuss with their patients why they were notified and to provide appropriate counseling, testing, and medical evaluation. Health-education material sent to recipients should be easy to understand and include information concerning where they can be tested, what hepatitis C means in terms of their day-to-day living, and where they can obtain more information.
Health-Care, Emergency Medical, and Public Safety Workers After Needle Sticks, Sharps, or Mucosal Exposures to HCV-Positive Blood Individual institutions should establish policies and procedures for HCV testing of persons after percutaneous or permucosal exposures to blood and ensure that all personnel are familiar with these policies and procedures (see text box on next page) (141). Health-care professionals who provide care to persons exposed to HCV in the occupational setting should be knowledgeable regarding the risk for HCV infection and appropriate counseling, testing, and medical follow-up. IG and antiviral agents are not recommended for postexposure prophylaxis of hepatitis C. Limited data indicate that antiviral therapy might be beneficial when started early in the course of HCV infection, but no guidelines exist for administration of therapy during the acute phase of infection. When HCV infection is identified early, the individual should be referred for medical management to a specialist knowledgeable in this area. Children Born to HCV-Positive Women Because of their recognized exposure, children born to HCV-positive women should be tested for HCV infection (158). IG and antiviral agents are not recommended for postexposure prophylaxis of infants born to HCV-positive women. Testing of infants for anti-HCV should be performed no sooner than age 12 months, when passively transferred maternal anti-HCV declines below detectable levels. If earlier diagnosis of HCV infection is desired, RT-PCR for HCV RNA may be performed at or after the infant's first well-child visit at age 1-2 months. Umbilical cord blood should not be used for diagnosis of perinatal HCV infection because cord blood can be contaminated by maternal blood. If positive for either anti-HCV or HCV RNA, children should be evaluated for the presence or development of liver disease, and those children with persistently elevated ALT levels should be referred to a specialist for medical management. Postexposure follow-up of health-care, emergency medical, and public safety workers for hepatitis C virus (HCV) infection
Persons for Whom Routine HCV Testing Is Not Recommended For the following persons, routine testing for HCV infection is not recommended unless they have risk factors for infection. Persons for whom routine hepatitis C virus (HCV) testing is not recommended
Health-Care, Emergency Medical, and Public Safety Workers Routine testing is recommended only for follow-up for a specific exposure. Pregnant Women Health-care professionals in settings where pregnant women are evaluated or receive routine care should take risk histories from their patients designed to determine the need for testing and other prevention measures, and those health-care professionals should be knowledgeable regarding HCV counseling, testing, and medical follow-up. Household (Nonsexual) Contacts of HCV-Positive Persons Routine testing for nonsexual household contacts of HCV-positive persons is not recommended unless a history exists of a direct (percutaneous or mucosal) exposure to blood. Persons for Whom Routine HCV Testing Is of Uncertain Need For persons at potential (or unknown) risk for HCV infection, the need for, or effectiveness of, routine testing has not been determined. Persons for whom routine hepatitis C virus (HCV) testing is of uncertain need
Recipients of Transplanted Tissue On the basis of currently available data, risk for HCV transmission from transplanted tissue (e.g., corneal, musculoskeletal, skin, ova, or sperm) appears to be rare. Intranasal Cocaine and Other Noninjecting Illegal Drug Users Currently, the strength of the association between intranasal cocaine use and HCV infection does not support routine testing based solely on this risk factor. Persons with a History of Tattooing or Body Piercing Because no data exist in the United States documenting that persons with a history of such exposures as tattooing and body piercing are at increased risk for HCV infection, routine testing is not recommended based on these exposures alone. In settings having a high proportion of HCV-infected persons and where tattooing and body piercing might be performed in an unregulated manner (e.g., correctional institutions), these types of exposures might be a risk factor for HCV infection. Data are needed to determine the risk for HCV infection among persons who have been exposed under these conditions. Persons with a History of Multiple Sex Partners or STDs Although persons with a history of multiple sex partners or treatment for STDs and who deny injecting-drug use appear to have an increased risk for HCV infection, insufficient data exist to recommend routine testing based on these histories alone. Health-care professionals who provide services to persons with STDs should use that opportunity to take complete risk histories from their patients to ascertain the need for HCV testing, provide risk-reduction counseling, offer hepatitis B vaccination, and, if appropriate, hepatitis A vaccination. Long-Term Steady Sex Partners of HCV-Positive Persons HCV-positive persons with long-term steady partners do not need to change their sexual practices. Persons with HCV infection should discuss with their partner the need for counseling and testing. If the partner chooses to be tested and tests negative, the couple should be informed of available data regarding risk for HCV transmission by sexual activity to assist them in making decisions about precautions (see section regarding counseling messages for HCV-positive persons). If the partner tests positive, appropriate counseling and evaluation for the presence or development of liver disease should be provided. Testing for HCV Infection Consent for testing should be obtained in a manner consistent with that for other medical care and services provided in the same setting, and should include measures to prevent unwanted disclosure of test results to others. Persons should be provided with information regarding
Comprehensive information regarding hepatitis C should be provided before testing; however, this might not be practical when HCV testing is performed as part of a clinical work-up or when testing for anti-HCV is required. In these cases, persons should be informed that a) testing for HCV infection will be performed, b) individual results will be kept confidential, and c) appropriate counseling and referral will be offered if results are positive. Testing for HCV infection can be performed in various settings, including physicians' offices, other health-care facilities, health department clinics, and HIV or other freestanding counseling and testing sites. Such settings should be prepared to provide appropriate information regarding hepatitis C and provide or offer referral for additional medical care or other needed services (e.g., drug treatment), as warranted. Facilities providing HCV testing should have access to information regarding referral resources, including availability, accessibility, and eligibility criteria of local medical care and mental health professionals, support groups, and drug-treatment centers. The diagnosis of HCV infection can be made by detecting either anti-HCV or HCV RNA. Anti-HCV is recommended for routine testing of asymptomatic persons, and should include use of both EIA to test for anti-HCV and supplemental or confirmatory testing with an additional, more specific assay (Figure_3). Use of supplemental antibody testing (i.e., RIBATM) for all positive anti-HCV results by EIA is preferred, particularly in settings where clinical services are not provided directly. Supplemental anti-HCV testing confirms the presence of anti-HCV (i.e., eliminates false-positive antibody results), which indicates past or current infection, and can be performed on the same serum sample collected for the EIA (i.e., routine serology). Confirmation or exclusion of HCV infection in a person with indeterminate anti-HCV supplemental test results should be made on the basis of further laboratory testing, which might include repeating the anti-HCV in two or more months or testing for HCV RNA and ALT level. In clinical settings, use of RT-PCR to detect HCV RNA might be appropriate to confirm the diagnosis of HCV infection (e.g., in patients with abnormal ALT levels or with indeterminate supplemental anti-HCV test results) although RT-PCR assays are not currently FDA-approved. Detection of HCV RNA by RT-PCR in a person with an anti-HCV-positive result indicates current infection. However, absence of HCV RNA in a person with an anti-HCV-positive result based on EIA testing alone (i.e., without supplemental anti-HCV testing) cannot differentiate between resolved infection and a false-positive anti-HCV test result. In addition, because some persons with HCV infection might experience intermittent viremia, the meaning of a single negative HCV RNA result is difficult to interpret, particularly in the absence of additional clinical information. If HCV RNA is used to confirm anti-HCV results, a separate serum sample will need to be collected and handled in a manner suitable for RT-PCR. If the HCV RNA result is negative, supplemental anti-HCV testing should be performed so that the anti-HCV EIA result can be interpreted before the result is reported to the patient. Laboratories that perform HCV testing should follow the recommended anti-HCV testing algorithm, which includes use of supplemental testing. Having assurances that the HCV testing is performed in accredited laboratories whose services adhere to recognized standards of good laboratory practice is also necessary. Laboratories that perform HCV RNA testing should review routinely their data regarding internal and external proficiency testing because of great variability in accuracy of HCV RNA testing. Prevention Messages and Medical Evaluation HCV-specific information and prevention messages should be provided to infected persons and individuals at risk by trained personnel in public and private health-care settings. Health-education materials should include a) general information about HCV infection; b) risk factors for infection, transmission, disease progression, and treatment; and c) detailed prevention messages appropriate for the population being tested. Written materials might also include information about community resources available for HCV-positive patients for medical evaluation and social support, as appropriate. Persons with High-Risk Drug and Sexual Practices Regardless of test results, persons who use illegal drugs or have high-risk sexual practices or occupations should be provided with information regarding how to reduce their risk for acquiring bloodborne and sexually transmitted infections or of potentially transmitting infectious agents to others (see section regarding primary prevention). Negative Test Results If their exposure was in the past, persons who test negative for HCV should be reassured. Indeterminate Test Results Persons whose HCV test results are indeterminate should be advised that the result is inconclusive, and they should receive appropriate follow-up testing or referral for further testing (see section regarding testing for HCV infection). Positive Test Results Persons who test positive should be provided with information regarding the need for a) preventing further harm to their liver; b) reducing risks for transmitting HCV to others; and c) medical evaluation for chronic liver disease and possible treatment.
NIH Consensus Statement Regarding Management of Hepatitis C (Excerpted) The NIH "Consensus Statement on Management of Hepatitis C" was based on data available in March 1997 (133). Because of advances in the field of antiviral therapy for chronic hepatitis C, standards of practice might change, and readers should consult with specialists knowledgeable in this area. Persons Recommended for Treatment Treatment is recommended for patients with chronic hepatitis C who are at greatest risk for progression to cirrhosis, as characterized by
Persons for Whom Treatment Is Unclear Included are
Persons for Whom Treatment Is Not Recommended Included are
PUBLIC HEALTH SURVEILLANCE The objectives of conducting surveillance for hepatitis C are to
Various surveillance approaches are required to achieve these objectives because of limitations of diagnostic tests for HCV infection, the number of asymptomatic patients with acute and chronic disease, and the long latent period between infection and chronic disease outcome. Surveillance for Acute Hepatitis C Surveillance for acute hepatitis C -- new, symptomatic infections -- provides the information necessary for determining incidence trends, changing patterns of transmission and persons at highest risk for infection. In addition, surveillance for new cases provides the best means to evaluate effectiveness of prevention efforts and to identify missed opportunities for prevention. Acute hepatitis C is one of the diseases mandated by the Council of State and Territorial Epidemiologists (CSTE) for reporting to CDC's National Notifiable Diseases Surveillance System. However, hepatitis C reporting has been unreliable to date because most health departments do not have the resources required for case investigations to determine if a laboratory report represents acute infection, chronic infection, repeated testing of a person previously reported, or a false-positive result. Historically, the most reliable national data regarding acute disease incidence and transmission patterns have come from sentinel surveillance (i.e., sentinel counties study of acute viral hepatitis). As hepatitis C prevention and control programs are implemented, federal, state, and local agencies will need to determine the best methods to effectively monitor new disease acquisition. Laboratory Reports of Anti-HCV-Positive Tests Although limitations exist for the use of anti-HCV-positive laboratory reports to identify new cases and to monitor trends in disease incidence, they potentially are an important source from which state and local health departments can identify infected persons who need counseling and medical follow-up. Development of registries of persons with anti-HCV-positive laboratory results might facilitate efforts to provide counseling and medical follow-up and these registries could be used to provide local, state, and national estimates of the proportion of persons with HCV infection who have been identified. If such registries are developed, the confidentiality of individual identifying information should be ensured according to applicable laws and regulations. Serologic Surveys Serologic surveys at state and local levels can characterize regional and local variations in prevalence of HCV infection, identify populations at high risk, monitor trends, and evaluate prevention programs. Existing laboratory-based reporting of HCV-positive test results cannot provide this information because persons who are tested will not be representative of the population as a whole, and certain populations at high risk might be underrepresented. Thus, data from newly designed or existing serologic surveys will be needed to monitor trends in HCV infection and evaluate prevention programs at state and local levels. Surveillance for Chronic Liver Disease Surveillance for HCV-related chronic liver disease can provide information to measure the burden of disease, determine natural history and risk factors, and evaluate the effect of therapeutic and prevention measures on incidence and severity of disease. Until recently, no such surveillance existed, but a newly established sentinel surveillance pilot program for physician-diagnosed chronic liver disease will provide baseline data and a template for a comprehensive sentinel surveillance system for chronic liver disease. As the primary source of data regarding the incidence and natural history of chronic liver disease, this network will be pivotal for monitoring the effects of education, counseling, other prevention programs, and newly developed therapies on the burden of the disease. FUTURE DIRECTIONS To prevent chronic HCV infection and its sequelae, prevention of new HCV infections should be the primary objective of public health activities. Achieving this objective will require the integration of HCV prevention and surveillance activities into current public health infrastructure. In addition, several questions concerning the epidemiology of HCV infection remain, and the answers to those questions could change or modify primary prevention activities. These questions primarily concern the magnitude of the risk attributable to sexual transmission of HCV and to illegal noninjecting-drug use. Identification of the large numbers of persons in the United States with chronic HCV infection is resource-intensive. The most efficient means to achieve this identification is unknown, because the prevention effectiveness of various implementation strategies has not been evaluated. However, widespread programs to identify, counsel, and treat HCV-infected persons, combined with improvements in the efficacy of treatment, are expected to lower the morbidity and mortality from HCV-related chronic liver disease substantially. Monitoring the progress of these activities to determine their effectiveness in achieving a reduction in HCV-related chronic disease is important. References
* Sentinel counties viral hepatitis surveillance system identifies all persons w symptomatic acute viral hepatitis reported through stimulated passive surveillan participating county health departments (four during 1982-1995 and six during 19 These counties are demographically representative of the U.S. population. Serum from reported cases are tested for all viral hepatitis markers, and case-patient interviewed extensively for risk factors for infection. Figure_1 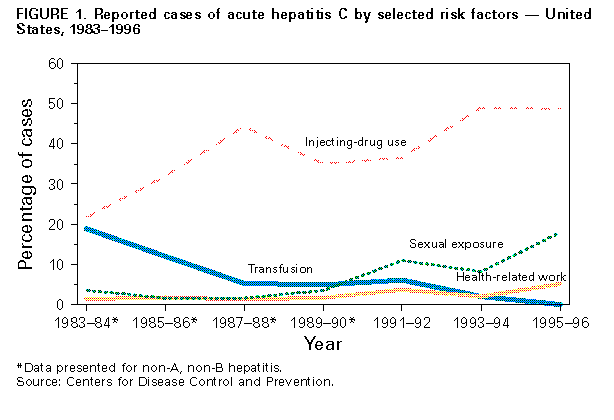 Return to top. Figure_2  Return to top. Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 1. Estimated average prevalence of hepatitis C virus (HCV) infection in the United States by various characteristics
and estimated prevalence of persons with these characteristics in the population
==============================================================================================================================
HCV-infection
prevalence
------------------------- Prevalence of persons
Characteristic % (range, %) with characteristic, %
------------------------------------------------------------------------------------------------------------------------------
Persons with hemophilia treated with products made before 87 (74-90) <0.01
1987
Injecting-drug users
current 79 (72-86) 0.5
history of prior use No Data 5
Persons with abnormal alanine aminotransferase levels 15 (10-18) 5
Chronic hemodialysis patients 10 (0-64) 0.1
Persons with multiple sex partners (lifetime)
>=50 9 (6-16) 4
10-49 3 (3-4) 22
2-9 2 (1-2) 52
Persons reporting a history of sexually transmitted diseases 6 (1-10) 17
Persons receiving blood transfusions before 1990 6 (5-9) 6
Infants born to infected mothers 5 (0-25) 0.1
Men who have sex with men 4 (2-18) 5
General population 1.8 (1.5-2.3) NA*
Health-care workers 1 (1-2) 9
Pregnant women 1 -- 1.5
Military personnel 0.3 (0.2-0.4) 0.5
Volunteer blood donors 0.16 -- 5
------------------------------------------------------------------------------------------------------------------------------
* Not applicable.
==============================================================================================================================
Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
TABLE 2. Tests for hepatitis C virus (HCV) infection
==========================================================================================================================================================
Test/Type Application Comments
----------------------------------------------------------------------------------------------------------------------------------------------------------
-- Hepatitis C virus antibody (anti-HCV)
-- EIA (enzyme immunoassay) -- Indicates past or present infection but does -- Sensitivity >=97%
not differentiate between acute chronic or -- EIA alone has low-positive
resolved infection predictive value in low-
-- All positive EIA results should be verified with prevalence population
a supplemental assay
HCV RNA (hepatitis C virus ribonucleic acid)
Qualitative tests*+
-- Reverse transcriptase polymerase chain -- Detect presence of circulating HCV RNA -- Detect virus as early as 1-2
reaction (RT-PCR) amplification of HCV RNA by -- Monitor patients on antiviral therapy weeks after exposure
in-house or commercial assays (e.g. Amplicor -- Detection of HCV RNA during
HCV) course of infection might be intermittent;
a single negative RT-PCR is not conclusive
-- False-positive and false-
negative results might occur
Quantitative tests*+
-- RT-PCR amplification of HCV RNA by in-house or -- Determine concentration of HCV RNA -- Less sensitive than qualitative
commercial assays (e.g. Amplicor HCV Monitor) -- Might be useful for assessing the RT-PCR
-- Branched chain DNA& (bDNA) assays likelihood of response to antiviral -- Should not be used to exclude the diagnosis
(e.g., Quantiplex HCV RNA Assay) of HCV infection or to determine treatment
endpoint
Genotype*+
-- Several methodologies available (e.g. -- Group isolates of HCV based on genetic -- Genotype 1 (subtypes 1a and 1b)
hybridization sequencing) differences into 6 genotypes and >90 subtypes most common in United States and
-- With new therapies, length of treatment associated with lower response
might vary based on genotype to antiviral activity
Serotype*
-- EIA based on immunoreactivity to synthetic -- No clinical utility -- Cannot distinguish between
peptides (e.g. Murex HCV Serotyping 1-6 Assay) subtypes
----------------------------------------------------------------------------------------------------------------------------------------------------------
* Currently not U.S. Food and Drug Administration approved; lack standardization.
+ Samples require special handling (e.g., serum must be separated within 2-4 hours of collection and stored frozen {-20 C or -70C};
frozen samples should be shipped on dry ice).
& Deoxyribonucleic acid.
==========================================================================================================================================================
Return to top. Figure_3 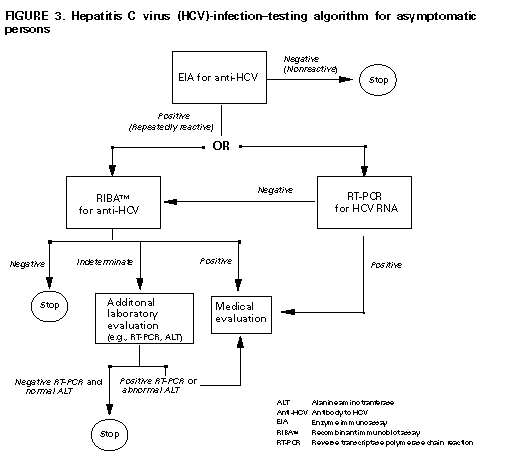 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/10/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}
{kind=link}