|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
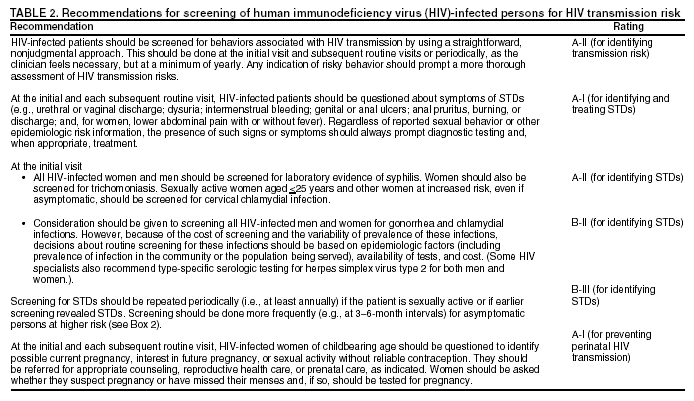
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Incorporating HIV Prevention into the Medical Care of Persons Living with HIVRecommendations of CDC, the Health Resources and Services Administration, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of AmericaPlease note: An erratum has been published for this article. To view the erratum, please click here and an update has been published for this report. To view the update, please click here. The material in this report originated in the National Center for HIV, STD and TB Prevention, Harold W. Jaffe, M.D., Director; Division of HIV/AIDS Prevention — Surveillance and Epidemiology, Robert S. Janssen, Director; Division of HIV/AIDS Prevention — Intervention, Research, and Support, Robert S. Janssen, M.D., Acting Director. Summary Reducing transmission of human immunodeficiency virus (HIV) in the United States requires new strategies, including emphasis on prevention of transmission by HIV-infected persons. Through ongoing attention to prevention, risky sexual and needle-sharing behaviors among persons with HIV infection can be reduced and transmission of HIV infection prevented. Medical care providers can substantially affect HIV transmission by screening their HIV-infected patients for risk behaviors; communicating prevention messages; discussing sexual and drug-use behavior; positively reinforcing changes to safer behavior; referring patients for services such as substance abuse treatment; facilitating partner notification, counseling, and testing; and identifying and treating other sexually transmitted diseases (STDs). To help incorporate HIV prevention into the medical care of HIV-infected persons, CDC, the Health Resources and Services Administration, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America developed these recommendations. The recommendations are general and apply to incorporating HIV prevention into the medical care of all HIV-infected adolescents and adults, regardless of age, sex, or race/ethnicity. They are intended for all persons who provide medical care to HIV-infected persons (e.g., physicians, nurse practitioners, nurses, physician assistants); they might also be useful to those who deliver prevention messages (e.g., case managers, social workers, health educators). The recommendations were developed by using an evidence-based approach. For each recommendation, the strength of the recommendation, the quality of available evidence supporting the recommendation, and the outcome for which the recommendation is rated are provided. The recommendations are categorized into three major components: screening for HIV transmission risk behaviors and STDs, providing brief behavioral risk-reduction interventions in the office setting and referring selected patients for additional prevention interventions and other related services, and facilitating notification and counseling of sex and needle-sharing partners of infected persons. IntroductionDespite substantial advances in the treatment of human immunodeficiency virus (HIV) infection, the estimated number of annual new HIV infections in the United States has remained at 40,000 for over 10 years (1). HIV prevention in this country has largely focused on persons who are not HIV infected, to help them avoid becoming infected. However, further reduction of HIV transmission will require new strategies, including increased emphasis on preventing transmission by HIV-infected persons (2,3). HIV-infected persons who are aware of their HIV infection tend to reduce behaviors that might transmit HIV to others (4--7). Nonetheless, recent reports suggest that such behavioral changes often are not maintained and that a substantial number of HIV-infected persons continue to engage in behaviors that place others at risk for HIV infection (8--13). Reversion to risky sexual behavior might be as important in HIV transmission as failure to adopt safer sexual behavior immediately after receiving a diagnosis of HIV (14). Unprotected anal sex appears to be occurring more frequently in some urban centers, particularly among young men who have sex with men (MSM) (15). Bacterial and viral sexually transmitted diseases (STDs) in HIV-infected men and women receiving outpatient care have been increasingly noted (16,17), indicating ongoing risky behaviors and opportunities for HIV transmission. Further, despite declining syphilis prevalence in the general U.S. population, sustained outbreaks of syphilis among MSM, many of whom are HIV infected, continue to occur in some areas; rates of gonorrhea and chlamydial infection have also risen for this population (18--21). Rising STD rates among MSM indicate increased potential for HIV transmission, both because these rates suggest ongoing risky behavior and because STDs have a synergistic effect on HIV infectivity and susceptibility (22). Studies suggest that optimism about the effectiveness of highly active antiretroviral therapy (HAART) for HIV may be contributing to relaxed attitudes toward safer sex practices and increased sexual risk-taking by some HIV-infected persons (12,23--27). Injection drug use also continues to play a key role in the HIV epidemic; at least 28% of AIDS cases among adults and adolescents with known HIV risk category reported to CDC in 2000 were associated with injection drug use (28). In some large drug-using communities, HIV seroincidence and seroprevalence among injection drug users (IDUs) have declined in recent years (29,30). This decline has been attributed to several factors, including increased use of sterile injection equipment, declines in needle-sharing, shifts from injection to noninjection methods of using drugs, and cessation of drug use (31--33). However, injection-drug use among young adult heroin users has increased substantially in some areas (34,35), a reminder that, as with sexual behaviors, changes to less risky behaviors may be difficult to sustain. Clinicians providing medical care to HIV-infected persons can play a key role in helping their patients reduce risk behaviors and maintain safer practices and can do so with a feasible level of effort, even in constrained practice settings. Clinicians can greatly affect patients' risks for transmission of HIV to others by performing a brief screening for HIV transmission risk behaviors; communicating prevention messages; discussing sexual and drug-use behavior; positively reinforcing changes to safer behavior; referring patients for such services as substance abuse treatment; facilitating partner notification, counseling, and testing; and identifying and treating other STDs (36,37). These measures may also decrease patients' risks of acquiring other STDs and bloodborne infections (e.g., viral hepatitis). Managed care plans can play an important role in HIV prevention by incorporating these recommendations into their practice guidelines, educating their providers and enrollees, and providing condoms and educational materials. In the context of care, prevention services might be delivered in clinic or office environments or through referral to community-based programs. Some clinicians have expressed concern that reimbursement is often not provided for prevention services and note that improving reimbursement for such services might enhance the adoption and implementation of these guidelines. This report provides general recommendations for incorporating HIV prevention into the medical care of all HIV-infected adolescents and adults, regardless of age, sex, or race/ethnicity. The recommendations are intended for all persons who provide medical care to HIV-infected persons (e.g., physicians, nurse practitioners, nurses, physician assistants). They may also be useful to those who deliver prevention messages (e.g., case managers, social workers, health educators). Special considerations may be needed for some subgroups (e.g., adolescents, for whom laws and regulations might exist governing providing of services to minors, the need to obtain parental consent, or duty to inform). However, it is beyond the scope of this report to address special considerations of subgroups. Furthermore, the recommendations focus on sexual and drug-injection behaviors, since these behaviors are responsible for nearly all HIV transmission in the United States. Separate guidelines have been published for preventing perinatal transmission (38--40). These recommendations were developed by using an evidence-based approach (Table 1). The strength of each recommendation is indicated on a scale of A (strongest recommendation for) to E (recommendation against); the quality of available evidence supporting the recommendation is indicated on a scale of I (strongest evidence for) to III (weakest evidence for), and the outcome for which the recommendation is rated is provided. The recommendations are categorized into three major components: 1) screening for HIV transmission risk behaviors and STDs, 2) providing brief behavioral risk-reduction interventions in the office setting and referring selected patients for additional prevention interventions and other related services, and 3) facilitating notification and counseling of sex and needle-sharing partners of infected persons. This report was developed by CDC, the Health Resources and Services Administration (HRSA), the National Institutes of Health (NIH), and the HIV Medicine Association (HIVMA) of the Infectious Diseases Society of America (IDSA). The recommendations will evolve as results from ongoing behavioral intervention trials become available. Risk ScreeningRisk screening is a brief assessment of behavioral and clinical factors associated with transmission of HIV and other STDs (Table 2). Risk screening can be used to identify patients who should receive more in-depth risk assessment and HIV risk-reduction counseling, other risk-reduction interventions, or referral for other services (e.g., substance abuse treatment). Risk screening identifies patients at greatest risk for transmitting HIV so that prevention and referral recommendations can be focused on these patients. Screening methods include probing for behaviors associated with transmission of HIV and other STDs, eliciting patient reports of symptoms of other STDs, and laboratory testing for other STDs. Although each of these methods has limitations, a combination of methods should increase the sensitivity and effectiveness of screening. In conducting risk screening, clinicians should recognize that risk is not static. Patients' lives and circumstances change, and a patient's risk of transmitting HIV may change from one medical encounter to another. Also, clinicians should recognize that working with adolescents may require special approaches and should be aware of and adhere to all laws and regulations related to providing services to minors. Screening for Behavioral Risk FactorsClinicians frequently believe that patients are uncomfortable disclosing personal risks and hesitant to respond to questions about sensitive issues, such as sexual behaviors and illicit drug use. However, available evidence suggests that patients, when asked, will often disclose their risks (41,42) and that some patients have reported greater confidence in their clinician's ability to provide high-quality care if asked about sexual and STD history during the initial visits (43). Screening for behavioral risk factors can be done with brief self-administered written questionnaires; computer-, audio-, and video-assisted questionnaires; structured face-to-face interviews; and personalized discussions (41,44--53). Screening questions can be either open-ended or closed (directed) (Box 1). Use of open-ended questions avoids simple "yes" or "no" responses and encourages patients to discuss personal risks and the circumstances in which risks occur (15,44,54). Open-ended questions also help the clinician gather enough detail to understand potential transmission risks and make more meaningful recommendations. However, although well received by patients, the open-ended approach may initially be difficult for clinicians schooled in directed questioning, who tend to prefer directed screening questions. Directed questions are probably useful for identifying patients with problems that should be more thoroughly discussed. Among directed approaches, technical tools like computer-, audio-, and video-assisted interviews have been found to elicit more self-reported risk behaviors than did interviewer-administered questionnaires, particularly among younger patients (41,51--53,55). Studies suggest that clinicians who receive some training, particularly that including role-play and feedback concerning clinical performance, are more likely to perform effective risk screening (46--49). Sex-related behaviors important to address in risk screening include whether the patient has been engaging in sex; number and sex of partners; partners' HIV serostatus (infected, not infected, or unknown); types of sexual activity (oral, vaginal, or anal sex) and whether condoms are used; and barriers to abstinence or correct condom use (e.g., difficulty talking with partners about or disclosing HIV serostatus, alcohol and other drug use before or during sex). Also, because the risk for perinatal HIV transmission is high without appropriate intervention, clinicians are advised to assess whether women of childbearing age might be pregnant, are interested in becoming pregnant, or are not specifically considering pregnancy but are sexually active and not using reliable contraception (39,56,57). Women who are unable to become pregnant because of elective sterilization, hysterectomy, salpingo-oophorectomy, or other medical reasons might be less likely to use condoms because of a lack of concern for contraception; these women should be counseled regarding the need for use of condoms to prevent transmission of HIV. Patients who wish to conceive and whose partner is not infected also might engage in risky behavior. Patients interested in pregnancy, for themselves or their partner, should be referred to a reproductive health specialist (58). Injection-drug--related behaviors important to address in screening include whether the patient has been injecting illicit drugs; whether the patient has been sharing needles and syringes or other injection equipment; how many partners the patient has shared needles with; whether needle-sharing partners are known to be HIV infected, not infected, or of unknown HIV serostatus; whether the patient has been using new or sterilized needles and syringes; and what barriers exist to ceasing illicit drug use or, failing that, to adopting safer injection practices (e.g., lack of access to sterile needles and syringes). Approaches to Screening for Behavioral Risk Factors The most effective manner for screening for behavioral risk factors is not well defined; however, simple approaches are more acceptable to both patients and health-care providers (53). Screening tools should be designed to be as sensitive as possible for identifying behavioral risks; a more detailed, personalized assessment can then be used to improve specificity and provide additional detail. The sensitivity of screening instruments depends on obtaining accurate information. However, accuracy of information can be influenced by a variety of factors: recall, misunderstanding about risk, legal concerns, concern about confidentiality of the information and how the information will be used, concern that answers may affect ability to receive services, concern that answers may affect social desirability (i.e., the tendency to provide responses that will avoid criticism), and the desire for social approval (the tendency to seek praise) (45,55). Interviewer factors also influence the accuracy of information. Surveys indicate that patients are more likely to discuss risk behaviors if they perceive their clinicians are comfortable talking about stigmatized topics such as sex and drug use (46--49) and are nonjudgmental, empathetic, knowledgeable, and comfortable counseling patients about sexual risk factors (41,46--50). These factors need to be considered when interpreting responses to screening questions. To the extent possible, screening and interventions should be individualized to meet patient needs. Examples of two screening approaches are provided (Box 1). Incorporating Screening for Behavioral Risk Factors into the Office Visit Before the patient is seen by the clinician, screening for behavioral risks can be done with a self-administered questionnaire; a computer-, audio-, or video-assisted questionnaire; or a brief interview with ancillary staff; the clinician can then review the results on the patient's medical record. Alternatively, behavioral risk screening can be done during the medical encounter (e.g., as part of the history); either open-ended questions or a checklist approach with in-depth discussion about positive responses can be used (Box 1). Because, given patients' immediate health needs, it can be difficult in the clinical care setting to remember less urgent matters such as risk screening and harm reduction, provider reminder systems (e.g., computerized reminders) have been used by health-care systems to help ensure that recommended procedures are done regularly. Multicomponent health-care system interventions that include a provider reminder system and a provider education program are effective in increasing delivery of certain prevention services (59). Risk screening might be more likely to occur in managed care settings if the managed care organization specifically calls for it (60). Screening for Clinical Risk FactorsScreening for STDs Recommendations for preventive measures, including medical screening and vaccinations, that should be included in the care of HIV-infected persons (16,21,39,44,54,61--69) have been published previously. This report is not intended to duplicate existing recommendations; it addresses screening specifically to identify clinical factors associated with increased risk for transmission of HIV from infected to noninfected persons. In this context, STDs are the primary infections of concern for three reasons. First, the presence of STDs often suggests recent or ongoing sexual behaviors that may result in HIV transmission. Second, many STDs enhance the risk for HIV transmission or acquisition (22,70--73). Early detection and treatment of bacterial STDs might reduce the risk for HIV transmission. Third, identification and treatment of STDs can reduce the potential for spread of these infections among high-risk groups (i.e., sex or drug-using networks). Screening and diagnostic testing serve distinctly different purposes. By definition, screening means testing on the basis of risk estimation, regardless of clinical indications for testing, and is a cornerstone of identifying persons at risk for transmitting HIV to others. Clinicians should routinely ask about STD symptoms, including urethral or vaginal discharge; dysuria; intermenstrual bleeding; genital or anal ulcers or other lesions; anal pain, pruritus, burning, discharge, or bleeding; and, for women, lower abdominal pain with or without fever. Regardless of reported sexual behavior or other epidemiologic risk information, the presence of such symptoms should always prompt diagnostic testing and, when appropriate, treatment. However, clinical symptoms are not sensitive for identifying many infections because most STDs are asymptomatic (74--81); therefore, laboratory screening of HIV-infected persons is an essential tool for identifying persons at risk for transmitting HIV and other STDs. Laboratory Testing for STDs Identification of syphilis requires direct bacteriologic (i.e., dark-field microscopy) or serologic testing. However, noninvasive, urine-based nucleic acid amplification tests (NAATs) have greatly simplified testing for Neisseria gonorrhoeae and Chlamydia trachomatis. Although they are more costly than other screening tests, their ease of use and sensitivity---similar to the sensitivity of culture for detection of N. gonorrhoeae and substantially higher than the sensitivity of all other tests for C. trachomatis (including culture)---for detecting genital infection are great advantages. Detection of rectal or pharyngeal gonorrhea still requires culture. Pharyngeal infection with C. trachomatis is uncommon, and routine screening for it is not recommended (63,82). NAATs have not been approved for use with specimens collected from sites other than the urethra, cervix, or urine. Recommended screening strategies and diagnostic tests for detecting asymptomatic STDs are described (Box 2, Table3). Local and state health departments have reporting requirements, which vary among states, for HIV and other STDs. Clinicians need to be aware of and comply with requirements for the areas in which they practice; information on reporting requirements can be obtained from health departments. Screening for Pregnancy Women of childbearing age should be questioned during routine visits about the possibility of pregnancy. Women who state that they suspect pregnancy or have missed their menses should be tested for pregnancy. Early pregnancy diagnosis would benefit even women not receiving antiretroviral treatment because they could be offered treatment to decrease the risk for perinatal HIV transmission. Behavioral InterventionsBehavioral interventions are strategies designed to change persons' knowledge, attitudes, behaviors, or practices in order to reduce their personal health risks or their risk of transmitting HIV to others (Table 4). Behavioral change can be facilitated by environmental cues in the clinic or office setting, messages delivered to patients by clinicians or other qualified staff on-site, or referral to other persons or organizations providing prevention services. Because behavior change often occurs in incremental steps, a brief behavioral intervention conducted at each clinic visit could result in patients, over time, adopting and maintaining safer practices. Behavioral interventions should be appropriate for the patient's culture, language, sex, sexual orientation, age, and developmental level (44). In settings where care is delivered to HIV-infected adolescents, for example, approaches need to be specifically tailored for this age group (83). Also, clinicians should be aware of and adhere to all laws and regulations related to providing services to minors. Structural Approaches To Support and Enhance PreventionClinic or office environments can be structured to support and enhance prevention. All patients, especially new patients, should be provided printed information about HIV transmission risks, preventing transmission of HIV to others, and preventing acquisition of other STDs. Information can be disseminated at various locations in the clinic; for example, posters and other visual cues containing prevention messages can be displayed in examination rooms and waiting rooms. These materials usually can be obtained through local or state health department HIV/AIDS and STD programs or from the National Prevention Information Network (NPIN) (1-800-458-5231; http://www.cdcnpin.org). Additionally, condoms should be readily accessible at the clinic. Repeating prevention messages throughout the patient's clinic visit reinforces their importance, increasing the likelihood that they will be remembered (68). Interventions Delivered On-SitePrevention Messages for All Patients All HIV-infected patients can benefit from brief prevention messages emphasizing the need for safer behaviors to protect both their own health and the health of their sex or needle-sharing partners. These messages can be delivered by clinicians, nurses, social workers, case managers, or health educators. They include discussion of the patient's responsibility for appropriate disclosure of HIV serostatus to sex and needle-sharing partners. Brief clinician-delivered approaches have been effective with a variety of health issues, including depression (84), smoking (85--90), alcohol abuse (91,92), weight and diet (93), and physical inactivity (94). This diverse experience with other health behaviors suggests that similar approaches may be effective in reducing HIV-infected patients' transmission risk behaviors. For patients already taking steps to reduce their risk of transmitting HIV, hearing the messages can reinforce continued risk-reduction behaviors. These patients should be commended and encouraged to continue these behaviors. General HIV Prevention Messages Patients frequently have inadequate information regarding factors that influence HIV transmission and methods for preventing transmission. The clinician should ensure that patients understand that the most effective methods for preventing HIV transmission remain those that protect noninfected persons against exposure to HIV. For sexual transmission, the only certain means for HIV-infected persons to prevent sexual transmission to noninfected persons are sexual abstinence or sex with only a partner known to be already infected with HIV. However, restricting sex to partners of the same serostatus does not protect against transmission of other STDs or the possibility of HIV superinfection unless condoms of latex, polyurethane, or other synthetic materials are consistently and correctly used. Superinfection with HIV has been reported and appears to be rare, but its clinical consequences are not known (95,96). For injection-related transmission, the only certain means for HIV-infected persons to prevent transmission to noninfected persons are abstaining from injection drug use or, for IDUs who are unable or unwilling to stop injecting drugs, refraining from sharing injection equipment (e.g., syringes, needles, cookers, cottons, water) with other persons. Neither antiretroviral therapy for HIV-infected persons nor postexposure prophylaxis for partners is a reliable substitute for adopting and maintaining behaviors that guard against HIV exposure (97). Identifying and Correcting Misconceptions Patients might have misconceptions about HIV transmission (98), particularly with regard to the risk for HIV transmission associated with specific behaviors, the effect of antiretroviral therapy on HIV transmission, or the effectiveness of postexposure prophylaxis for nonoccupational exposure to HIV. Risk for HIV Transmission Associated with Specific Sexual Behaviors. Patients often ask their clinicians about the degree of HIV transmission risk associated with specific sexual activities. Numerous studies have examined the risk for HIV transmission associated with various sex acts (99--113). These studies indicate that some sexual behaviors do have a lower average per-act risk for transmission than others and that replacing a higher-risk behavior with a relatively lower-risk behavior might reduce the likelihood that HIV transmission will occur. However, risk for HIV transmission is affected by numerous biological factors (e.g., host genetics, stage of infection, viral load, coexisting STDs) and behavioral factors (e.g., patterns of sexual and drug-injection partnering) (105,114), and per-act risk estimates based on models that assume a constant per-contact infectivity could be inaccurate (110,113). Thus, estimates of the absolute per-episode risk for transmission associated with different activities could be highly misleading when applied to a specific patient or situation. Further the relative risks of becoming infected with HIV, from the perspective of a person not infected with HIV, might vary greatly according to the various choices related to sexual behavior (Table 5) (115,116). Effect of Antiretroviral Therapy on HIV Transmission. High viral load is a major risk factor for HIV transmission (117--125). Among untreated patients, the risk for HIV transmission through heterosexual contact has been shown to increase approximately 2.5-fold for each 10-fold increase in plasma viral load (126) (Table 6). By lowering viral load, antiretroviral therapy might reduce risk for HIV transmission, as has been demonstrated with perinatal transmission (127,128) and indirectly suggested for transmission via genital secretions (semen and cervicovaginal fluid) (2,129--133). However, because HIV can be detected in the semen, rectal secretions, female genital secretions, and pharynx of HIV-infected patients with undetectable plasma viral loads (16,134--137) and because consistent reduction of viral load depends on high adherence to antiretroviral regimens, the clinician should assume that all patients who are receiving therapy, even those with undetectable plasma HIV levels, can still transmit HIV. Patients who have treatment interruptions, whether scheduled or not, should be advised that this will likely lead to a rise in plasma viral load and increased risk for transmission. Another concern related to adherence to antiretroviral therapy is the development of drug-resistant mutations with subsequent transmission of drug-resistant viral strains. Several reports suggest that transmission of drug-resistant HIV occurs in the United States (138--141). Recent reports suggest that drug-resistant HIV strains might be less easily transmitted than wild-type virus (142), but these data are limited and their significance is unclear. Effectiveness of Postexposure Prophylaxis for Non occupational Exposure to HIV. Although the U.S. Public Health Service recommends using antiretroviral drugs to reduce the likelihood of acquiring HIV infection from occupational exposure (e.g., accidental needle sticks received by health care workers) (143), limited data are available on efficacy of prophylaxis for nonoccupational exposure (97,143--147). Observational data suggesting effectiveness have been reported (148); however, postexposure prophylaxis might not protect against infection in all cases, and effectiveness of these regimens might be further hindered by lack of tolerability, potential toxicity, or viral resistance. Thus, avoiding exposure remains the best approach to preventing transmission, and the potential availability of postexposure prophylaxis should not be used as justification for engaging in risky behavior. Tailored Interventions for Patients at High Risk for Transmitting HIV Interventions tailored to the individual patient's risks can be delivered to patients at highest risk for transmitting HIV infection and for acquiring new STDs. This includes patients whose risk screening indicates current sex or drug-injection practices that may lead to transmission, who have a current or recent STD, or who have mentioned items of concern in discussions with the clinician (149,150). Any positive results of screening for behavioral risks or STDs should be addressed in more detail with the patient so a more thorough risk assessment can be done and an appropriate risk-reduction plan can be discussed and agreed upon. Although the efficacy of brief clinician-delivered interventions with HIV-infected patients has not been studied extensively, substantial evidence exists for the efficacy of provider-delivered, tailored messages for other health concerns (151--155). An attempt should be made to determine which of the patient's risk behaviors and underlying concerns can be addressed during clinic visits and which might require referral (Box 3). At a minimum, an appropriate referral should be made and the patient should be informed of the risks involved in continuing the behavior. HIV-infected persons who remain sexually active should be reminded that the only certain means for preventing transmission to noninfected persons is to restrict sex to partners known to be already infected with HIV and that they have a responsibility for disclosure of HIV serostatus to prospective sex partners. For mutually consensual sex with a person of unknown or discordant HIV serostatus, consistent and correct use of condoms made of latex, polyurethane, or other synthetic materials can substantially reduce the risk for HIV transmission. Also, some sex acts have relatively less risk for HIV transmission than others (Table 5). For HIV-infected patients who continue injection drug use, the provider should emphasize the risks associated with sharing needles and should provide information regarding substance abuse treatment and access to clean needles (Box 4) (156--158). Examples of targeted motivational messages on condom use and needle sharing are provided (Figures 1 and 2), and providers can individualize their own messages using these as a guide. Clinician Training Clinicians can prepare themselves to deliver HIV prevention messages and brief behavioral interventions to their patients by 1) developing strategies for incorporating HIV risk-reduction interventions into patients' clinic visits (159); 2) obtaining training on speaking with patients about sex and drug-use behaviors and on giving explanations in simple, everyday language (68,87,160,161); 3) becoming familiar with interventions that have demonstrated effectiveness (162); 4) becoming familiar with the underlying causes of and concerns related to risk behaviors among HIV-infected persons (e.g., domestic violence) (13,163); and 5) becoming familiar with community resources that address risk reduction. Free training on risk screening and prevention can be obtained at CDC-funded STD/HIV Prevention Training Centers (http://depts.washington.edu/nnptc) and HRSA-funded AIDS Education and Training Centers (http://www.aids-ed.org), which also offer continuing medical education credit for this training. Ongoing training will help clinicians refine their counseling skills as well as keep current with prevention concerns at the community level, thus increasing their ability to appropriately counsel and provide support to patients. Ongoing Delivery of Prevention Messages Prevention messages can be reinforced by subsequent longer or more intensive interventions in clinic or office environments by nurses, social workers, or health educators. Advantages of a multidisciplinary approach are that skill sets vary among staff members from various disciplines and that a patient may be more receptive to discussing prevention-related issues with one team member than with another. For HIV-negative persons or persons of unknown HIV serostatus, randomized controlled trials provide strong evidence for the efficacy of short, one- or two-session interventions (164--170) and for longer or multisession interventions in clinics for individuals and groups (164,171--173). For example, for persons who continue to engage in risky behaviors, CDC recommends client-centered counseling, a specific model of HIV prevention counseling (44,164). Evidence for the efficacy of multisession interventions for HIV-infected patients, individually or in groups, in clinical settings is limited to a few randomized, controlled trials (69,174,175) and other studies that might not have assessed behavioral outcomes (6,176--180). The studies of single-session interventions for individual HIV-infected patients in clinical settings have not been randomized controlled trials (181--187). Referrals for Additional Prevention Interventions and Other ServicesTypes of Referrals Certain patients need more intensive or ongoing behavioral interventions than can feasibly be provided in medical care settings (44). Many have underlying problems that impede adoption of safer behaviors (e.g., homelessness, substance abuse, mental illness), and achieving behavioral change is often dependent on addressing these concerns. Clinicians will usually not have time or resources to fully address these issues, many of which can best be addressed through referrals for services such as intensive HIV prevention interventions (e.g., multisession risk-reduction counseling, support groups), medical services (e.g., family planning and contraceptive counseling, substance abuse treatment), mental health services (e.g., treatment of depression, counseling for sexual compulsivity), and social services (e.g., housing, child care and custody, protection from domestic violence). For example, all patients should be made aware of their responsibility for appropriate disclosure of HIV serostatus to sex and needle-sharing partners; however, full consideration of the complexities of disclosure, including benefits and potential risks, may not be possible in the time available during medical visits (188). Patients who are having, or are likely to have, difficulty initiating or sustaining behaviors that reduce or prevent HIV transmission might benefit from prevention case management. Prevention case management provides ongoing, intensive, one-on-one, client-centered risk assessment and prevention counseling, and assistance accessing other services to address concerns that affect patients' health and ability to change HIV-related risk-taking behavior. For HIV-seronegative persons, randomized controlled trials provide evidence for the efficacy of HIV prevention interventions delivered by health departments and community-based organizations (164,189--198). For HIV-infected persons, efficacy studies of such interventions are limited to a few randomized controlled trials (199--201), only one of which documented change in risk-related behavior (199), and to other studies, the majority of which did not assess behavioral outcomes (7,202--207). Referrals for IDUs For IDUs, ceasing injection-drug use is the only reliable way to eliminate the risk of injection-associated HIV transmission; however, most IDUs are unable to sustain long-term abstinence without substance abuse treatment. Several studies have examined the effect of substance abuse treatment, particularly methadone maintenance treatment, on HIV risk behaviors among IDUs (208--210). These include controlled (211--217) and noncontrolled (218--221) cohort studies, case-control studies (222), and observational studies with controls (223,224), and collectively they provide evidence that methadone maintenance treatment reduces risky injection and sexual behaviors and HIV seroconversion. Thus, early entry into substance abuse treatment programs, maintenance of treatment, and sustained abstinence from injecting are crucial for reducing the risk for HIV transmission from infected IDUs. For those IDUs not able or willing to stop injecting drugs, once-only use of sterile syringes can greatly reduce the risk for injection-related HIV transmission. Substantial evidence from cohort, case-control, and observational studies (225) indicates that access to sterile syringes through syringe exchange programs reduces HIV risk behavior and HIV seroconversion among IDUs. Physician prescribing and pharmacy programs can also increase access to sterile syringes (226--231). Disinfecting syringes and other injection equipment by boiling or flushing with bleach when new, sterile equipment is not available has been suggested to reduce the risk for HIV transmission (156); however, it is difficult to reliably disinfect syringes, and this practice is not as safe as using a new, sterile syringe (232--234). Information on access to sterile syringes and safe syringe disposal can be obtained through local health departments or state HIV/AIDS prevention programs. Engaging the Patient in the Referral Process When referrals are made, the patient's willingness and ability to accept and complete a referral should be assessed. Referrals that match the patient's self-identified priorities are more likely to be successful than those that do not; the services need to be responsive to the patient's needs and appropriate for the patient's culture, language, sex, sexual orientation, age, and developmental level. For example, adolescents should be referred to behavioral intervention programs and services that work specifically with this population. Discussion with the patient can identify barriers to the patient's completing the referral (e.g., lack of transportation or child care, work schedule, cost). Accessibility and convenience of services predict whether a referral will be completed. The patient should be given specific information regarding accessing referral services and might need assistance (e.g., scheduling appointments, obtaining transportation) in completing referrals. The likelihood that referrals will be completed successfully could possibly be increased if clinicians or other health-care staff assist patients with making appointments to referral services. When a clinician does not have the capacity to make all appropriate referrals, or when needs are especially complex, a case manager can help make referrals and coordinate care. Outreach workers, peer counselors or educators, treatment advocates, and treatment educators can also help patients identify needs and complete referrals successfully. Health department HIV/AIDS prevention and care programs can provide information on accessing these services. Assessing the success of referrals by documenting referrals made, the status of those referrals, and patient satisfaction with referrals will further assist clinicians in meeting patient needs. Information obtained through follow-up of referrals can identify barriers to completing the referral, responsiveness of referral services to patient needs, and gaps in the referral system, and can be used to develop strategies for removing the barriers. Referral Guides and Information Preparation for making patient referrals includes 1) learning about local HIV prevention and supportive social services, including those supported by the Ryan White CARE Act; 2) learning about available resources and having a referral guide listing such resources; and 3) contacting staff in local programs to facilitate subsequent referrals. Referral guides and other information usually can be obtained from local and state health department HIV/AIDS prevention and care programs, which are key sources of information about services available locally. Health departments and some managed care organizations are also a source of educational materials, posters, and other prevention-related material. Health departments can provide or suggest sources of training and technical assistance on behavioral interventions. A complete listing of state AIDS directors and contact information is available from the National Alliance of State and Territorial AIDS Directors (NASTAD) at http://www.nastad.org. In addition, information can be obtained from local health planning councils, consortia, and community planning groups; local, state, and national HIV/AIDS information hotlines and Internet websites; and community-based health and human service providers (Box 5). Examples of Case Situations for Prevention Counseling1. A patient with newly diagnosed HIV infection comes to your office for initial evaluation. Of the many things that must be addressed during this initial visit (e.g., any emergent medical or psychiatric problems, education about HIV, history, physical, initial laboratory work [if not already done]), how does one address prevention? What is the minimum that should be done, and how can it be incorporated into this visit? Assuming no emergent issues preclude a complete history and physical examination during this visit, the following should be done:
2. A patient with chronic, stable HIV comes to you with a new STD. What prevention considerations should be covered in this visit? For the patient who has had a stable course of disease, a new STD can be a sign of emerging social, emotional, or substance abuse problems. These potential problems should be addressed in addition to the STD.
3. A patient with chronic, stable HIV has been seen regularly in a health care setting. What should be included in this patient's routine clinical care? Discussion of sexual and needle-sharing practices should be integrated into a routine part of clinical care.
4. A patient who has been treated with HAART for 2 years comes to you. At the time of treatment initiation, CD4+count was 200 cells/µL and the viral load was 50,000 copies/ml. The response to therapy was prompt; CD4+ count increased to 500 cells/µL, and the viral load has been undetectable since soon after treatment began. The patient now has mildly elevated cholesterol, some mild lipodystrophy, and facial wasting. He states that he would like to stop HAART because of the side effects. What should you tell this patient?
Partner Counseling and Referral Services, Including Partner NotificationHIV-infected persons are often not yet aware of their infection; thus, they cannot benefit from early medical evaluation and treatment and do not know that they may be transmitting HIV to others. Reaching such persons as early after infection as possible is important for their own health and is a critical strategy for reducing HIV transmission in the community. Furthermore, interviews of HIV-infected persons in various settings suggest that >70% are sexually active after receiving their diagnosis, and many have not told their partners about their infection (188). Partner counseling and referral services (PCRS), including partner notification, are intended to address these problems by 1) providing services to HIV-infected persons and their sex and needle-sharing partners so the partners can take steps to avoid becoming infected or, if already infected, to avoid infecting others and 2) helping infected partners gain earlier access to medical evaluation, treatment, and other services (Table 7). A key element of PCRS involves informing current partners (and past partners who may have been exposed) that a person who is HIV infected has identified them as a sex or needle-sharing partner and advising them to have HIV counseling and testing (235--238). Informing partners of their exposure to HIV is confidential; i.e., partners are not told who reported their name or when the reported exposure occurred. It is voluntary in that the infected person decides which names to reveal to the interviewer. Studies have indicated that infected persons are more likely to name their close partners than their more casual partners (204,239,240). Limited reports of partner violence after notification suggest a need for caution, but such violence seems to be rare (241--2). When asked, 92% of notified partners reported that they believe the health department should continue partner notification services (243). No studies have directly shown that PCRS prevents disease in a community. However, studies have demonstrated that quality HIV prevention counseling can reduce the risk of acquiring a new STD (164) and that persons who become aware of their HIV infection can take steps to protect their health and prevent further transmission (244); in addition, before--after studies have suggested that partners change their behavior after they are notified (245). Finally, compelling arguments have been offered regarding partners' rights to know this information that is important to their health. Laws and Regulations Related to Informing PartnersThe majority of states and some cities or localities have laws and regulations related to informing partners that they have been exposed to HIV. Certain health departments require that, even if a patient refuses to report a partner, the clinician report to the health department any partner of whom he or she is aware. Many states also have laws regarding disclosure by clinicians to third parties known to be at high risk for future HIV transmission from patients known to be infected (i.e., duty to warn) (246). Clinicians should know and comply with any such requirements in the areas in which they practice. With regard to PCRS, clinicians should also be aware of and adhere to all laws and regulations related to providing services to minors. Approaches to Notifying PartnersPartners can be reached and informed of their exposure by health department staff, clinicians in the private sector, or the infected person. In the only randomized controlled trial that has been conducted to date (175), 35 HIV-infected persons were asked to notify their partners themselves, and 10 partners were notified. Another 39 HIV-infected persons were assigned to health department referral; and for these, 78 partners were notified. Thus, notification by the health department appears to be substantially more effective than notification by the infected person. Other studies, with less rigorous designs, have demonstrated similar results (247,248). Some persons, when asked, prefer to inform their partners themselves. This could have a benefit if partners provide support to the infected person. However, patients frequently find that informing their partners is more difficult than they anticipated. Certain health departments offer contract referral, in which the infected person has a few days to notify his or her partners. If by the contract date the partners have not had a visit for counseling and testing, they are then contacted by the health department. In practice, patients' difficulties in informing their partners usually means notification is done by the health department. Although clinicians might wish to take on the responsibility for informing partners, one observational study has indicated that health department specialists were more successful than physicians in interviewing patients and locating partners (249). Health departments have staff who are trained to do partner notification and skilled at providing this free, confidential service. These disease intervention specialists can work closely with public and private sector clinicians who treat persons with other STDs. With regard to partner notification, the clinician should be sensitive to concerns of domestic violence or abuse by the informed partner. All partners should be notified at least once. Persons who continue to have sex with an HIV-infected person despite an earlier notification may have erroneously concluded that someone else was the infected partner. Thus, renotification might be important, although no research is available on renotification. Additional information, recommendations, and requirements related to PCRS are available through health department HIV/AIDS programs. A complete listing of state AIDS directors and contact information is available from the National Alliance of State and Territorial AIDS Directors (NASTAD) at http://www.nastad.org. Acknowledgments The preparers are grateful to P. Lynne Stockton, V.M.D, and P. Susanne Justice, CDC, for their editorial assistance and to Mark R. Vogel, M.A., HIVMA of IDSA, who assisted in coordinating responses from members of that organization. References
Members of the HIV Prevention in Clinical Care Working Group CDC: Sevgi Aral, Ph.D., Samuel W. Dooley, M.D., Mary L. Kamb, M.D., Jonathan
Kaplan, M.D., Mary Spink Neumann, Ph.D., Ida M. Onorato, M.D.,Thomas A.
Peterman, M.D., Kathryn J. Rauch, Renee Ridzon, M.D., J. Walton Senterfitt,
Ph.D., Atlanta, Georgia. Consultants to the Working Group Bruce D. Agins, M.D., New York State Department of Health
AIDS Institute, New York, New York; Kim W. Hamlett-Berry, Ph.D.,
Department of Veterans Affairs, Washington, D.C.; H. Hunter Handsfield,
M.D., University of Washington, Public Health-Seattle and King County,
Seattle, Washington; Fredrick Hecht, M.D., University of California, San
Francisco AIDS Program, San Francisco, California (HIVMA of IDSA); King K.
Holmes, M.D., University of Washington, Seattle, Washington; Kenneth
Mayer, M.D., Brown University School of Medicine, Providence, Rhode Island
(HIVMA of IDSA); Thomas C. Quinn, M.D., The Johns Hopkins University
School of Medicine, Baltimore, Maryland; Julie M. Scofield, National
Alliance of State and Territorial AIDS Directors, Washington, D.C.; Dan
Wohlfeiler, M.P.H., California Department of Public Health, Berkeley,
California.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 7/14/2003 |
|||||||||
This page last reviewed 7/14/2003
|