Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Prevention of Varicella
Recommendations of the Advisory Committee on Immunization
Practices (ACIP)
Prepared by
Mona Marin, MD, Dalya Güris, MD,* Sandra S. Chaves,
MD, Scott Schmid, PhD, Jane F. Seward, MBBS Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC
The material in this report originated in the National Center for Immunization and Respiratory Diseases, Anne Schuchat, MD, Director; and the Division
of Viral Diseases, Larry Anderson, MD, Director.
Corresponding preparer: Mona Marin, MD, National Center for Immunization and Respiratory Diseases, CDC, 1600 Clifton Road NE, MS
A-47, Atlanta, GA 30333. Telephone: 404-639-8791; Fax: 404-639-8665; E-mail:
mmarin@cdc.gov.
Summary
Two live, attenuated varicella zoster virus--containing vaccines are available in the United States for prevention of
varicella: 1) a single-antigen varicella vaccine
(VARIVAX,® Merck & Co., Inc., Whitehouse Station, New Jersey), which was licensed
in the United States in 1995 for use among healthy children aged
>12 months, adolescents, and adults; and 2) a
combination measles, mumps, rubella, and varicella vaccine
(ProQuad,® Merck & Co., Inc., Whitehouse Station, New Jersey), which
was licensed in the United States in 2005 for use among healthy children aged 12 months--12 years. Initial Advisory
Committee on Immunization Practices (ACIP) recommendations for prevention of varicella issued in 1995 (CDC. Prevention
of varicella: recommendations of the Advisory Committee on Immunization Practices [ACIP]. MMWR 1996;45[No.
RR-11]) included routine vaccination of children aged 12--18 months, catch-up vaccination of susceptible children aged 19
months--12 years, and vaccination of susceptible persons who have close contact with persons at high risk for serious complications
(e.g., health-care personnel and family contacts of immunocompromised persons). One dose of vaccine was recommended
for children aged 12 months--12 years and 2 doses, 4--8 weeks apart, for persons aged
>13 years. In 1999, ACIP updated the recommendations (CDC. Prevention of varicella: updated recommendations of the Advisory Committee on
Immunization Practices [ACIP]. MMWR 1999;48[No. RR-6]) to include establishing child care and school entry requirements, use of
the vaccine following exposure and for outbreak control, use of the vaccine for certain children infected with
human immunodeficiency virus, and vaccination of adolescents and adults at high risk for exposure or transmission.
In June 2005 and June 2006, ACIP adopted new recommendations regarding the use of live, attenuated varicella
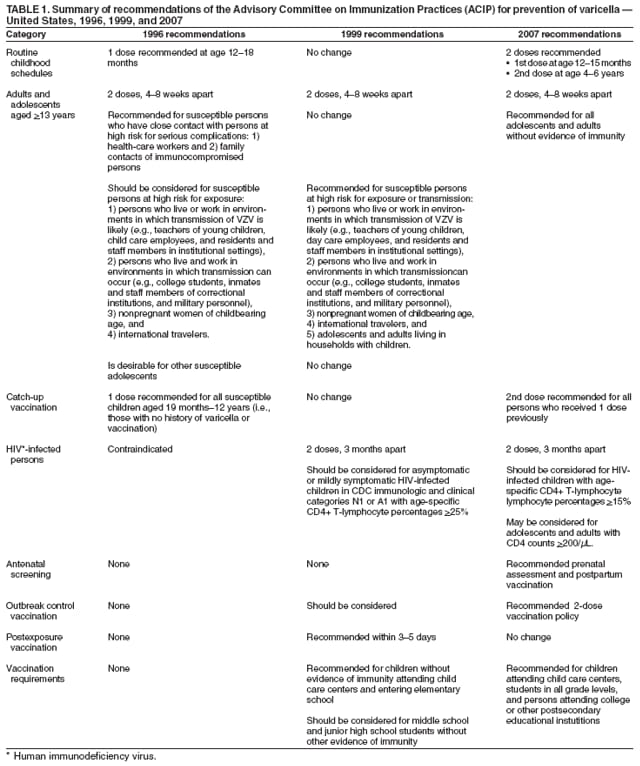
vaccines for prevention of varicella. This report revises, updates, and replaces the 1996 and 1999 ACIP statements for prevention
of varicella. The new recommendations include 1) implementation of a routine 2-dose varicella vaccination program
for children, with the first dose administered at age 12--15 months and the second dose at age 4--6 years; 2) a second dose
catch-up varicella vaccination for children, adolescents, and adults who previously had received 1 dose; 3) routine vaccination of
all healthy persons aged >13 years without evidence of immunity; 4) prenatal assessment and postpartum vaccination;
5) expanding the use of the varicella vaccine for HIV-infected children with age-specific CD4+T lymphocyte percentages of
15%--24% and adolescents and adults with CD4+T lymphocyte counts
>200 cells/µL; and 6) establishing middle school,
high school, and college entry vaccination requirements. ACIP also approved criteria for evidence of immunity to varicella.
Introduction
Varicella is a highly infectious disease caused by the varicella-zoster virus (VZV). Secondary attack rates for this virus
might reach 90% for susceptible household contacts. VZV causes a systemic infection that results typically in lifetime immunity.
In otherwise healthy persons, clinical illness after reexposure is rare.
In 1995, a vaccine to prevent varicella
(VARIVAX,® Merck & Co., Inc., Whitehouse Station, New Jersey) was licensed
in the United States for use among healthy children aged
>12 months, adolescents, and adults; recommendations of the
Advisory Committee on Immunization Practices (ACIP)
regarding use of the varicella vaccine have been published previously
(1,2) This report revises, updates, and replaces earlier ACIP statements
(Table 1).
Methods
In response to increasing reports of varicella outbreaks among highly vaccinated populations
(3--6), ACIP's measles-mumps-rubella and varicella (MMRV) workgroup first met in February 2004 to review data related to varicella vaccine use in
the United States since implementation of the vaccination program in 1995 and to consider recommendation options
for improving control of varicella disease. The workgroup held monthly conference calls and met in person three times a year.
The workgroup reviewed data on the impact of the 1-dose varicella vaccination program, including data on vaccination
coverage, changes in varicella epidemiology, transmission from vaccinated persons with varicella, vaccine effectiveness,
immune response to vaccination, evidence of immunity, and potential risk factors for vaccine failure. Published and
unpublished data related to correlates of protection, safety, immunogenicity, and
efficacy† of the new quadrivalent MMRV vaccine and
the immunogenicity and efficacy of a second dose of varicella vaccine also were reviewed.
Cost-benefit and cost-effectiveness analyses were considered, including revised cost-benefit analysis of both the 1- and 2-dose programs for children
compared with no vaccination program and the incremental benefit of a second dose. Presentations were made to the full ACIP
meetings in October 2004, February 2005, June 2005, and June 2006. Recommendation options were developed and discussed by
the MMRV workgroup. When definitive research evidence was lacking, the recommendations incorporated expert opinion of
the workgroup members. The workgroup sought input from partner organizations (i.e., the American Academy of
Pediatrics [AAP], the American Academy of Family Physicians [AAFP], the American College of Obstetricians and Gynecologists,
the Council of State and Territorial Epidemiologists, and the
Association of Immunization Managers) and from state public
health professionals and immunization program directors. Proposed recommendations and a draft statement were presented to
the full ACIP in June 2005 and June 2006. After deliberations, final ACIP recommendations were approved in 2005 and
2006. Modifications to the draft statement were made following CDC and external review process to update and clarify wording
in the document.
Epidemiology of Varicella
General
VZV is transmitted from person to person by direct contact, inhalation of aerosols from vesicular fluid of skin lesions
of acute varicella or zoster, or infected respiratory tract secretions that also might be aerosolized. The virus enters the
host through the upper-respiratory tract or the conjunctiva.
The average incubation period for varicella is 14--16
days§ after exposure to rash; however, this period can vary (range:
10--21 days). The period of contagiousness of infected persons is estimated to begin 1--2 days before the onset of rash and to
end when all lesions are crusted, typically 4--7 days after onset of rash
(7). Persons who have progressive varicella
(i.e., development of new lesions for >7 days) might be contagious longer, presumably because their immune response is
depressed, which allows viral replication to persist. VZV
remains dormant in sensory-nerve ganglia and might be
reactivated at a later time, causing herpes zoster (HZ) (i.e., shingles), a painful vesicular rash typically appearing in a dermatomal distribution
of one or two sensory-nerve roots.
Since implementation of a universal childhood varicella vaccination program in 1995, the epidemiology and
clinical characteristics of varicella in the United States have changed, with substantial declines in morbidity and mortality
attributable to varicella. No consistent changes in HZ epidemiology have been documented.
Vaccinated persons might develop modified varicella disease with atypical presentation. Varicella disease that develops
>42 days after vaccination (i.e., breakthrough varicella) typically is mild, with <50 skin lesions, low or no fever, and shorter
(4--6 days) duration of illness. The rash is more likely to be predominantly maculopapular rather than vesicular.
Nevertheless, breakthrough varicella is contagious.
Prevaccine Era
Before the introduction of varicella vaccine in 1995, varicella was a universal childhood disease in the United States,
with peak incidence in the spring and an average annual incidence of 15--16 cases per 1,000 population. On the basis of data
from the National Health Interview Survey (NHIS) for 1980--1990, an average of 4 million cases were estimated to have
occurred
annually (annual incidence rate: 15 cases per 1,000 population)
(8). Varicella was not a nationally notifiable disease
when vaccine was introduced in 1995, and surveillance data were limited. In 1994, only 28 states, the District of Columbia,
and New York City reported cases to CDC's National Notifiable Disease Surveillance System (NNDSS); reporting was
passive, with estimated completeness ranging from <0.1% to 20%
(9).
In multiple studies, age-specific incidence data were derived from NHIS and from state and local surveys
(8,10,11). During 1980--1990, an estimated 33% of cases occurred among preschool-aged children (i.e., children aged 12 months--4 years),
and 44% occurred among school-aged children (i.e., children aged 5--9 years) (annual incidence rates: 82.8 and 91.1 cases
per 1,000 children, respectively). Approximately 90%--92% of cases occurred among persons aged <15 years, and cases
occurred rarely among persons aged >50 years. However, studies using data from state and local surveys conducted during
1990--1992 and during 1994--1995 indicated that the highest incidence of varicella occurred among preschool-aged rather than
school-aged children, indicating that the disease was being acquired at earlier ages
(10,11). National seroprevalence data for
1988--1994 indicated that 95.5% of adults aged 20--29 years, 98.9% of adults aged 30--39 years, and >99.6% of adults aged
>40 years were immune to VZV (12). However, for reasons that are not well
understood, the epidemiology of varicella differs between countries with temperate and tropical climates
(13--18). In the majority of countries with temperate climates,
>90% of persons are infected by adolescence whereas in countries with tropical climates, a higher
proportion of infections are acquired at older ages, which results in higher susceptibility among adults
(19).
Estimates of the burden of varicella hospitalization varied according to the year(s) studied, the source of data, and
the definitions used for a varicella-related hospitalization (20--23). Estimates were higher if varicella was listed as either a
principal or a secondary cause of hospitalization, in which case some incidental varicella hospitalization might have been
included. During 1988--1995, an estimated 10,632 hospitalizations were attributable annually to varicella in the United States
(range: 8,198--16,586) (20). Another study demonstrated an annual average of 15,073 hospitalizations during 1993--1995, but
this period might have included an epidemic year
(22). Overall rates of hospitalization for varicella during 1988--1995
ranged from 2.3 to 6.0 cases per 100,000 population. If any
varicella-related hospital discharge diagnostic code was included,
rates varied between 5.0 and 7.0 cases per 100,000 population
(20--23).
During 1988--1995, persons without severe
immuno-compromising conditions or treatments comprised the
largest proportion (89%) of annual varicella-related hospitalizations
(20). Before vaccination, children aged
<4 years accounted for 43%--44% of hospitalizations, and persons aged
>20 years accounted for 32%--33%
(20,22). The rate of complications from varicella was substantially higher for
persons aged >20 years and for infants (i.e., children aged
<1 year). Adults aged >20 years were 13 times more likely to be hospitalized when they had varicella than children aged
5--9 years, and infants aged <1 year were six times more likely to be hospitalized than children aged 5--9 years
(20). The most common complications of
varicella that resulted in hospitalizations were skin and soft tissue infections (especially invasive group A streptococcal
infections), pneumonia, dehydration, and encephalitis. In 1980, an association was identified between Reye syndrome and the use
of aspirin during varicella or influenza-like illness; since then, Reye syndrome, which was once considered a
common complication resulting from varicella infection, has become rare
(24--26).
During 1970--1994, the average annual number of deaths for which varicella was recorded as the underlying cause was
105; the overall average annual varicella mortality rate was 0.4 deaths per 1 million population. The age distribution of
varicella deaths has shifted during this period. During 1970--1974, persons aged <20 years accounted for 80% of varicella
deaths, compared with 46% during 1990--1994. During 1970--1994, the average case-fatality rate (CFR) for varicella for all
ages combined ranged from 2.0 to 3.6 per 100,000 cases, with higher rates among infants and adults aged
>20 years (27). Although CFRs declined substantially during this period, the risk for varicella-related death during 1990--1994 was still
25 times higher for adults than for children aged 12 months--4 years (CFR: 21.3 and 0.8 per 100,000 cases,
respectively). During the same period, 89% of varicella deaths among children and 75% of varicella deaths among adults occurred in
persons without severe underlying immunocompromising medical conditions. The most common complications among persons
who died of varicella were pneumonia, central nervous system complications (including encephalitis), secondary infection,
and hemorrhagic conditions. A recent reanalysis of varicella deaths also considered
varicella when listed as a contributing cause of death in addition to the underlying cause studied in the previous report
(28). During 1990--1994, a varicella diagnosis was
listed on an average of 145 death certificates per year (105 as an underlying cause and 40 as a contributing cause), with an
overall annual varicella mortality rate of 0.6 deaths per 1 million
population.
Varicella during pregnancy can have adverse consequences for the fetus and infant, including congenital varicella
syndrome (see Prenatal and Perinatal Exposure). Reliable data on the number of cases of congenital varicella syndrome are not
available. However, on the basis of age-specific varicella incidence (from NHIS), the annual number of births, and the risk
for congenital varicella syndrome (1.1% overall risk in the first 20 weeks of pregnancy), 44 cases of congenital
varicella syndrome are estimated to have occurred each year in the United States during the prevaccine era
(29).
Postvaccine Era
In 1995, a varicella vaccine
(VARIVAX,® Merck & Co., Inc., Whitehouse Station, New Jersey) was licensed in the
United States for use among healthy children aged
>12 months, adolescents, and adults. At that time, ACIP recommended
routine varicella vaccination of children aged 12--18 months, catch-up vaccination of susceptible children aged 19 months--12
years, and vaccination of susceptible persons who have close contact with persons at high risk for serious complications (e.g.,
health-care workers and family contacts of
immunocompromised persons) (1; Table 1). In 1999, ACIP updated the recommendations
to include child care and school entry requirements, use of the vaccine after exposure and for outbreak control, use of the vaccine
for certain children infected with human immunodeficiency virus (HIV), and vaccination of adolescents and adults at high risk
for exposure or transmission (2; Table 1).
During 1997--2005, national varicella vaccination coverage among children aged 19--35 months increased from 27%
to 88%, with no statistically significant difference in coverage by race or ethnicity
(30). In 2005, state-specific varicella vaccination coverage ranged from 69% to 96%
(31). National surveillance data continue to be limited, but passive
surveillance data in certain states have documented a decline in
varicella incidence.
In four states (Illinois, Michigan, Texas, and West Virginia) with adequate
(>5% of expected cases during
1990--1994) reporting to NNDSS, varicella incidence for 2004 declined 53%--88% compared with the average incidence for
1990--1994, with vaccination coverage among children aged 19--35 months ranging from 82% to 88%
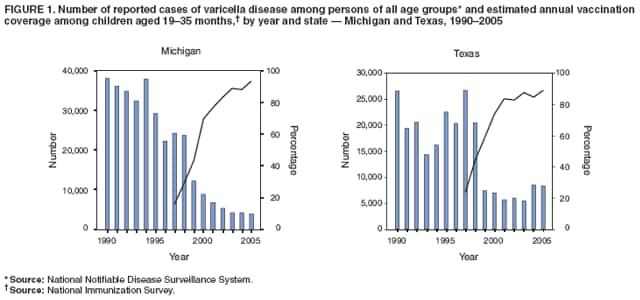
(32; CDC, unpublished data, 2006). During 2003--2005, the number of cases increased in Illinois and Texas; the biggest increase (56%) occurred in
Texas (Figure 1). The number of cases remained stable in Michigan (Figure 1) and declined minimally in West Virginia.
In 1995, along with implementation of the national vaccination program, CDC instituted active surveillance for varicella
in three communities (Antelope Valley, California; Travis County, Texas; and West Philadelphia, Pennsylvania) in
collaboration with state and local health departments to establish baseline data and to monitor trends in varicella disease after
introduction of varicella vaccine. By 2000, vaccination coverage among children 19--35 months in these three communities had
reached 74%--84%, and reported total varicella cases had declined 71%--84%
(33). Although incidence declined to the greatest
extent (83%--90%) among children aged 12 months--4 years, incidence declined in all age groups, including infants and
adults, indicating the herd immunity effects of the vaccination program. Since 2001, only two sites were funded to
continue surveillance (Antelope Valley and West Philadelphia). By 2005, vaccination coverage in these two sites had increased to
90%, and the reduction in incidence had reached 90% and 91%, respectively
(34). During 1996--2005, as vaccination
coverage continued to increase, the proportion of persons with varicella who had been vaccinated increased from 2% to 56%.
During 1995--2004, peak incidence for varicella cases in active surveillance sites shifted from age 3--6 years to age 9--11 years.
After introduction of vaccine in 1995, the number and rate of annual varicella-related hospitalizations declined. In
one study of a nationally representative sample that was conducted during 1993--2001, varicella hospitalizations declined
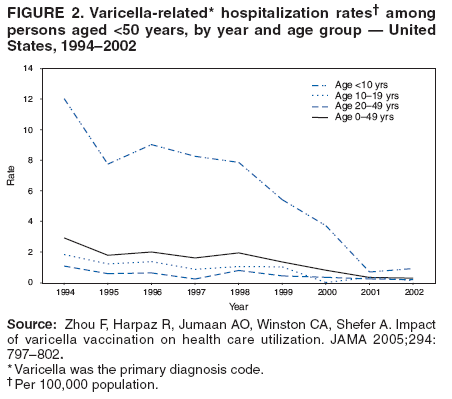
75% (22). In another study, the annual varicella-related hospitalization rate declined 88% during 1994--2002
(23) (Figure 2). Hospitalization rates declined 100% among
infants, and substantial declines also were recorded in all other age groups (up
to age 50 years); hospitalization rates declined 91% among children aged <10 years, 92% among children and adolescents
aged 10--19 years, and 78% among adults aged 20--49 years. The greater decline in hospitalizations among children led to
an increase in the proportion of varicella-related
hospitalizations among adults (40% of hospitalizations in 2002 occurred
among persons aged >20 years) (23). In the
combined active surveillance area, varicella-related hospitalizations declined from
2.4--4.2 hospitalizations per 100,000 population during 1995--1998 to 1.5 per 100,000 population in 2000
(33) and to 0.8 per 100,000 population in 2005
(34).
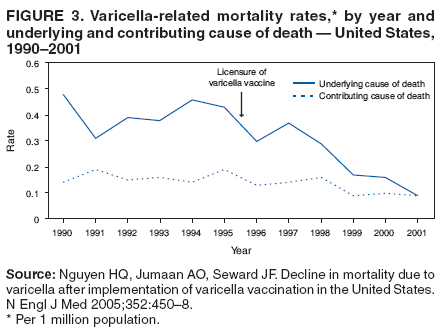
During 1995--2001, the number of deaths for which varicella was listed as the underlying cause decreased from 115 to
26 (28) (Figure 3). Since then, the number of deaths declined further; 16 deaths were reported in 2003. Age-adjusted
mortality rates decreased 66%, from an average of 0.41 deaths per 1 million population during 1990--1994 to 0.14 during
1999--2001. The decline was observed in all age groups <50 years, with the greatest reduction (92%) occurring among children aged
12
months--4 years (0.09 deaths per 1 million population), followed by an 88% reduction among children aged 5--9 years
(0.10 deaths per 1 million population). Deaths among persons aged
>50 years did not decline to the same extent; however,
the validity of reported varicella deaths in this age group is low
(35), and the majority of these deaths are not considered to
be caused by varicella. During 1999--2001, the average rate of mortality attributed to varicella among all racial and
ethnic populations was <0.15 deaths per 1 million persons. Persons without high-risk conditions (e.g.,
malignancies, HIV/acquired immunodeficiency syndrome [AIDS], and other
immune deficiencies) accounted for 92% of deaths attributable
to varicella. The average rates of deaths for which varicella was listed as a contributing cause of death also
declined during 1999--2001, compared with 1990--1994.
Despite high 1-dose vaccination coverage and the success of the vaccination program in reducing varicella morbidity
and mortality, reports to CDC from active surveillance sites and from states with
well-implemented vaccination programs and surveillance indicate that in certain states and in one
active surveillance site, the number of reported varicella cases
has remained constant or declined minimally, and outbreaks have continued to occur. During 2001--2005, outbreaks
were reported in schools with high varicella vaccination coverage (range 96%--100%)
(3,4). The outbreaks were similar in
certain respects: 1) all occurred in elementary schools, 2) vaccine effectiveness was similar (range: 72%--85%), 3) the highest
attack rates occurred among the younger students, 4) each outbreak lasted approximately
2 months, and 5) index cases occurred among vaccinated students (although their disease was mild). Overall attack rates among vaccinated children varied
(range: 11%--17%), with attack rates in certain classrooms as high as 40%. These data indicate that even in settings in
which vaccination coverage was nearly universal and vaccine performed as expected, the 1-dose vaccination program could
not prevent varicella outbreaks completely.
Prenatal and Perinatal Exposure
In the prevaccine era, prenatal infection was uncommon because the majority of women of childbearing age
were immune to VZV (12,36). Varicella in pregnant women is
associated with a risk for VZV transmission to the fetus or
newborn. Intrauterine VZV infection might result in congenital varicella syndrome, neonatal varicella, or HZ during
infancy or early childhood (37--46). Infants who are
exposed prenatally to VZV, even if asymptomatic, might have measurable
varicella-specific IgM antibody during the newborn period, have persistent varicella-specific IgG immunity after age 1 year without
a history of postnatal varicella, or demonstrate positive lymphocyte transformation in response to VZV antigen
(37).
Congenital varicella syndrome was first recognized in 1947
(40). Congenital varicella syndrome can occur among
infants born to mothers infected during the first half of pregnancy and might be manifested by low birthweight, cutaneous
scarring, limb hypoplasia, microcephaly, cortical atrophy, chorioretinitis, cataracts, and other anomalies. In one study, incidence
of congenital varicella syndrome was calculated using aggregate data from nine cohort studies carried out during
1986--2002 (47). Rates were 0.6% (4 of 725) for 2--12 weeks' gestation, 1.4% (9 of 642) for 13--28 weeks, and 0 (0 of 385) after
28 weeks.
In a prospective study of 1,373 mothers with varicella during pregnancy conducted in the United Kingdom and
West Germany during 1980--1993, the highest risk (2%) for congenital varicella syndrome was observed when maternal
infection occurred during 13--20 weeks' gestation
(43). The risk was 0.4% after maternal infection during 0--12 weeks' gestation.
No cases of congenital varicella syndrome occurred among the infants of 366 mothers with HZ during pregnancy. Nine
isolated cases involving birth defects consistent with congenital varicella syndrome have been reported after maternal varicella
beyond 20 weeks' gestation (with the latest occurring at 28 weeks)
(47,48). In a prospective study, HZ occurred
during infancy or early childhood in four (0.8%) of 477 infants who were exposed to VZV during 13--24 weeks' gestation and in six (1.7%)
of 345 infants who were exposed during 25--36 weeks' gestation
(43).
The onset of varicella in pregnant women from 5 days
before to 2 days after delivery results in severe varicella infection in
an estimated 17%--30% of their newborn infants. These infants are exposed to VZV without sufficient maternal
antibody to lessen the severity of disease. The risk for neonatal death has been estimated to be 31% among infants whose mothers
had onset of rash <4 days before giving birth
(45). This estimate was made on the basis of a limited number of infant deaths
and might be higher than the actual risk because the study was performed before neonatal intensive care was available. In
addition, certain cases were not part of prospective studies but were reported retrospectively, making the results subject to selection
bias. When these cases were reevaluated subsequently by another investigator, certain
infants were demonstrated to have been at
higher risk for death because of low birthweight; in at least one case, another cause of death was probable
(46). Varicella-zoster immune globulin (VZIG) has been reported to reduce incidence of severe neonatal varicella disease
(49) and therefore is indicated in such situations. Nevertheless, the risk for death among neonates who do not receive postexposure
prophylaxis with VZIG is likely to be substantially lower than was estimated previously.
Herpes Zoster Surveillance
After primary infection, VZV persists as a latent infection in sensory-nerve ganglia. The virus can reactivate, causing
HZ. Mechanisms controlling VZV latency are not well understood. Risk factors for HZ include aging, immunosuppression,
and initial infection with varicella in utero or during early childhood (i.e., age <18 months). An estimated 15%--30% of
the general population experience HZ during their lifetimes
(50,51); this proportion is likely to increase
as life expectancy increases. The most common complication of HZ, particularly in older persons, is postherpetic neuralgia (PHN),
the persistence of sometimes debilitating pain weeks to months after resolution of HZ.
Life-threatening complications of HZ also can occur; these include herpes ophthalmicus, which can lead to blindness. Another severe manifestation is
dissemination, which might involve generalized skin eruptions, and central nervous system, pulmonary, hepatic, and
pancreatic complications. Dissemination, pneumonia, and
visceral involvement typically are restricted to immunocompromised
persons. VZV can be transmitted from the lesions of patients who have HZ to susceptible contacts. Although few data are available
to assess this risk, one household contact study reported
that the risk for VZV transmission from HZ was approximately
20% of the risk for transmission from varicella
(52).
Varicella vaccination might alter the risk for HZ at the level of both the individual and the population (i.e., herd
immunity). Just as wild-type VZV can cause wild-type HZ, attenuated vaccine virus has the potential to become latent and later reactivate
to cause vaccine virus strain (also called Oka-strain) HZ
(53). Multiple studies have evaluated the risk for Oka-strain HZ
after vaccination of immunocompromised or healthy children
(54--58). In a study of leukemic children, the rate of HZ after a
mean 4.1 years of follow-up (range: 6 months--10 years) was 2% in vaccine recipients and 15% in controls with a history of
varicella (54). A subset of 96 of these vaccine recipients was matched prospectively according to chemotherapeutic protocol with
96 leukemic children who had experienced natural varicella. Analysis indicated that the incidence of HZ was
approximately three times lower in vaccine recipients (0.80 per 100 person-years) than in the matched leukemic children who had experienced
natural varicella (2.46 per 100 person-years) (p = 0.01). Data for healthy children are more limited, and findings might be influenced
by multiple factors (e.g., incomplete ascertainment, limited duration of follow up or no follow up of subjects of older ages,
no comprehensive screening for wild-type varicella infection before or after vaccination, or lack of testing all cases to distinguish
Oka- from wild-type HZ). Nonetheless, these studies suggest that the risk for Oka-strain HZ after a single dose of varicella vaccine
is lower than that after wild-type varicella infection
(56--58). Over time, the risk for and manifestation of Oka-strain HZ should
be examined in older persons who are at greater risk for HZ complications. Persons who experience varicella infection
before vaccination (i.e., as a result of in utero or unapparent infection) or after vaccination (i.e., as a result of breakthrough
infection) presumably are latently infected with two strains of VZV. The risk for HZ in these persons is unknown. No long-term
studies have been conducted that compare the risk for Oka-strain HZ in persons who receive 1 dose of varicella vaccine with the risk
for those who receive 2 doses.
Varicella vaccination also might change the risk for HZ at the population level. With the development of herd
immunity and reduction in the likelihood of exposure, the varicella vaccination program prevents wild-type VZV infection
among vaccine recipients and nonvaccine recipients, eliminating the risk for wild-type HZ in these persons. Reduction in
the likelihood of wild-type varicella infection also increases the
median age for acquiring varicella (although age-specific
incidence rates themselves are lower). This reduces the risk for varicella infection during early childhood (i.e., age <18 months),
thereby reducing a risk factor for childhood HZ.
Exposure of persons with latent wild-type VZV infection to persons with varicella is thought to boost specific
immunity, which might contribute to controlling reactivation of VZV and the development of HZ
(50). Concern has been expressed that by providing fewer opportunities for varicella exposure among persons with previous wild-type varicella
infection, reduction in the likelihood of exposure might
increase the risk for HZ, possibly within as few as 5 years after introduction of
varicella vaccination (59) and reaching a vaccination
coverage of >90%.
Herpes zoster is not a nationally notifiable disease in the United States, and HZ surveillance has been conducted
using multiple methods, study sites, or data sources. For certain studies, baseline data were available before the start of the
varicella vaccination program. One study that included baseline data was a retrospective analysis of electronic medical records from
a health maintenance organization (HMO) during 1992--2002
(60). This HMO study indicated that age-adjusted incidence
of HZ remained stable during 1992--2002 as incidence of
varicella decreased (60). Age-adjusted and -specific
annual incidence rates of HZ fluctuated slightly over time; the age-adjusted rate was highest in 1992, at 4.1 cases per 1,000
person-years, and was 3.7 cases per 1,000 person-years in 2002. For other studies initiated in the postvaccine era, baseline data are
not available (61--63). An analysis of national incidence data from the Medstat database (available at
http://www.medstat.com/Products/view/?id=71) demonstrated
an overall incidence of HZ in 2000 and 2001 of 3.2 (95% confidence interval [CI]
= 3.1--3.2) per 1,000 person-years (61), representing no increase in age-adjusted HZ in the past 20 years in the United
States compared with earlier published data
(64). Data from two HMOs in Oregon and Washington for 1997--2003 indicated
no statistically significant increase in HZ incidence rates except among
children aged 10--17 years (relative risk [RR] = 1.12, CI
= 1.05--1.18); these increases were attributed to increased use of oral steroids
(62). Another study of data gathered from a statewide telephone survey during 1999--2003 in Massachusetts demonstrated an increase in HZ
(63). Age groups particularly affected included persons aged 25--44 years and those aged >65 years. Finally, in the two active varicella surveillance
sites (Antelope Valley, California, and West Philadelphia, Pennsylvania), active surveillance for HZ in children aged <20 years
has been ongoing since 2000. During 2000--2004, incidence of HZ in children aged <10 years declined significantly
(p<0.05) from 0.75 to 0.23 cases per 1,000 children
(65; CDC unpublished data, 2006). In summary, multiple studies and
surveillance data demonstrate no consistent trends in HZ incidence in the United States since implementation of the varicella
vaccination program in 1995.
Use of Acyclovir to Treat and Prevent Varicella
Acyclovir is a synthetic nucleoside analog that inhibits replication of human herpes viruses, including VZV. Since the
early 1980s, intravenous acyclovir has been available to treat immunocompromised persons who have varicella.
When administered within 24 hours of onset of rash, acyclovir has been demonstrated to be effective in reducing
varicella-associated morbidity and mortality in this population
(66--68).
In 1992, the Food and Drug Administration (FDA)
approved the use of oral acyclovir for the treatment of varicella
in otherwise healthy children. This approval was made on the basis of placebo-controlled, double-blind studies
(69,70) that demonstrated the beneficial clinical effects (i.e., a decrease in the number of days in which new lesions appeared, the
duration of fever, and the severity of cutaneous and systemic signs and symptoms) that occurred when acyclovir was
administered within 24 hours of rash onset. No serious adverse events occurred during the period of drug
administration. Administration of acyclovir did not decrease transmission of varicella or reduce the duration of absence from school. Because few
complications occurred (1%--2%), these studies could not determine whether acyclovir had a statistically significant effect on disease
severity among healthy children. In these studies, antibody titers after infection in children receiving acyclovir did not
differ substantially from titers of children in the control group
(69,70). Clinical trials among adolescents and adults have
indicated that acyclovir is well-tolerated and effective in
reducing the duration and severity of clinical illness if the drug is
administered within 24 hours of rash onset
(71--73).
In 1993, AAP's Committee on Infectious Diseases published a statement
regarding the use of acyclovir (74). AAP did
not consider administration of acyclovir to healthy children to have clinical benefit sufficient to justify its routine
administration; however, AAP stated that certain circumstances might justify its use. AAP recommended that oral acyclovir should
be considered for otherwise healthy persons at increased risk for moderate to severe varicella (e.g., persons aged >12 years,
persons with chronic cutaneous or pulmonary disorders, persons
receiving long-term salicylate therapy, and persons receiving
short, intermittent, or aerosolized courses of corticosteroids). Certain experts also recommend use of oral acyclovir
for secondary case-patients who live in the same households as infected children
(74).
Acyclovir is classified as a Category B drug in the FDA
use-in-pregnancy rating. Although studies involving animals
have not indicated teratogenic effects, adequate, well-controlled studies in pregnant women have not been conducted.
However, a prospective registry of acyclovir use during pregnancy that collected data on outcomes of 596 infants whose mothers
were exposed to systemic acyclovir during the first trimester of pregnancy indicated that the rate and types of birth
defects
approximated those in the general population
(75). AAP has not recommended routine use of oral acyclovir for
pregnant women because the risks and benefits to the fetus and mother were unknown. However, in instances of serious,
viral-mediated complications (e.g., pneumonia), AAP has recommended that intravenous acyclovir should be considered
(74).
Two nucleoside analogs, acyclovir and famciclovir, have been approved by FDA for treating HZ. If administered within
72 hours of rash onset, acyclovir has accelerated the rate of cutaneous healing and reduced the severity of acute pain in adults
who have HZ (76). Oral famciclovir, when administered
during the same period, has similar efficacy
(77).
Acyclovir is not indicated for prophylactic use among
otherwise healthy children, adolescents, or adults without evidence
of immunity after exposure to varicella. Vaccination is the method of choice in these situations. No studies have been
conducted regarding prophylactic use of acyclovir among immunocompromised persons; therefore, VZIG is recommended in
these situations.
Vaccines for Prevention of Varicella
Two live attenuated varicella virus vaccines are licensed in the United States for prevention of varicella:
single-antigen varicella vaccine
(VARIVAX,® Merck & Co., Inc., Whitehouse Station, New Jersey) and combination MMRV
vaccine (ProQuad,® Merck & Co., Inc., Whitehouse, New Jersey). Both vaccines are derived from the Oka strain of live,
attenuated VZV. The Oka strain was isolated in Japan
(78) in the early 1970s from vesicular fluid in a healthy child who had
natural varicella and was attenuated through sequential propagation in cultures of human embryonic lung cells,
embryonic guinea-pig cells, and human diploid cells (WI-38). The virus in the Oka/Merck vaccine has undergone further passage through
human diploid-cell cultures (MRC-5) for a total of 31 passages.
In 1995, the single-antigen varicella vaccine was licensed in the United States for use among healthy persons aged
>12 months. This vaccine is lyophilized; when reconstituted as directed in the package insert and stored at room temperature for
a maximum of 30 minutes, it contains a minimum of 1,350 plaque forming units (PFUs) of Oka/Merck VZV in each 0.5
mL dose (79). Each dose also contains 12.5 mg of hydrolyzed gelatin, trace amounts of neomycin and fetal bovine serum, 25
mg of sucrose, and trace residual components of MRC-5 cells (including DNA and protein). The vaccine does
not contain preservatives. Since 1995, >55 million doses have been distributed in the United States. Reporting of serious
adverse events has been rare (see Vaccine-Associated Adverse Events).
In 2005, the combination MMRV vaccine was licensed in the United States for use among healthy children aged
12 months--12 years. The attenuated measles, mumps, and rubella vaccine viruses in
ProQuad® are identical and of equal titer
to those in the measles, mumps, and rubella (MMR) vaccine,
MMRII® (80). The titer of Oka/Merck VZV is higher in
MMRV than in single-antigen varicella vaccine, a minimum of 3.99
log10 PFUs compared with 1,350 PFUs (approximately
3.13 log10) in each 0.5 mL dose. The other constituents are similar to those in the single-antigen varicella vaccine.
Immune Response to Vaccination
In clinical trials of the single-antigen varicella vaccine conducted before licensure, seroconversion was assessed using lots
of vaccine with different amounts of PFUs and laboratory
assays with different levels of sensitivity and specificity. Using
a specially developed, sensitive gp-enzyme-linked immunosorbent assay (ELISA) test that is not available
commercially, seroconversion (defined by the acquisition of any detectable varicella antibodies >0.3 gpELISA units) was
observed at approximately 4--6 weeks after vaccination with
1 dose of varicella vaccine in approximately 97% of 6,889
susceptible children aged 1--12 years (79). The seroconversion rate was 98% for children aged 12--15 months and 95% among those
aged 5--12 years (81). Adolescents aged 13--17 years had a lower seroconversion rate (79%) after a single dose of vaccine. A
study performed postlicensure used fluorescent antibody
to membrane antigen (FAMA) titers 16 weeks after vaccination to
assess serologic response and demonstrated that 61 (76%) of 80 healthy child vaccine recipients seroconverted (FAMA titers
>1:4) after 1 dose of single-antigen varicella
vaccine (82).
Primary antibody response to the vaccine at 6 weeks postvaccination is correlated with protection against disease
(83,84). In clinical trials, rates of breakthrough disease were lower among children with varicella antibody titers of
>5 gpELISA units than among those with titers of <5 units
(84); children with a 6-week postvaccination antibody titer of <5 gpELISA units were
3.5 times more likely to have breakthrough varicella than those with a titer of
>5 gpELISA units. Later studies of
immunogenicity
(85) have reported the proportion of vaccinated children who achieved this antibody level
instead of seroconversion. After 1 dose of the
single-antigen varicella vaccine, 86% of children had gpELISA levels of
>5 units/mL (85). Studies performed
using FAMA indicated that a titer >1:4 at 16 weeks postvaccination is correlated with protection against disease
(82). Of healthy persons with a titer of >1:4 at 16 weeks post vaccination, <1% have had varicella after a household exposure (n = 130).
In contrast, the attack rate among those with a titer of <1:4 was 55% (n = 60).
Persistence of antibody in children after 1 dose of single-antigen varicella vaccine was demonstrated in both short- and
long-term follow-up studies. In a clinical study, the rate of antibody persistence detected by gpELISA was nearly 100% after 9
years of follow-up for 277 children (85). Another study demonstrated that although antibody titers (detected by FAMA)
might decline 12--24 months after vaccination, the median titer did not change after 1--4 years and even rose after 10 years
(86). In Japan, VZV antibodies were present in 37 (97%) of 38 children who received varicella vaccine 7--10 years earlier (with
titers comparable to those of 29 children who had had natural varicella infection within the previous 10 years)
(87) and in 100% of 25 children when followed for as long as 20 years (i.e., antibody levels were higher than those observed 10 years earlier)
(88). Interpretation of long-term studies is complicated by at least two factors. First, asymptomatic boosting of
vaccine-induced immunity by exposure to wild-type VZV is likely. Because varicella vaccine is not routinely recommended in Japan,
coverage of children was estimated to be low (approximately 20%) during 1991--1993. Second, sample sizes were limited as a result
of the decrease in the number of children followed-up with increasing time since vaccination.
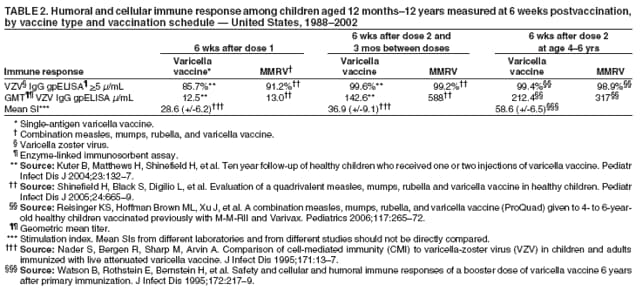
The second dose of varicella vaccine in children produced an improved immunologic response that is correlated
with improved protection. A comparative study of healthy children who received 1 or 2 doses of single-antigen varicella
vaccine administered 3 months apart indicated that a second dose provided higher antibody levels as measured by the proportion
of subjects with titers of >5 gpELISA units and by
geometric mean titers (GMTs) and higher efficacy
(85; Tables 2--4). The proportion of subjects with antibody titers of
>5 gpELISA units in the 2-dose recipients was higher 6 weeks after the
second dose than after the first dose (99.6% and 85.7%, respectively) and remained high at the end of the 9-year follow-up
period, although the difference between the two regimens narrowed (97% and 95%, respectively). GMT 6 weeks after the
second dose was substantially higher than that after a single dose (142 and 12, respectively). The difference in GMTs between the
two regimens did not persist over 9 years of follow-up among subjects who seroconverted after vaccination, although GMTs
in both regimens remained high by the end of the study period. However, receipt of a second dose decreased the rate
of breakthrough varicella significantly (3.3-fold) and increased vaccine efficacy (p<0.001). Another study that assessed
the immunogenicity of a second dose received 4--6 years after the first dose demonstrated a substantial increase in antibody
levels in the first 7--10 days in the majority of those tested, indicating an anamnestic response. On the day of the second dose,
GMT was 25.7, compared with 143.6 GMT 7--10 days after the second dose; 60% of recipients had at least a fourfold increase
in antibody titers, and an additional 17% had at least a twofold increase
(89). Three months after the second dose,
GMT remained higher than on the day of second dose (119.0 and 25.7, respectively). Among children, VZV antibody levels
and GMTs after 2 doses administered 4--6 years apart were comparable to those
obtained when the 2 doses were administered 3 months apart.
The combination MMRV vaccine was licensed on the basis of noninferiority of immunogenicity of the
antigenic components compared with MMR and varicella vaccines administered concomitantly at separate inspection sites rather
than on clinical efficacy (80). Clinical studies of healthy children aged 12--23 months indicated that those who received 1 dose
of MMRV vaccine had levels of antibody to measles, mumps, rubella, and varicella similar to levels of children who received
1 dose of MMR and 1 dose of varicella vaccines concomitantly at separate injection sites. For the varicella component
in MMRV, 91.2% (CI = 87.0%--94.4%) of children achieved antibody titers of
>5 gpELISA units/mL 6 weeks after
vaccination (90). A subgroup of children received a second dose of MMRV vaccine approximately 3 months after the first dose.
The serologic response (>5 gpELISA units/mL) after 2 doses was 99.2% (CI = 97.0%--99.9%) (Table 2). Also, GMT for
varicella after the second dose of MMRV vaccine increased approximately
forty-onefold (90). Administration of combination
MMRV vaccine to healthy children aged 4--6 years who had been vaccinated previously with MMR and single-antigen
varicella vaccines resulted in similar antibody levels and a
twenty-fivefold increase in GMT levels (91).
Among persons aged >13 years, multiple studies have
described seroconversion rates after receipt of the
single-antigen varicella vaccine (range: 72%--94% after 1 dose and 94%--99% after a second dose administered 4--8 weeks
later) (79,92,93). In clinical studies, detectable antibody levels have persisted for at least 5 years in 97% of adolescents and
adults who were administered 2 doses of vaccine 4--8 weeks apart
(79). However, other studies demonstrated that 25%--31%
of
adult vaccine recipients who seroconverted lost detectable antibodies (by FAMA) at multiple intervals (range: 1--11
years) after vaccination (93,94). For persons who had breakthrough disease after exposure to varicella, the severity of illness or
the attack rates did not increase over time
(95).
Innate (i.e., nonspecific) and adaptive (i.e., humoral and cellular) immunity are important in the control of primary
varicella infection. The capacity to elicit cell-mediated immunity is important for viral clearance, providing
long-term protection against disease and preventing symptomatic VZV reactivation. Studies among children and adults have
indicated that breakthrough varicella typically is mild, even among vaccine recipients without seroconversion or vaccine recipients
who lost detectable antibody, suggesting that VZV-specific
cell-mediated immunity affords protection to vaccine recipients in
the absence of a detectable antibody response
(94,95). Studies of the cellular immune response to vaccination among
children demonstrated that immunization with 1
dose of varicella vaccine induced VZV-specific T-cell proliferation that
was maintained in 26 (90%) of 29 children 1 year postvaccination and in 52 (87%) of 60 children 5 years postvaccination
(96). In this study, the mean stimulation index (SI), a marker of cell-mediated immunity, was 12.1 after
1 year and 22.1 after 5 years. Data obtained at 1 year postvaccination from a subset of children in a prelicensure study comparing the immune
response among children who received 1 and 2 doses administered 3 months apart demonstrated that the
varicella-specific lymphocyte proliferation responses were significantly higher for recipients of 2 doses than for recipients of 1 dose (mean SI: 34.7 and
23.1, respectively; p = 0.03) (97). In the study of the 2 doses administered 4--6 years apart, results also indicated that
the lymphocyte proliferation response was significantly higher at 6 weeks and 3 months after the second dose than at the
same time points after the first dose (p<0.01)
(89; Table 2).
Among adults, vaccine-induced VZV-specific T-cell proliferation was maintained in 16 (94%) of 17 subjects 1 and 5
years postvaccination (96,98). The mean SI was 9.9 after 1 year and 22.4 after 5 years.
Correlates of Protection
For children, the varicella antibody response measured by gpELISA 6 weeks postvaccination correlates with
neutralizing antibody level, VZV-specific T-cell proliferative responses, vaccine efficacy, and long-term protection against varicella
after exposure to VZV (83,84,99,100). A titer of
>5 gpELISA units/mL is associated with protection against disease although
it should not be considered an absolute guarantee of protection. Breakthrough cases have occurred among children with
>5 gpELISA units/mL. A FAMA titer
>1:4 at 16 weeks post-vaccination also correlates with protection against disease
(82). However, neither of these antibody tests is available commercially. The relationship between the antibody level measured
at other intervals postvaccination, especially immediately prior to
exposure and breakthrough disease has not been studied.
No correlates of protection have been evaluated for adults.
Vaccine Efficacy and Vaccine Effectiveness
One-Dose Regimen
Prelicensure Efficacy
In prelicensure studies carried out among children aged
12 months--14 years, the protective efficacy of
single-antigen varicella vaccine varied, depending on the amount of live
virus administered per dose, the exposure setting (community
or household), and the quality and length of the clinical follow-up. The majority of the prelicensure studies reported efficacy of
1 dose of varicella vaccine within the range of 70%--90% against any clinical disease and 95% against severe disease for
7--10 years after vaccination (81,101,102). A randomized placebo-controlled efficacy trial was conducted among children aged
12 months--14 years, but the formulation differed from that of the current vaccine (17,000 PFUs per dose
(103,104), with follow-up of children through 7 years postvaccination
(105). Reported efficacy was 100% at 1 year and 98% at 2 years
after vaccination, and 100% and 92%, respectively, after exposures to VZV that occurred in the household. Although a
randomized control study was not conducted for adults, the efficacy of single-antigen varicella vaccine was
determined by evaluation of protection when adult vaccine recipients were exposed to varicella in the household. On the basis of the reported
historical
attack rate of 87% for natural varicella after household exposure among unvaccinated children, estimated efficacy
among adults was approximately 80% (79). The attack rate of unvaccinated adults exposed in households was not studied.
Postlicensure Efficacy and Effectiveness
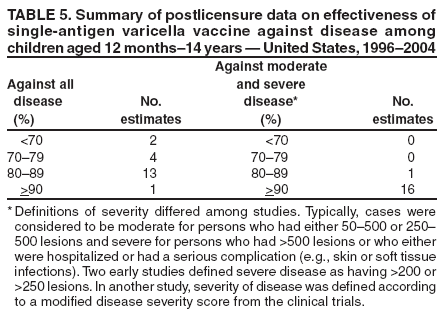
Prevention of All Varicella Disease
Postlicensure studies have assessed the
effectiveness¶ of the single-antigen varicella vaccine under field conditions in
child care, school, household, and community settings using multiple methods. Effectiveness frequently has been estimated
against all varicella and also against moderate and severe varicella (defined in different ways). Outbreak investigations
have assessed effectiveness against clinically defined varicella. The majority of these investigations have demonstrated
vaccine effectiveness for prevention of varicella in the same range
described in prelicensure trials (70%--90%)
(3--6,106--113), with some lower (44%, 56%)
(114,115) and some higher (100% in one of two schools investigated) estimates
(107). A retrospective cohort study in 11 childcare centers demonstrated vaccine effectiveness of 83% for prevention of
clinically diagnosed varicella (116). In a case-control study that measured vaccine effectiveness against laboratory-confirmed varicella
in a pediatric office setting during 1997--2003, vaccine effectiveness was 85% (CI = 78%--90%) during the first four years
and 87% (CI = 81%--91%) for the entire study period
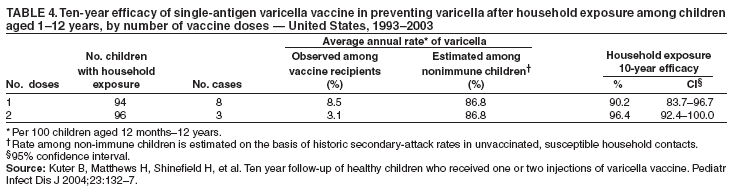
(117,118). Finally, in a study of household secondary attack
rates, considered the most robust test of vaccine performance because of the intensity of exposure, varicella vaccine was 79% (CI
= 70%--85%) effective in preventing clinically defined varicella in exposed household contacts aged 12 months--14
years without a history of varicella disease or vaccination
(119). Postlicensure data on vaccine effectiveness against all disease
have been summarized (Table 5).
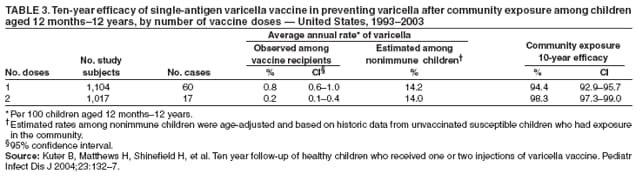
In a randomized clinical trial conducted postlicensure that compared the efficacy of 1 dose of varicella vaccine with that of
2 doses, the estimated vaccine efficacy for 1 dose for a
10-year observation period was 94.4% (CI = 92.9%--95.7%)
(85; Table 3). In the same study, the efficacy of 1 dose of vaccine in preventing varicella after household exposure for 10 years was
90.2% (CI = 83.7%--96.7%) (Table 4). This study did not use placebo controls and used historic data for attack rates
in unvaccinated children to calculate vaccine
efficacy.
Prevention of Moderate and Severe Varicella
Postlicensure studies assessing vaccine performance in
preventing moderate and severe varicella have
consistently demonstrated high effectiveness. Definitions for disease
severity have varied among studies. Certain studies have used
a defined scale of illness that included the number of skin
lesions, fever, complications, and investigator assessment of
illness severity, and others have used only the number of skin
lesions, reported complications, or hospitalizations.
Moderate varicella typically has been defined as either 50--500 or 250--500 lesions, and severe varicella has been defined as >500 lesions or
any hospitalization or complication. In the randomized postlicensure clinical trial, severe varicella was defined as >300 lesions
and fever of >102°F (38.9°C), oral equivalent.
Regardless of different definitions, multiple studies have
demonstrated that single-antigen varicella vaccine was>>95% effective in preventing combined moderate and severe disease
(3--6,85,106,107,109--113,115--119); one study demonstrated effectiveness of 86%
(114). Effectiveness was 100% against severe disease
when measured separately
(6,85,109,111,117,119). Postlicensure data on vaccine effectiveness against moderate and severe
varicella have been summarized (Table 5).
Two-Dose Regimen
In a randomized clinical trial of single-antigen varicella vaccine that compared the efficacy of 1 dose with that of 2
doses administered 3 months apart, the estimated vaccine efficacy of 2 doses for a 10-year observation period was 98.3% (CI
= 97.3%--99.0%), which was significantly higher than efficacy after 1 dose (p<0.001)
(85; Table 5). The 2-dose regimen also was 100% efficacious against severe varicella. In the same study, the efficacy of 2 doses of single-antigen varicella vaccine
in preventing disease after household exposure over 10 years was 96.4% (CI = 92.4%--100%), not significantly different from
1 dose (90.2%) (p = 0.112) (Table 4). However, the number of cases involving household exposure was limited.
Formal studies to evaluate the clinical efficacy of the combination MMRV vaccine have not been performed. Efficacy of
the individual components was established previously in clinical studies with the single-antigen vaccines.
Breakthrough Disease
Breakthrough disease is defined as a case of infection with wild-type VZV occurring >42 days after vaccination. In
clinical trials, varicella disease was substantially less severe among vaccinated persons than among unvaccinated persons, who
usually have fever and several hundred vesicular lesions
(120). In cases of breakthrough disease, the median number of skin lesions
is commonly <50 (99,121--123). In addition,
compared with unvaccinated persons, vaccine recipients have had fewer
vesicular lesions (lesions more commonly are atypical, with papules that do not progress to vesicles), shorter
duration of illness, and lower incidence of fever.
Multiple postlicensure investigations also have demonstrated that the majority of breakthrough varicella cases
are significantly milder than cases among unvaccinated children (p<0.05)
(3,5,107--114,116--118,124). However,
approximately 25%--30% of breakthrough cases are not mild, with clinical features more similar to those in unvaccinated children
(124). Since 1999, when varicella deaths became nationally notifiable, two deaths from breakthrough varicella disease have
been reported to CDC; one of a girl aged 9 years with a history of asthma who was receiving steroids when she had
the breakthrough infection, and the other of a girl aged 7 years with a history of malignant ependymoma who also was
under steroid therapy at the time of her death (CDC, unpublished data, 2006).
One-Dose Regimen
In clinical trials, 1,114 children aged 1--12 years received
1 dose of single-antigen varicella vaccine containing
2,900--9,000 PFUs of attenuated virus per dose and were actively followed for up to 10 years postvaccination
(79). Among a subset of 95 vaccine recipients with household exposure to varicella, eight (8%) reported a mild form of varicella (10--34 lesions).
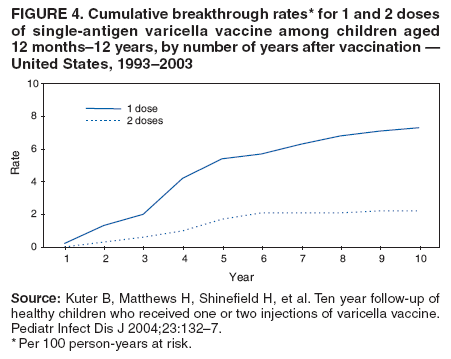
In a randomized clinical trial that compared the efficacy of 1 dose of vaccine to that of 2 doses during a 10-year
observation period, the cumulative rate of breakthrough varicella among children who received 1 dose was 7.3%
(85). Breakthrough cases occurred annually in 0.2%--2.3% of recipients of 1 dose of vaccine. Cases occurred throughout the observation period,
but the majority were reported 2--5 years after vaccination (Figure 4). Of 57 children with breakthrough cases, 13 (23%) had
>50 lesions.
In cross-sectional studies, the attack rate for breakthrough disease has ranged between 11% and 17% (and as high as 40%
in certain classrooms) in outbreak investigations
(3) and 15% in household settings
(119).
Two-Dose Regimen
Data Among Children
In a randomized clinical trial that compared the efficacy of 1 dose of vaccine with that of 2 doses, the cumulative rate
of breakthrough varicella during a 10-year observation period was 3.3-fold lower among children who received 2 doses than
that among children who received 1 dose (2.2% and 7.3,
respectively; p<0.001) (85). Breakthrough cases occurred
occasionally in 0.8% of 2-dose vaccine recipients. The
majority of cases of breakthrough disease occurred 2--5 years after vaccination; no
cases were reported 7--10 years after vaccination (Figure 4). Of 16 children with breakthrough cases, three (19%) had >50
lesions. The proportion of children with >50 lesions did not differ between the 1-dose and 2-dose
regimens (p = 0.5).
Breakthrough Infections Among Adolescents and Adults
In postlicensure studies of adolescents and adults who
received 2 doses, 40 (9%) cases of breakthrough
varicella occurred among 461 vaccine recipients who were followed for 8 weeks--11.8 years (mean: 3.3 years) after vaccination
(95), and 12 (10%) cases occurred among 120 vaccine recipients who were followed for 1 month--20.6 years (mean: 4.6
years) (94). One prelicensure study of persons who had
received 2 doses of vaccine reported that 12 (8%) breakthrough cases
had occurred among 152 vaccine recipients who were followed for 5--66 months (mean: 30 months) postvaccination
(93).
Contagiousness
Prelicensure clinical trials reported the rate of disease transmission from vaccinated persons with varicella cases to
their vaccinated siblings. In 10 trials that were conducted during 1981--1989, breakthrough infections occurred in 114 (5.3%)
of 2,163 vaccinated children during the 1--8 year follow-up period of active surveillance, and secondary transmission occurred
to 11 (12.2%) of their 90 vaccinated siblings
(121). Illness was mild in both index and secondary case-patients.
Household
transmission from a vaccinated child with breakthrough disease to a susceptible adult (one of whom died) have been
reported (CDC, unpublished data, 2006). One study examined secondary attack rates from vaccinated and unvaccinated persons
with varicella to both vaccinated and unvaccinated households contacts aged 12 months--14 years
(119). This study demonstrated that vaccinated persons with varicella with <50 lesions were only one third as contagious as unvaccinated persons
with varicella. However, vaccinated persons with varicella who had
>50 lesions were as contagious as unvaccinated persons
with varicella (119). Vaccinated persons with varicella tend to have milder disease, and, although they are less contagious
than unvaccinated persons with varicella, they might not receive a diagnosis and be isolated. As a result, they might have
more opportunities to infect others in community settings, thereby further contributing to VZV transmission. Vaccinated
persons with varicella also have been index case-patients in varicella outbreaks
(3,4,115).
Risk Factors for Vaccine Failure
Potential risk factors for vaccine failure have been identified in studies of vaccine effectiveness during outbreak
investigations and other specially designed studies
(5,108--110,113--115,118,125). In outbreak investigations, the low number of
cases limits the ability of researchers to conduct multivariate analyses and examine the independent effect of each risk factor
for vaccine failure. An increased risk for breakthrough disease has been noted with decreasing age at vaccination, with a
threefold increase in breakthrough disease risk for children vaccinated at age <14 months
(110), an increase of twofold in one study
and nearly fourfold in another for children vaccinated at age <16 months
(108,115), and a ninefold increase for
children vaccinated at age <19 months
(113). Other outbreak investigations have demonstrated that time since vaccination
(variably defined as >3, >5, or
>5 years) was associated with an increased risk for breakthrough disease (relative risk [RR] = 2.6, 6.7,
and 2.6, respectively) (5,114,115). However, age at vaccination and time since vaccination are highly correlated, and
their independent association with the risk for breakthrough disease has been assessed in only one outbreak investigation
(113). A retrospective cohort study that adjusted for other potential risk factors demonstrated an increased risk for breakthrough
disease for children vaccinated at age <15 months (adjusted relative risk [aRR] = 1.4; CI = 1.1%--1.9%)
(125). A case-control study demonstrated that the effectiveness of vaccine in the first year after vaccination was significantly lower (73%) among
children vaccinated at age <15 months than it was among children vaccinated at age
>15 months (99%) (p = 0.01) (118). However,
the difference in the overall effectiveness between children vaccinated at these ages was not statistically significant for
subsequent years (8 years of follow-up) (81% and 88%, respectively; p = 0.17). Active surveillance data collected during 1995--2004
from a sentinel population of 350,000 persons were analyzed to
determine whether the severity and annual incidence
of breakthrough varicella cases increased with time since vaccination
(126). Children vaccinated >5 years previously were
2.6 times more likely to have moderate and severe breakthrough
varicella than those vaccinated <5 years previously (p =
0.016). The annual rates of breakthrough varicella among children aged 12 months--12 years increased significantly with time
since vaccination after adjusting for the effects of age at infection, age at vaccination, and year of infection (p<0.01).
Multiple other studies that examined possible reasons for lower vaccine effectiveness did not find age at vaccination
(3--5,111,114) or time since vaccination
(3,110,111) to be associated with vaccine failure. An ongoing study is examining
these factors and risk for vaccine failure
(127). After 8 years of active follow-up of 7,449 children vaccinated at age 12--23
months, results do not indicate an increased risk for breakthrough disease among children vaccinated at age 12--14 months
compared with those vaccinated at age 15--23 months. Moreover, a test for trend revealed no change in the rate of
reported breakthrough disease for each additional month of age at vaccination
(127).
Two outbreak investigations noted an increased risk for breakthrough disease in children with asthma and
eczema (109,113). In these investigations, the use of steroids to treat asthma or eczema was not studied. Steroids have been
associated previously with severe varicella in unvaccinated persons
(128--130). Only one retrospective cohort study
controlled simultaneously for the effect of multiple risk factors, including the use of steroids, and this study demonstrated no
association of risk for breakthrough disease with asthma or eczema
(125). However, this study documented an increased risk
for breakthrough disease if the child had received a prescription of oral steroids (considered a proxy for taking oral steroids
when exposed to varicella) within 3 months of breakthrough disease (adjusted RR [aRR] = 2.4; CI = 1.3%--4.4%) and
when varicella vaccination was administered within 28 days of MMR vaccine (aRR = 3.1; CI = 1.5%--6.4%).
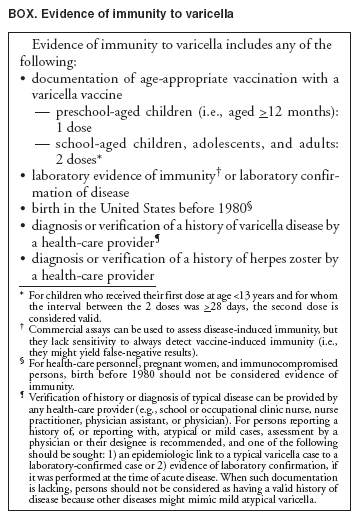
Evidence of Immunity
ACIP has approved criteria for evidence of immunity to varicella (Box). Only doses of varicella vaccines for which
written documentation of the date of administration is presented should be considered valid. Neither a self-reported dose nor a
history of vaccination provided by a parent is, by itself, considered adequate evidence of immunity. Persons who lack
documentation of adequate vaccination or other evidence of
immunity should be vaccinated.
Historically, self-reporting of varicella disease by adults or by parents for their children has been considered valid evidence
of immunity. The predictive value of a self-reported positive disease history was extremely high in adults in the prevaccine
era although data on positive predictive value are lacking in parental reports regarding their children
(131--133). As disease incidence decreases and the proportion of vaccinated persons with varicella having mild cases increases, varicella will be
less readily recognized clinically. A recent study demonstrated that only 75% of unvaccinated children aged 12
months--4 years who reported a positive history of
varicella were in fact immune (confirmed by serological testing), compared with 89%
of children aged 5--9 years and 10--14 years
(134). To limit the number of false-positive
reports and ensure immunity, ACIP recommends that evidence of immunity should be either a diagnosis of varicella by a health-care provider or a
health-care provider verification of a history of disease rather than parental or
self-reporting. The above-cited study demonstrated
that 99% of persons aged 15--19 years and 100% of those aged 20--29 years who
reported a history of varicella were immune
(134). Because serologic evidence of VZV infection
has been documented in 96%--97% of U.S.-born adults aged 20--29
years and in 97%--99% of adults aged >30 years tested during 1998--1999
(12), U.S. birth before 1980 is considered evidence
of immunity except for health-care personnel (HCP), pregnant women, and immunocomprised persons. For these three
groups, certainty regarding immunity is desirable because of the possibility of nosocomial transmission to
high-risk patients; transmission of the virus to the fetus, which might result in congenital
varicella syndrome; and the possibility of severe disease. Postvaccination serologic testing to verify an immune response to varicella vaccine is not
routinely recommended because available commercial assays lack sensitivity in detecting vaccine-induced immunity and might give
false negative results.
Simultaneous Administration of Vaccines
Single-antigen varicella vaccine is well-tolerated and effective in healthy children aged
>12 months when administered simultaneously with MMR vaccine either at separate sites and with separate syringes or separately
>4 weeks apart. The number and types of adverse events occurring in children who have received VARIVAX and MMRII concurrently have not
differed from those in children who have been administered the vaccines at different visits
(79,135). Data concerning the effect of simultaneous administration of VARIVAX with vaccines containing various combinations of MMR, diphtheria and
tetanus toxoids and pertussis (DTP), and Haemophilus
influenzae type b (Hib) have not been published
(79). A randomized study of 694 subjects determined that the immune response to MMR, varicella, and Hib vaccines administered concurrently with
a fourth dose of pneumococal conjugate vaccine (PCV7) was not inferior to that of those vaccines when administered
without PCV7; the percentage of subjects who seroconverted was >90% for all antigens for both groups
(136).
Concomitant administration of the combination MMRV vaccine with other vaccines also has been assessed. In a
clinical trial involving 1,913 healthy children aged 12--15 months, three groups were compared
(137). One group received concomitantly administered (at separate sites) MMRV vaccine, Diphtheria and Tetanus Toxoids and Acellular
Pertussis Vaccine Absorbed (DTaP), Hib conjugate (meningococcal
protein conjugate) vaccine, and hepatitis B (recombinant) (Hep
B) vaccine. The second group received MMRV vaccine at the initial visit, followed by DTaP, Hib, and Hep B
vaccines administered concomitantly 6 weeks later. The third group received MMR and varicella vaccines concomitantly followed
6 weeks later by DTaP, Hib, and Hep B vaccines. Seroconversion rates and antibody titers were comparable for the
measles, mumps, rubella, and varicella components for the first two groups. No immunologic data were reported for
the third group. The Hib and Hep B seroconversion rates for the two groups that received those vaccines also were comparable.
Data are absent or limited for the concomitant use of MMRV vaccine with inactivated polio, pneumococal
conjugate, influenza, and hepatitis A vaccines. Simultaneous administration of the majority of widely used live and inactivated
vaccines has produced seroconversion rates and rates of adverse reactions similar to those observed when the vaccines
are administered separately. Therefore, single-antigen and combination MMRV vaccines may be administered simultaneously
with other vaccines recommended for children aged 12--15 months and those aged 4--6 years. Simultaneous administration
is
particularly important when health-care providers anticipate
that, because of certain factors (e.g., previously
missed vaccination opportunities), a child might not return for subsequent vaccination.
Economic Analysis of Vaccination
A cost-effectiveness analysis was performed before initiation of the varicella vaccination program in the United States
(138). The results of the study indicated a savings of $5.40 for each dollar spent on routine vaccination of preschool-aged
children when direct and indirect costs were considered. When only direct medical costs were considered, the benefit-cost ratio
was 0.9:1.0. Benefit-cost ratios were only slightly lower when lower estimates of the short- and long-term effectiveness of
the vaccine were used.
A recent analysis was performed that used current estimates of morbidity and mortality
(20,28,33) and current direct and indirect costs (ACIP, unpublished presentation, 2006). The model considered that the second dose will reduce varicella
disease residual after the first dose by 79%. From a societal perspective, both 1-dose and 2-dose vaccination programs are cost
saving compared with no program. The vaccine program cost was estimated at $320 million for 1 dose and $538 million for 2
doses. The savings from varicella disease prevented were estimated at approximately $1.3 billion for the 1-dose program
and approximately $1.4 billion for the 2-dose program. Compared with the 1-dose program, the incremental cost for the
second dose was estimated to be $96,000 per quality-adjusted life year (QALY) saved. If benefits from preventing group
A streptococcus infections and HZ among vaccinated persons are added, incremental costs per QALY saved are $91,000
and $17,000, respectively. Because of the uncertainty of the modeled predictions of an increase in HZ among persons with
a history of varicella and the fact that no consistent trends
demonstrate an increase in HZ attributable to the
varicella vaccination program in the United States, HZ among persons with a history of varicella was not included in the model.
Storage, Handling, and Transportation of Varicella Vaccines
Single-antigen varicella and combination MMRV vaccines have similar but not identical distribution, handling, and
storage requirements (79,80). For potency to be maintained, the lyophilized varicella vaccines must be stored frozen at an
average temperature of 5°F (-15°C) or colder. Household freezers manufactured since the mid-1980s are designed to
maintain temperatures from -4°F (-20°C) to 5°F (-15°C). When tested, VARIVAX has remained stable in frost-free freezers.
Freezers that reliably maintain an average temperature of <5°F (<-15°C) and that have a separate sealed freezer door are acceptable
for storing VARIVAX and ProQuad. Health-care providers may use stand-alone freezers or the freezer compartment
of refrigerator-freezer combinations, provided that the freezer compartment has its own separate, sealed, and insulated
exterior door. Units with an internal freezer door are not acceptable. Temperatures should be documented at the beginning and end
of each day. Providers should document the required temperature in a newly purchased unit for a minimum of 1 week
before using it to store vaccine and routinely thereafter. When varicella vaccines are stored in the freezer compartment of a
combined refrigerator-freezer, temperatures in both compartments should be monitored carefully. Setting the thermostat low enough
for storage of varicella-containing vaccines might inadvertently expose refrigerated vaccines to freezing temperatures.
Refrigerators with ice compartments that either are not tightly enclosed or are enclosed with unsealed, uninsulated doors (e.g.,
small, dormitory-style refrigerators) are not acceptable
for the storage of varicella vaccines.
Diluent should be stored separately either at room temperature or in the refrigerator. Vaccines should be
reconstituted according to the directions in the package insert and only with the diluent supplied with the vaccine, which does not
contain preservative or other antiviral substances that could inactivate the vaccine virus. Once reconstituted, vaccine should be
used immediately to minimize loss of potency. Vaccine should be discarded if not used within 30 minutes after reconstitution.
Handling and Transportation of Varicella Vaccines Within Off-Site Clinics
When an immunization session is being held at a site distant from the freezer in which the vaccine is stored, the number
of vaccine vials needed for the immunization session should be packed in either a vaccine shipping container (as received
from the manufacturer) or in an insulated cooler, with an
adequate quantity of dry ice (i.e., a minimum of 6 lbs per box) to
preserve potency. When placed in a suitable container, dry ice will maintain a temperature of
<5°F (<-15°C). Dry ice should remain
in
the container upon arrival at the clinic site. If no dry ice remains when the container is opened at the receiving site,
the manufacturer (Merck and Company, Inc.) should be contacted for guidance (telephone: 1-800-982-7482). If dry ice
is available at the receiving site, it may be used to store vaccine. Thermometers or temperature indicators cannot be used in
a container with dry ice. Diluent should not be transported on dry ice.
If dry ice is not available, only single-antigen varicella vaccine may be transported, with frozen packs to keep
the temperatures between 36°F--46°F (2°C--8°C). Transport temperatures should be monitored, and a temperature indicator
or thermometer should be placed in the container and checked on arrival. The container should be kept closed as much
as possible during the immunization session; temperatures should be checked and recorded hourly. If the temperature
remains between 36°F--46°F (2°C--8°C), the single-antigen varicella vaccine may be used for up to 72 hours after its removal from
the freezer. The date and time should be marked on the vaccine vial. Single-antigen varicella vaccine stored at
refrigerated temperatures for any period of time may not be refrozen for future use.
Transportation and storage of combination MMRV vaccine at temperatures between 36°F--46°F (2°C--8°C) is not
permissible for any length of time. In contrast to single-antigen varicella vaccine, combination MMRV vaccine must be maintained
at temperatures of <5°F
(<-15°C) until the time of reconstitution and administration. This difference in vaccine
storage temperatures must be considered when planning off-site clinics. For this reason, transportation of MMRV vaccine to
off-site clinics is not advised. If any concerns arise regarding the storage of single-antigen varicella or combination MMRV vaccines,
the manufacturer should be contacted for guidance.
Minimizing Wastage of Vaccine
Vaccine wastage can be minimized by accurately determining the number of doses needed for a given patient population.
To ensure maximal vaccine potency, smaller shipments of vaccine should be ordered more frequently (preferably at least
once every 3 months). Single-antigen varicella vaccine should not be distributed to providers who do not have the capacity to
store it properly in a freezer until it is used. Transportation of varicella vaccine should be kept to a minimum to prevent loss
of potency. Off-site clinic sites should receive only such amounts of vaccine as they can use within a short time (72 hours
if storing single-antigen varicella vaccine at refrigerated temperatures).
Adverse Events After Vaccination
Because adverse events after vaccination might continue to be caused by wild-type VZV even as varicella disease
declines, health-care providers should obtain event-appropriate clinical specimens (e.g., cerebrospinal fluid for encephalitis,
bronchial lavage or lung biopsy for pneumonia) for laboratory evaluation, including strain identification. Information regarding
strain identification is available from Merck's VZV Identification Program (telephone: 1-800-652-6372) or from CDC's
National Varicella Reference Laboratory (telephone: 404--639--0066; e-mail: vzvlab@cdc.gov) or at
http://www.cdc.gov/nip/diseases/varicella/surv/default.htm. Commercial
laboratories do not have the capability for strain identification.
The National Vaccine Injury Act of 1986 requires physicians and other health-care providers who administer vaccines
to maintain permanent immunization records and to report occurrences of adverse events for selected vaccines,
including varicella vaccines. Serious adverse events (i.e., all events
requiring medical attention) suspected to have been caused by
varicella vaccines should be reported to the Vaccine
Adverse Event Reporting System (VAERS). Forms and instructions are available
at https://secure.vaers.org/vaersDataEntryintro.htm, in the FDA Drug Bulletin at
http://www.fda.gov/medwatch, or from the 24-hour VAERS information recording at 1-800 822-7967.
Prelicensure
Single-Antigen Varicella Vaccine
Single-antigen varicella vaccine was well-tolerated when
administered to >11,000 healthy children, adolescents, and
adults during prelicensure clinical trials. In a double-blind,
placebo-controlled study among 914 susceptible healthy children aged
12 months--14 years, the only statistically significant (p<0.05) adverse events reported that were more common among
vaccine recipients than among placebo recipients were pain and redness at the injection site
(103). This study also described the presence of
unspecific rash among 2% of placebo and 4% of vaccine
recipients occurring within 43 days of vaccination.
Of
the 28 reported rashes, 10 (36%) were examined by a physician; among those that were examined, four of the
seven noninjection site rashes in vaccine recipients were judged to be varicella-like, compared with none of the rashes in the
placebo recipients.
In a study comparing the safety of 1 dose of single-antigen varicella vaccine with that of 2 doses administered 3
months apart, no serious adverse events related to vaccination were reported among approximately 2,000 healthy subjects aged
12 months--12 years who were followed for 42 days after each injection. The 2-dose vaccine regimen was generally
well-tolerated, and its safety profile was comparable to that of the 1-dose regimen. Incidence of injection site complaints
observed <3 days after vaccination was slightly higher after dose 2 (25.4%) than after dose 1 (21.7%). Incidence of systemic clinical
complaints was lower after dose 2; fever incidence from days 7--21 was 7% after dose 1 and 4% after dose 2 (p = 0.009), and
varicelliform rash incidence after dose 1 was 3%, compared with 1% after dose 2 (p = 0.008), with peak occurrence 8--21 days
after vaccination (139).
In uncontrolled trials of persons aged
>13 years , approximately 1,600 vaccine recipients who received 1 dose of
single-antigen varicella vaccine and 955 who received 2 doses of vaccine were monitored for 42 days for adverse events
(79). After the first and second doses, 24.4% and 32.5% of vaccine recipients, respectively, had complaints regarding the injection
site. Varicella-like rash at the injection site occurred in 3% of vaccine recipients after the first injection and in 1% after the
second. A nonlocalized rash occurred in 5.5% of vaccine recipients after the first injection and in 0.9% of vaccine recipients after
the second, at a peak of 7--21 and 0--23 days postvaccination, respectively.
Combination MMRV Vaccine
In clinical trials, combination MMRV vaccine was administered to 4,497 children aged 12--23 months
without concomitant administration with other vaccines
(80). The safety profile of the first dose was compared with the safety
of MMRII vaccine and VARIVAX administered concomitantly at separate injection sites. The follow-up period was 42
days postvaccination. Systemic vaccine-related adverse events were reported at a statistically significantly greater rate in persons
who received MMRV vaccine than in persons who received the two vaccines administered concomitantly at separate
injection sites: fever (>102°F
[>38.9°C] oral equivalent), (21.5% and 14.9%, respectively), and measles-like rash (3.0% and
2.1%, respectively). Both fever and measles-like rash usually occurred within 5--12 days after the vaccination, were of short
duration, and resolved with no long-term sequelae. Pain, tenderness, and soreness at the injection site were reported at a
statistically significantly lower rate in persons who received the combination MMRV vaccine (22.0%) than in those who received
MMRII and VARIVAX vaccines (26.7%). Rash at the injection site was more frequent among recipients of
1-dose MMRV vaccine (2.3%) than among recipients of the two vaccines administered separately as first doses (1.5%). A study that also
compared use of MMRV with MMRII and VARIVAX administered as a first dose demonstrated similar results
(90). During days 5--12, children in the group that received MMRV had higher rates of elevated temperatures than those in the group that
received MMRII and VARIVAX (27.7% and 18.7%, respectively; p = 0.034).
To demonstrate that MMRV vaccine could be administered as a second dose, a study was conducted involving 799
children aged 4--6 years who had received primary doses of MMRII and VARIVAX vaccines, either concomitantly or not, at age
>12 months and >1 month before study enrollment
(91). These children were vaccinated randomly (with MMRV and
placebo, MMR and placebo, or MMRII and VARIVAX) and then monitored for safety. No serious vaccine-related adverse
experiences were reported. Overall, the proportions of subjects with one or more adverse event were comparable among groups
receiving MMRV, MMRII, and MMRII and VARIVAX. The group receiving MMRV vaccine had a statistically significantly
greater proportion of subjects with erythema (p = 0.01) and swelling (p = 0.008) at the injection site 1--5 days after
vaccination. Another study examined the safety of 2 doses of MMRV administered 3 months apart to 480 children aged 12--23
months (90). The rate of adverse events typically was lower after the second dose of MMRV than after the first dose. The incidence
of varicella-like rashes was lower after a second dose of MMRV than after concomitant administration of MMRII and
VARIVAX vaccines (0.0% and 1.9%, respectively; p = 0.01).
Postlicensure
During March 1, 1995--December 31, 2005, a total of 47.7 million doses of varicella vaccine were distributed in the
United States, and 25,306 adverse events that occurred after varicella vaccine administration were reported to VAERS, 1,276 (5%)
of which were classified as serious. The overall adverse event reporting rate was 52.7 cases per 100,000 doses distributed. The
rate
of reporting of serious adverse events was 2.6 per 100,000 doses distributed. Half of all adverse events reported
occurred among children aged 12--23 months (VAERS,
unpublished data, 2006).
Not all adverse events that occur after vaccination are
reported, and many reports describe events that might have
been caused by confounding or unrelated factors (e.g., medications and other diseases). Because varicella disease continues to
occur, wild-type virus might account for certain reported events. For serious adverse events for which background incidence data
are known, VAERS reporting rates are lower than expected after natural varicella or than background rates of disease in
the community. Inherent limitations of passive safety surveillance impede comparing adverse event rates after vaccination
reported to VAERS with those from complications after natural disease. Nevertheless, the magnitude of these differences suggests
that serious adverse events occur at a substantially
lower rate after vaccination than after natural disease. This assumption
is corroborated by the substantial decline in the number of severe complications, hospitalizations, and deaths related to
varicella that have been reported since implementation of the varicella vaccination program
(22,23,28).
Similar to the prelicensure experience, postlicensure safety surveillance data after administration of single-antigen
varicella vaccine indicated that rash, fever, and injection-site reactions were the most frequently reported adverse events
(140,141). Using these reports from passive surveillance of adverse events during the first 4 years of the vaccination program, when
wild-type VZV was still circulating widely, polymerase chain reaction (PCR) analysis confirmed that the majority of rash
events occurring within 42 days of vaccination were caused primarily by wild-type varicella-zoster virus. Rashes from the
wild-type virus occurred a median of 8 days after vaccination (range: 1--24 days), whereas rashes from the vaccine strain occurred
a median of 21 days after vaccination (range: 5--42 days)
(140).
As part of postmarketing evaluation of the short-term safety of VARIVAX, 89,753 vaccinated adults and children
were identified from automated clinical databases of hospitals, emergency room visits, and clinic visits during April
1995--December 1996 (56). Out of all potential adverse events identified, no consistent time association or clustering of any
events was noted during the exposure follow-up period. No cases of ataxia or encephalitis were identified after receipt of
varicella vaccine in this group of vaccine recipients. In the prevaccine era, among children aged <15 years, acute cerebellar ataxia
was estimated to occur at a rate of one in 4,000 varicella cases, and varicella encephalitis without ataxia was estimated to
occur at one in 33,000 varicella cases (142).
Severe complications that are laboratory-confirmed to be caused by vaccine virus strain are rare and include
pneumonia (140), hepatitis (143), severe disseminated varicella infection
(140,141,144,145), and secondary transmission from
five vaccine recipients (140,146--148). Except for the secondary transmission cases, these cases all occurred
in immunocompromised patients or in persons who had other serious medical conditions that were undiagnosed at the time
of vaccination.
Although other serious adverse events have been reported, vaccine strain involvement was not
laboratory-confirmed. Thrombocytopenia
(140,141,149) and acute cerebellar ataxia
(140,141,150) have been described as potentially
associated with single-antigen varicella vaccine. Two children had acute hemiparesis diagnosed after varicella vaccination (one at 5
days and the other at 3 weeks) (151). In both cases, unilateral
infarction of the basal ganglia and internal capsule was noted;
this distribution is consistent with varicella angiopathy. Urticaria after varicella vaccine has been associated with gelatin
allergy (152). Recurrent papular urticaria has been reported to be potentially associated with varicella vaccination
(153). However, available data regarding the potential adverse events after
varicella vaccination are insufficient to determine a
causal association. The quality of reported information varies widely, and simultaneous administration with other
vaccines (especially MMR) might confound attribution.
Herpes Zoster. Similar to wild-type VZV, vaccine virus can establish latent infection and subsequently reactivate, causing
HZ disease in vaccine recipients. Before vaccine licensure, studies in children with leukemia had demonstrated a much lower rate
of HZ in vaccinated children compared with those (age and protocol matched) with previous varicella
(54). Cases of HZ in healthy vaccine recipients have been confirmed to be caused by both vaccine virus and wild-type virus, suggesting that certain HZ cases
in vaccine recipients might result from antecedent natural
varicella infection that might not have been detected by the
patient or from infection after vaccination
(140). A single case has been reported of a child who received a diagnosis of
neuroblastoma and had severe chronic zoster attributed to vaccine virus strain that with time became drug resistant
(145). A large postlicensure safety study performed through surveys conducted every 6 months and validated by medical chart review in the first 9 years of a
15-year follow-up study of >7,000 enrolled children vaccinated with
single-antigen varicella vaccine at age 12--24 months estimated
HZ disease incidence to be 22 per 100,000 person-years (CI = 13--37) as reported by parents (Steven Black, MD,
Northern
California Kaiser Permanente Medical Care Program, unpublished presentation, 2005). The incidence of HZ was 30 per
100,000 person-years among healthy children aged 5--9 years
(154) and 46 per 100,000 person-years for those aged
<14 years (64). However, these rates are drawn from different populations and based on different methodologies. In addition, a proportion
of children in these age groups would not have experienced varicella disease; those rates are likely to underestimate rates in a
cohort of children all infected with wild-type VZV, making direct comparison
difficult with a vaccinated cohort.
Transmission of Vaccine Virus
Results from prelicensure vaccine trials of the
single-antigen varicella vaccine suggest that transmission of varicella
vaccine virus from healthy persons to susceptible contacts is rare. This risk was assessed in siblings of healthy vaccinated children
who themselves received placebo (103). Six (1%) of 439 placebo recipients seroconverted without rash; the vaccinated siblings
of these six children also did not develop rash. Serologic data suggested that three of these six seroconverters received
vaccine mistakenly in lieu of their siblings. In a smaller study, immunocompromised siblings of healthy children
receiving varicella vaccine were evaluated clinically and by testing for humoral or cell-mediated immune responses
(155). No evidence was demonstrated of vaccine virus transmission to any of 30 immunocompromised
siblings from 37 healthy children receiving varicella vaccine.
Accumulated data from postlicensure surveillance activities suggest that the risk for transmission of varicella vaccine
virus from healthy persons to susceptible contacts is low. With >55 million doses of VARIVAX distributed since
licensure, transmission from immunocompetent persons after vaccination has been documented by PCR analysis from only five
persons, resulting in six secondary infections, all of them mild
(140,146--148). Three episodes involved transmission from
healthy children aged 1 year to healthy household contacts, including a sibling aged 4 months, a father, and a pregnant mother. In
the latter episode, the mother chose to terminate the pregnancy, but fetal tissue tested subsequently by PCR was negative
for varicella vaccine virus (147). The children in these episodes had 2, 12, and 30 lesions, respectively. A fourth episode
involved transmission from an immunocompetent adolescent who was a resident in an institution for chronically disabled children.
The adolescent had >500 lesions after vaccination, and vaccine virus was transmitted to another immunocompetent resident of
the institution and to a health-care worker, both of whom had histories of varicella
(146). The fifth episode represented a
tertiary spread from a healthy sibling contact of a vaccinee with leukemia
(148). Rashes for both healthy siblings were mild (i.e.,
40 and 11 lesions, respectively), and vaccine virus was isolated from all three case-patients. The third sibling had rash 18
days after the onset of the secondary case-patient and 33 days after rash onset in the vaccinated leukemic child. In addition to
these five episodes, one child has been reported to have transmitted vaccine virus from HZ that occurred 5 months after
varicella vaccination; 2 weeks later, a mild varicella-like rash from which vaccine varicella virus was isolated occurred in the
child's vaccinated brother (156).
Although varicella vaccine is not recommended for children with cellular immune deficiencies, the experience
from prelicensure vaccine trials involving children with leukemia is instructive. Data from a study of varicella vaccination
in children with leukemia indicated that varicella virus vaccine transmission occurred in 15 (17%) of 88 healthy,
susceptible siblings of leukemic vaccine recipients; the rash was mild in 11 (73%) of the 15 infected siblings
(148). The risk for transmission was correlated with the number of skin lesions in the immunocompromised vaccine recipients.
These data suggest that healthy, vaccinated persons have a minimal risk for transmitting vaccine virus to their
contacts, particularly in the absence of vaccine rash in the vaccine
recipient. Vaccine recipients who have a vaccine-related
rash, particularly HCP and household contacts of immunocompromised persons, should avoid contact with persons
without evidence of immunity who are at high risk for severe complications (see Health-Care Personnel)
Summary of Rationale for Varicella Vaccination
Varicella vaccine is an effective prevention tool for decreasing the burden attributable to varicella disease and
its complications in the United States. In the prevaccine era, varicella was a childhood disease with >90% of the 4 million
cases, two thirds of approximately 11,000 hospitalizations, and
approximately half of 100--150 annual deaths occurring
among persons aged <20 years. Single-antigen varicella vaccine is
licensed for use among healthy persons aged
>12 months, and the combination MMRV vaccine is licensed for use in healthy children aged 12 months--12 years. Prelicensure and
postlicensure
studies have demonstrated that 1 dose of single-antigen varicella vaccine is approximately 85% effective in preventing
varicella. Breakthrough varicella disease that occurs
after vaccination frequently is mild and modified.
Varicella vaccine is >95% effective in preventing severe varicella disease. Since implementation of the varicella vaccination program in 1995, varicella
incidence, hospitalizations, and deaths have declined substantially. MMRV was licensed on the basis of immunological noninferiority
to its vaccine antigenic components. Initial varicella vaccine policy recommendations were for 1 dose of varicella vaccine
for children aged 12 months--12 years and 2 doses, 4--8 weeks apart, for persons aged
>13 years. In June 2006, ACIP approved a routine 2-dose recommendation for children. The first dose should be administered at age 12--15 months and the second
dose at age 4--6 years.
The rationale for the second dose of varicella vaccine for children is to further decrease varicella disease and its
complications in the United States. Despite the successes of the
1-dose vaccination program in children, vaccine effectiveness of 85% has
not been sufficient to prevent varicella outbreaks, which, although less than in the prevaccine era, have continued to occur
in highly vaccinated school populations. Breakthrough varicella is contagious. Studies of the immune response after 1 and
2 doses of varicella vaccine demonstrate a greater-than-tenfold boost in GMTs when measured 6 weeks after the second
varicella vaccine dose. A higher proportion (>99%) of children achieve an antibody response of
>5 gpELISA units after the second dose compared with 76%--85% of children after a single dose of varicella vaccine. The second dose of varicella vaccine is
expected to provide improved protection to the 15%--20% of children who do not respond adequately to the first dose. Data from
a randomized clinical trial conducted postlicensure indicated that vaccine efficacy after
2 doses of single-antigen varicella vaccine in children (98.3%; CI = 97.3%--99.0%) was significantly higher than that after a single dose (94.4%; CI
=92.9%--95.7%). The risk for breakthrough disease was 3.3-fold lower among children who
received 2 doses than it was among children who received
1 dose. How this increase in vaccine efficacy (typically higher than observed under field conditions) will translate
into vaccine effectiveness under conditions of community use will be an important area of study.
The recommended ages for routine first (at age 12--15 months) and second (at age 4--6 years) doses of varicella vaccine
are harmonized with the recommendations for MMR vaccine use and intended to limit the period when children have
no varicella antibody. The recommended age for the
second dose is supported by the current epidemiology of
varicella, with low incidence and few outbreaks among preschool-aged children and higher incidence and more outbreaks among
elementary-school--aged children. However, the second dose may be administered at an earlier age, provided that the interval between
the first and second doses is 3 months. The recommendation for the minimum interval between doses is made on the basis of
the design of the studies evaluating 2 doses among children aged 12 months--12 years. MMRV vaccine may be used to
vaccinate children against measles, mumps, rubella, and varicella simultaneously. Because the risk for transmission can be high
among students in schools, colleges, and other postsecondary educational institutions, students without evidence of immunity
should receive 2 doses of varicella vaccine. All children and adolescents who received
1 dose of varicella vaccine previously should receive a second dose.
Varicella disease is more severe and its complications more frequent among adolescents and adults. The recommendation
for vaccination of all adolescents and adults without
evidence of immunity will provide protection in these age groups.
Because varicella might be more severe in immunocompromised persons who might not be eligible for vaccination, and because of
the risk of VZV transmission in health-care settings, HCP must be vaccinated. Varicella
disease during the first two trimesters of pregnancy might
infect the fetus and result in congenital varicella syndrome. Therefore, routine antenatal screening
for evidence of immunity and postpartum vaccination for those without evidence of immunity now is recommended.
Recommendations for the Use of Varicella Vaccines
Two 0.5-mL doses of varicella vaccine administered subcutaneously are recommended for children aged
>12 months, adolescents, and adults without evidence of immunity. For children aged 12 months--12 years, the recommended
minimum interval between the two doses is 3 months. However, if the second dose was administered
>28 days after the first dose, the second dose is considered valid and need not be
repeated. For persons aged >13 years, the recommended minimum
interval is 4 weeks. Single-antigen varicella vaccine is approved for use among healthy persons aged
>12 months. Combination MMRV vaccine is approved for use among healthy children aged 12 months--12 years. MMRV vaccine is indicated for
simultaneous vaccination against measles, mumps, rubella, and varicella. Whenever any components of the combination vaccine
are
indicated and the other components are not
contraindicated, use of licensed combination vaccines, such as MMRV vaccine,
is preferred over separate injection of equivalent component vaccines
(157).
Routine Vaccination
Persons Aged 12 Months--12 Years
Preschool-Aged Children
All healthy children should receive their first dose of varicella-containing vaccine routinely at age 12--15 months.
School-Aged Children
A second dose of varicella vaccine is recommended routinely for all children aged 4--6 years (i.e., before
entering prekindergarten, kindergarten, or first grade). However, it may be administered at an earlier age provided that the
interval between the first and second dose is >3 months.
Because of the risk for transmission of VZV in schools, all children entering school should have received 2 doses of
varicella-containing vaccine or have other evidence of immunity to varicella (see Evidence of Immunity).
Persons Aged >13 Years
Persons aged >13 years without evidence of varicella immunity should receive two 0.5-mL doses of single-antigen
varicella vaccine administered subcutaneously, 4--8 weeks apart. If >8 weeks elapse after the first dose, the second dose may
be administered without restarting the schedule. Only single-antigen varicella vaccine may be used for vaccination of persons
in this age group. MMRV is not licensed for use among persons aged
>13 years.
School-Aged Children, College Students, and Students in Other Postsecondary Educational Institutions
All students should be assessed for varicella immunity, and those without evidence of immunity should routinely receive
2 doses of single-antigen varicella vaccine 4--8 weeks apart. The risk for transmission of varicella among school-aged
children, college students, and students in other postsecondary educational institutions can be high because of high contact rates.
Other Adults
All healthy adults should be assessed for varicella immunity, and those who do not have evidence of immunity
should receive 2 doses of single-antigen varicella vaccine 4--8 weeks apart. Adults who might be at increased risk for exposure
or transmission and who do not have evidence of immunity should receive special consideration for vaccination,
including 1) HCP, 2) household contacts of immunocompromised persons, 3) persons who live or work in environments in
which transmission of VZV is likely (e.g., teachers, day-care employees, residents and staff in institutional settings), 4) persons
who live or work in environments in which transmission has been reported (e.g., college students, inmates and staff members
of correctional institutions, and military personnel), 5) nonpregnant women of childbearing age, 6) adolescents and adults
living in households with children, and 7) international travelers.
Second Dose Catch-Up Vaccination
To improve individual protection against varicella and to have a more rapid impact on school outbreaks, second dose
catch-up varicella vaccination is recommended for children, adolescents, and adults who previously
received 1 dose. The recommended minimum interval between the first dose and the catch-up second dose is 3 months for children aged
<12 years and 4 weeks for persons aged
>13 years. However, the catch-up second dose may be administered at any interval longer
than the minimum recommended interval. Catch-up vaccination may be implemented during routine health-care provider
visits and through school- and college-entry requirements.
As part of comprehensive health services for all adolescents, ACIP, AAP, and AAFP recommend a health maintenance visit
at age 11--12 years. This visit also should serve as an immunization visit to evaluate vaccination status and administer
necessary vaccinations (158). Physicians should use this and other routine visits to ensure that all children without evidence of
varicella immunity have received 2 doses of varicella vaccine.
Requirements for Entry to Child Care, School, College, and Other
Postsecondary Educational Institutions
Child care and school entry requirements for varicella
immunity have been recommended previously
(2). In 2005, ACIP recommended expanding the requirements to cover students in all grade levels. Official health agencies should take
necessary steps, including developing and enforcing school immunization requirements, to ensure that students at all grade
levels (including college) and children in child care centers are protected against varicella and other vaccine-preventable
diseases (157).
Prenatal Assessment and Postpartum Vaccination
Prenatal assessment of women for evidence of varicella
immunity is recommended. Birth before 1980 is not
considered evidence of immunity for pregnant women because of potential severe consequences of varicella infection during
pregnancy, including infection of the fetus. Upon completion or termination of their pregnancies, women who do not have evidence
of varicella immunity should receive the first dose of vaccine before discharge from the health-care
facility. The second dose should be administered 4--8 weeks later, which
coincides with the postpartum visit (6--8 weeks after delivery). For
women who gave birth, the second dose should be administered
at the postpartum visit. Women should be counseled to
avoid conception for 1 month after each dose of varicella vaccine. Health-care settings in which completion or termination
of pregnancy occurs should use standing orders to ensure the administration of varicella vaccine to women
without evidence of immunity.
Special Considerations for Vaccination
Vaccination of HIV-Infected Persons
HIV-infected children with CD4+ T-lymphocyte percentage >15% should be considered for vaccination with the
single-antigen varicella vaccine. Varicella vaccine was recommended previously for HIV-infected children in CDC clinical
and immunologic categories N1 and A1 with age-specific CD4+ T-lymphocyte percentage
>25% (2). Limited data from a
clinical trial in which 2 doses of single-antigen varicella vaccine were administered 3 months apart to 37 HIV-infected children
(CDC clinical categories N, A, or B and immunologic category 2 [CD4+ T-lymphocyte percentage
>15%--24%]) aged 1--8 years indicated that the vaccine was well-tolerated and that >80% of subjects had detectable VZV specific
immune response (either antibody or cell immune response or both) at 1 year after immunization
(159). These children were no less likely to have
an antibody response to the varicella vaccine than were subjects who were less affected immunologically by HIV
infection. Because children infected with HIV are at increased risk for morbidity from varicella and HZ (i.e., shingles) compared
with healthy children, ACIP recommends that, after weighing potential risks and benefits, single-antigen varicella vaccine should
be considered for HIV-infected children with CD4+ T-lymphocyte percentages
>15%. Eligible children should receive 2 doses
of single-antigen varicella vaccine 3 months apart. Because persons with impaired cellular immunity are potentially at greater
risk for complications after vaccination with a live vaccine, these vaccine
recipients should be encouraged to return for evaluation
if they experience a postvaccination varicella-like rash. Data are not available regarding safety, immunogenicity, or efficacy
of MMRV vaccine in HIV-infected children, MMRV vaccine should not be administered as a substitute for the
single-antigen varicella vaccine when vaccinating these children. The titer of Oka/Merck VZV is higher in combination
MMRV vaccine than in single-antigen varicella vaccine. Recommendations for vaccination of HIV-infected children with
measles, mumps, or rubella vaccines have been published previously
(160).
Data on use of varicella vaccine in HIV-infected adolescents and adults are lacking. However, on the basis of expert
opinion, the safety of varicella vaccine in HIV-infected persons aged >8 years with comparable levels of immune function
(CD4+T-lymphocyte count >200
cells/µL) is likely to be similar to that of children aged <8 years. Immunogenicity might be lower
in older HIV-infected children, adolescents, and adults compared to children aged 1--8 years. However, weighing the risk
for severe disease from wild VZV and potential benefit of vaccination, vaccination may be considered (2 doses, administered
3
months apart) for HIV-infected persons with CD4+T-lymphocytes count
>200 cells/µL in these age groups. If vaccination
of HIV-infected persons results in clinical disease, the use of acyclovir might modify the severity of disease.
Situations in Which Some Degree of Immunodeficiency Might be Present
Persons with impaired humoral immunity may be vaccinated. No data have been published concerning whether
persons without evidence of immunity receiving only inhaled, nasal, or topical doses of steroids can be vaccinated safely.
However, clinical experience suggests that vaccination is well-tolerated among these persons. Persons without evidence of immunity
who are receiving systemic steroids for certain conditions (e.g., asthma) and who are not otherwise immunocompromised may
be vaccinated if they are receiving <2 mg/kg of body weight or a total of <20 mg/day of prednisone or its equivalent.
Certain experts suggest withholding steroids for 2--3 weeks after vaccination if it can be done safely
(1). Data from a Japanese study using the Oka/Biken varicella vaccine (which is not available in the United States but whose immunogenicity and efficacy
are similar to those of the varicella vaccine used in the United States) indicated that children taking steroids for nephrosis
were vaccinated safely when the steroids were suspended for 1--2 weeks before vaccination, although no
serious reactions occurred among children vaccinated when steroid therapy was not suspended
(161). Persons who are receiving high doses of
systemic steroids (i.e., >2 mg/kg prednisone) for
>2 weeks may be vaccinated once steroid therapy has been discontinued for
>1 month, in accordance with the general recommendations for the use of live-virus vaccines
(157).
Vaccination of leukemic children who are in remission and who do not have evidence of immunity to varicella should
be undertaken only with expert guidance and with the availability of antiviral therapy should complications ensue. Patients
with leukemia, lymphoma, or other malignancies whose disease is in remission and whose chemotherapy has been terminated for
at least 3 months can receive live-virus vaccines
(157). When immunizing persons in whom some degree of
immunodeficiency might be present, only single-antigen varicella vaccine should be used.
Vaccination of Household Contacts of Immunocompromised Persons
Immunocompromised persons are at high risk for serious varicella infections. Severe disease occurs in approximately 30%
of such persons with primary infection. Because varicella vaccine now is recommended for all healthy children and
adults without evidence of immunity, household contacts of immunocompromised persons should be vaccinated routinely.
Although the risk for exposure to wild VZV for immunocompromised persons now is lower than it was previously, vaccine should
be offered to child and adult household contacts without evidence of immunity of immunocompromised persons. Vaccination
of household contacts provides protection for immunocompromised persons by decreasing the likelihood that wild-type
VZV will be introduced into the household. Vaccination of household contacts of immunocompromised persons
theoretically might pose a minimal risk for transmission of vaccine virus to immunocompromised persons, although in one study,
no evidence of transmission of vaccine virus was demonstrated after vaccination of 37 healthy siblings of 30 children
with malignancy (155). No cases have been documented of transmission of vaccine virus to immunocompromised persons in
the postlicensure period in the United States, with >55 million doses of vaccine distributed. Other data indicate that
disease caused by vaccine virus in immunocompromised persons is milder than wild-type disease and can be treated with
acyclovir (148,159). The benefits of vaccinating susceptible household contacts of immunocompromised persons outweigh
the extremely low potential risk for transmission of vaccine virus to immunocompromised contacts. Vaccine recipients in
whom vaccine-related rash occurs, particularly HCP and household contacts of immunocompromised persons, should avoid
contact with susceptible persons who are at high risk for severe complications. If a susceptible, immunocompromised person
is inadvertently exposed to a person who has a vaccine-related rash, postexposure prophylaxis with VZIG is not
needed because disease associated with this type of virus is expected to be mild.
Nursing Mothers
Postpartum vaccination of women without evidence of immunity need not be delayed because of breastfeeding.
Women who have received varicella vaccination postpartum may continue to breastfeed. The majority of live vaccines are
not associated with virus secretion in breast milk
(157). A study involving 12 women who received single-antigen varicella
vaccine while breastfeeding indicated no evidence of VZV DNA either in 217 breast milk samples collected or in infants tested
after both vaccine doses (162). No infants seroconverted. Another study did not detect varicella gene sequences in
the
postvaccination breast milk samples (163). Therefore, single-antigen varicella vaccine should be administered to
nursing mothers without evidence of immunity. Combination MMRV vaccine is not licensed for use among persons aged
>13 years.
Health-Care Personnel
Nosocomial transmission of VZV is well-recognized
(131,164--173), and guidelines for the prevention of nosocomial
VZV infection and for infection control in HCP have been published
(174,175). Sources of nosocomial exposure have
included patients, hospital staff, and visitors (e.g., the children of hospital employees) who are infected with varicella or HZ.
In hospitals, airborne transmission of VZV has been demonstrated when varicella has occurred in susceptible persons who had
no direct contact with the index case-patient
(176--180).
To prevent disease and nosocomial spread of VZV, health-care institutions should ensure that all HCP have evidence
of immunity to varicella. Birth before 1980 is not considered evidence of immunity for HCP because of the possibility
of nosocomial transmission to high-risk patients. In health-care institutions, serologic screening before vaccination of
personnel who have a negative or uncertain history of varicella and who are unvaccinated is likely to be cost effective. Institutions
may elect to test all HCP regardless of disease history because a small proportion of persons with a positive history of
disease might be susceptible.
Routine testing for varicella immunity after 2 doses of vaccine is not recommended for the management of vaccinated
HCP. Available commercial assays are not sensitive enough to detect antibody after vaccination in all instances. Sensitive tests
have indicated that 99% of adults develop antibodies after the second dose. However, seroconversion does not always result in
full protection against disease, and no data regarding correlates of protection are available for adults.
HCP who have received 2 doses of vaccine and who are exposed to VZV should be monitored daily during days 10--21
after exposure through the employee health program or by an infection control nurse to determine clinical status (i.e., daily
screen for fever, skin lesions, and systemic symptoms). Persons with varicella might be infectious up to 2 days before rash onset.
In addition, HCP should be instructed to report fever, headache, or other constitutional symptoms and any atypical skin
lesions immediately. HCP should be placed on sick leave immediately if symptoms occur. Health-care institutions should
establish protocols and recommendations for screening and vaccinating HCP and for management of HCP after exposures in the
work place.
HCP who have received 1 dose of vaccine and who are
exposed to VZV should receive the second dose with
single-antigen varicella vaccine within 3--5 days after exposure to rash (provided 4 weeks have elapsed after the first dose). After
vaccination, management is similar to that of 2-dose vaccine recipients.
Unvaccinated HCP who have no other evidence of immunity who are exposed to VZV are potentially infective from
days 10--21 after exposure and should be furloughed during this period. They should receive postexposure vaccination as soon
as possible. Vaccination within 3--5 days of exposure to rash might modify the disease if infection occurred. Vaccination >5
days postexposure still is indicated because it induces protection against subsequent exposures (if the current
exposure did not cause infection).
The risk for transmission of vaccine virus from vaccine
recipients in whom varicella-like rash occurs after vaccination is
low and has been documented after exposures in households and long-term care facilities
(140,146--148). No cases have been documented after vaccination of HCP. The benefits of vaccinating HCP without evidence of immunity outweigh
this extremely low potential risk. As a safeguard, institutions should consider precautions for personnel in whom rash occurs
after vaccination. HCP in whom a vaccine-related rash occurs should avoid contact with persons without
evidence of immunity who are at risk for severe disease and complications until all lesions resolve (i.e., are crusted over or fade away) or no
new lesions appear within a 24-hour period.
Varicella IgG Antibody Testing
The tests most widely used to detect varicella IgG antibody after natural varicella infection among HCP are
latex agglutination (LA) and ELISA. A commercially available LA test using latex particles coated with VZV glycoprotein
antigens can be completed in 15 minutes and does not require special equipment
(181). The sensitivity and specificity of the LA
test are comparable to those of FAMA in detecting antibody response after natural varicella infection. The LA test generally
is more sensitive than commercial ELISAs. The LA test has detected antibody for up to 11 years after varicella vaccination
(182).
However, for the purpose of screening HCP for varicella susceptibility, a less sensitive and more specific commercial
ELISA should be considered. A recent report indicated that the LA test can
produce false-positive results, particularly when only
a single concentration of serum is evaluated
(183); this led to documented cases of false-positive results in HCP
who consequently remained unvaccinated and subsequently contracted varicella.
Vaccination for Outbreak Control
Varicella vaccination is recommended for outbreak control. Persons who do not have adequate evidence of immunity
should receive their first or second dose as appropriate. Additionally, in outbreaks among preschool-aged children, 2-dose vaccination
is recommended for optimal protection, and children vaccinated with 1 dose should receive their second dose provided
3 months have elapsed since the first dose. State and local health departments may advise exposed persons who do not have evidence
of immunity to contact their health-care providers for vaccination, or they may offer vaccination through the health department
or school (or other institutions) vaccination clinics. Although outbreak control efforts optimally should be implemented as soon
as an outbreak is identified, vaccination should be offered even if the outbreak is identified late. Varicella outbreaks in
certain settings (e.g., child care facilities, schools, or institutions) can last as long as 4--5 months. Thus, offering vaccine during
an outbreak might provide protection to persons not yet exposed and shorten the duration of the outbreak
(184). Persons receiving either their first or second dose as part of the outbreak control program may be readmitted to school
immediately. Those vaccinated with the first dose as part of outbreak control measures should be scheduled for the second dose as
age appropriate. Persons who are unvaccinated and without other evidence of immunity who do not receive vaccine should
be excluded from institutions in which the outbreak is occurring until 21 days after the onset of rash in the last case of varicella.
In addition, for school-aged persons covered by the 2-dose school vaccination requirements, exclusion during an outbreak
is recommended for those vaccine recipients who had
received the first dose before the outbreak but not the second as part of
the oubtreak control program. Persons at increased risk for severe varicella who have contraindications to vaccination
should receive VZIG within 96 hours of exposure.
Contraindications
General
Adequate treatment provisions for anaphylactic reactions, including epinephrine injection (1:1000), should be available
for immediate use should an anaphylactic reaction occur.
Before administering a vaccine, health-care providers should obtain
the vaccine recipient's vaccination history and determine whether the individual had any previous reactions to any
vaccine including Varivax, ProQuad or any measles, mumps, or rubella containing vaccines.
Allergy to Vaccine Components
The administration of live varicella-containing vaccines rarely results in hypersensitivity. The information in the
package insert should be reviewed carefully before vaccine is
administered. Vaccination is contraindicated for persons who have
a history of anaphylactic reaction to any component of the vaccine, including gelatin. Single-antigen varicella vaccine does
not contain preservatives or egg protein; these substances have caused hypersensitive reactions to other vaccines. For
the combination MMRV vaccine, live measles and live mumps vaccines are produced in chick embryo culture. However,
among persons who are allergic to eggs, the risk for serious allergic reactions after administration of measles- or
mumps-containing vaccines is low. Because skin testing with vaccine is not predictive of allergic reaction to vaccination, skin testing is
not required before administering combination MMRV vaccine to persons who are allergic to eggs
(160). The majority of anaphylactic reactions to measles- and
mumps-containing vaccines are associated not with hypersensitivity to egg antigens
but with other vaccine components. Neither single-antigen varicella nor combination MMRV vaccines should be administered
to persons who have a history of anaphylactic reaction to neomycin. However, neomycin allergy usually is manifested as a
contact dermatitis, which is a delayed-type immune response rather than anaphylaxis. For persons who experience such a response,
the adverse reaction, if any, would appear as an erythematous, pruritic nodule or papule present 48--96 hours after vaccination.
A history of contact dermatitis to neomycin is not a contraindication to receiving varicella vaccines.
Altered Immunity
Single-antigen varicella and combination MMRV vaccines are not licensed for use in persons who have any
malignant condition, including blood dyscrasias, leukemia, lymphomas of any type, or other malignant neoplasms affecting the
bone marrow or lymphatic systems. Combination MMRV vaccine should not be administered to persons with primary or
acquired immunodeficiency, including immunosuppression associated with AIDS or other clinical manifestations of HIV
infections, cellular immunodeficiencies, hypogammaglobulinemia, and dysgammaglobulinemia. Combination MMRV vaccine should
not be administered as a substitute for the component vaccines when vaccinating HIV-infected children.
Varicella vaccines should not be administered to persons who have a family history of congenital or
hereditary immunodeficiency in first-degree relatives (e.g., parents and siblings) unless the immune competence of the potential
vaccine recipient has been clinically substantiated or verified by a
laboratory.
Varicella vaccines should not be administered to persons receiving high-dose systemic immunosuppressive
therapy, including persons on oral steroids
>2 mg/kg of body weight or a total of
>20 mg/day of prednisone or equivalent for
persons who weigh >10 kg, when administered for
>2 weeks. Such persons are more susceptible to infections than healthy
persons. Administration of varicella vaccines can result in a more extensive vaccine-associated rash or disseminated disease in
persons receiving immunosuppressive doses of corticosteroids
(185). This contraindication does not apply
to persons who are receiving inhaled, nasal, or topical corticosteroids or low-dose corticosteroids as are used
commonly for asthma prophylaxis or for
corticosteroid-replacement therapy (see Situations in Which Some Degree of Immunodeficiency Might Be Present).
Pregnancy
Because the effects of the varicella virus vaccine on the fetus are unknown, pregnant women should not be
vaccinated. Nonpregnant women who are vaccinated should avoid
becoming pregnant for 1 month after each injection. For
persons without evidence of immunity, having a pregnant household member is not a contraindication to vaccination.
If a pregnant woman is vaccinated or becomes pregnant within 1 month of vaccination, she should be counseled
about potential effects on the fetus. Wild-type varicella poses a low risk to the fetus (see Prenatal and Perinatal
Exposure). Because the virulence of the attenuated virus used in the vaccine is less than that of the wild-type virus, the risk to the fetus,
if any, should be even lower. In 1995, Merck and Co., Inc., in collaboration with CDC, established the VARIVAX
Pregnancy Registry to monitor the maternal-fetal outcomes of pregnant women who were inadvertently administered
varicella vaccine 3 months before or at any time during pregnancy (to report, call: 1-800-986-8999)
(186). During the first 10 years of the pregnancy registry no cases of congenital varicella syndrome or birth defects compatible with congenital varicella
syndrome have been documented (187,188). Among 131 live-born infants of prospectively reported seronegative women (82 of
whom were born to mothers vaccinated during the highest risk period [i.e., the first or second trimester of pregnancy]), no
birth defects consistent with congenital varicella syndrome have been documented (prevalence
rate = 0; CI = 0--6.7%), and three major birth defects were reported (prevalence rate = 2.3%; CI = 0.5%--6.7%). The rate of occurrence of major birth
defects from prospective reports in the registry was similar to the rate reported in the general U.S. population (3.2%), and the
defects indicated no specific pattern or target organ. Although the study results do not exclude the possibility of risk for women
who received inadvertent varicella vaccination before or during pregnancy, the potential risk, if any, is low.
Precautions
Illness
Vaccination of persons who have acute severe illness,
including untreated, active tuberculosis, should be postponed
until recovery. The decision to delay vaccination depends on the severity of symptoms and on the etiology of the disease. No
data are available regarding whether either single-antigen varicella or combination MMRV vaccines exacerbate tuberculosis.
Live attenuated measles, mumps, and rubella virus vaccines administered individually might result in a temporary depression
of tuberculin skin sensitivity. Therefore, if a tuberculin test is to be performed, it should be administered either any time
before, simultaneously with, or at least 4--6 weeks after combination MMRV vaccine. However, tuberculin skin testing is not
a prerequisite for vaccination with single-antigen varicella or combination MMRV vaccines.
Varicella vaccines may be administered to children without evidence of immunity who have mild illnesses, with or
without low-grade fever (e.g., diarrhea or upper-respiratory infection)
(189). Physicians should be alert to the
vaccine-associated temperature elevations that might occur predominantly in the second week after vaccination, especially with
combination MMRV vaccine. Studies suggest that failure to vaccinate children with minor illnesses can impede
vaccination efforts (190).
Thrombocytopenia
Thrombocytopenia is not a contraindication for
single-antigen varicella vaccine. No clinical data are available regarding
the development or worsening of thrombocytopenia in persons vaccinated with combination MMRV vaccine. Cases
of thrombocytopenia have been reported after MMR vaccine and after varicella vaccination. Postmarketing experience with
live MMR vaccine indicates that persons with thrombocytopenia might develop more severe thrombocytopenia after
vaccination. For vaccination of thrombocytopenic children with combination MMRV vaccine, health-care providers should refer to
the ACIP recommendations on MMR vaccination
(160).
Recent Administration of Blood, Plasma, or Immune Globulin
Although passively acquired antibody is known to interfere with response to measles and rubella vaccines
(191), the effect of the administration of immune globulin (IG) on the
response to varicella virus vaccine is unknown. The duration
of interference with the response to measles vaccination is dose-related and ranges from 3--11 months. Because of the
potential inhibition of the response to varicella vaccination by passively transferred antibodies, varicella vaccines should not
be administered for the same intervals as measles vaccine (3--11 months, depending on the dosage) after
administration of blood (except washed red blood cells), plasma, or IG. Suggested intervals between administration of antibody-containing
products for different indications and varicella vaccine have been published previously
(157). In addition, persons who received a varicella vaccine should not be administered an antibody-containing product for 2 weeks after vaccination unless the
benefits exceed those of vaccination. In such cases, the vaccine recipient should either be
revaccinated or tested for immunity at the appropriate intervals, depending on the dose received, and then revaccinated if seronegative.
Use of Salicylates
No adverse events associated with the use of salicylates after varicella vaccination have been reported; however, the
vaccine manufacturer recommends that vaccine recipients avoid
using salicylates for 6 weeks after receiving varicella vaccines
because of the association between aspirin use and Reye syndrome after varicella. Vaccination with subsequent close monitoring
should be considered for children who have rheumatoid arthritis or other conditions requiring therapeutic aspirin. The risk for
serious complications associated with aspirin is likely to be greater in children in whom natural varicella develops than it is in
children who receive the vaccine containing attenuated
VZV. No association has been documented between Reye syndrome
and analgesics or antipyretics that do not contain salicylic acid.
Postexposure Prophylaxis
Healthy Persons
Prelicensure data from the United States and Japan on varicella exposures in children from household, hospital,
and community settings indicate that single-antigen varicella vaccine is effective in preventing illness or modifying varicella
severity if administered to unvaccinated children within 3 days, and possibly up to 5 days, of exposure to rash
(78,101,192). Vaccination within 3 days of exposure to rash was
>90% effective in preventing varicella whereas vaccination within 5 days
of exposure to rash was approximately 70% effective in preventing varicella and 100% effective in modifying severe
disease (101,192). Limited postlicensure studies also have demonstrated that varicella vaccine is highly effective in either preventing
or modifying disease if administered within 3 days of exposure
(193,194). Varicella vaccine is recommended for
postexposure administration for unvaccinated persons without other evidence of immunity. If exposure to VZV does not cause
infection, postexposure vaccination should induce protection against subsequent exposures. If the exposure results in infection,
no
evidence indicates that administration of single-antigen varicella vaccine during the presymptomatic or prodromal stage
of illness increases the risk for vaccine-associated
adverse events. No data are available regarding the potential benefit
of administering a second dose to 1-dose vaccine recipients after exposure. However, administration of a second dose should
be considered for persons who have previously received 1 dose to bring them up-to-date. Studies on postexposure use of
varicella vaccine have been conducted exclusively in children. A higher proportion of adults do not respond to the first dose of
varicella vaccine. Nevertheless, postexposure vaccination should be offered to adults without evidence of immunity.
Although postexposure use of varicella vaccine has potential applications in hospital settings, vaccination is recommended routinely
for all HCP without evidence of immunity and is the preferred method for preventing varicella in health-care settings
(195). Preferably, HCP should be vaccinated when they begin employment. No data are available on the use of combination
MMRV raccine for postexposure prophylaxis.
Persons Without Evidence of Immunity Who Have Contraindications
for Vaccination and Who Are at Risk for Severe Disease and Complications
Studies conducted in 1969 indicated that clinical varicella was prevented in nonimmune, healthy children by
the administration of zoster immune globulin (ZIG) (prepared from patients recovering from HZ) within 72 hours of
exposure (196). ZIG also lowered attack rates among immunocompromised persons if administered no later than 96 hours
after exposure (196). VZIG (prepared from plasma obtained from healthy, volunteer blood donors identified by routine
screening to have high antibody titers to VZV) became
available in 1978. Both serologic and clinical evaluations have demonstrated
that the product is equivalent to ZIG in preventing or modifying clinical illness in non-immune, immunocompromised
persons who are exposed to varicella
(197,198). In a study of immunocompromised children who were administered VZIG within
96 hours of exposure, approximately one in five exposures resulted in clinical varicella, and one in 20 resulted in
subclinical disease (198). The severity of clinical varicella (evaluated by percentage of
patients with >100 lesions or complications)
was lower than expected on the basis of historic controls.
The VZIG product currently used in the United States,
VariZIG™(Cangene Corporation, Winnipeg, Canada), is
available under an Investigational New Drug Application
Expanded Access protocol (available at
http://www.fda.gov/cber/infosheets/mphvzig020806.htm). A request for licensure in the United States might be submitted to FDA in the
future. VariZIG is a lyophilized presentation which, when properly reconstituted, is approximately a 5% solution of IgG that can be
administered intramuscularly (199). VariZIG can be
obtained 24 hours a day from the sole authorized U.S.
distributor (FFF Enterprises, Temecula, California) at 1-800-843-7477 or online at
http://www.fffenterprises.com.
Administration of VZIG
VZIG provides maximum benefit when administered as soon as possible after exposure, but it might be effective
if administered as late as 96 hours after exposure. The effectiveness of VZIG when administered >96 hours after
initial exposure has not been evaluated. The duration of protection provided after administration of VZIG is unknown,
but protection should last at least one half-life of the IG (i.e.,
approximately 3 weeks). Susceptible persons at high risk for
whom varicella vaccination is contraindicated and who are again exposed
>3 weeks after receiving a dose of VZIG should
receive another full dose of VZIG. Patients receiving monthly high-dose immune globulin intravenous (IGIV)
(>400 mg/kg) are likely to be protected and probably do not require VZIG if the last dose of IGIV was administered <3 weeks before
exposure (200). VZIG has not been proven to be useful in treating clinical varicella or HZ or in preventing disseminated zoster and
is not recommended for such use. VZIG might extend the incubation period of the virus from 10--21 days to
>28 days. This should be taken into account after exposures when VZIG is administered.
Dosage
VariZIG is supplied in 125-U vials. The recommended dose is 125 units/10 kg of body weight, up to a maximum of
625 units (five vials). The minimum dose is 125 U. The human IgG content is 60--200 mg per 125 units dose of VariZIG.
Indications for the Use of VZIG for Postexposure Prophylaxis
The decision to administer VZIG depends on three factors: 1) whether the patient lacks evidence of immunity, 2)
whether the exposure is likely to result in infection, and 3) whether the patient is at greater risk for complications than the
general population.
Both healthy and immunocompromised children and adults who have verified positive histories of varicella (except
for bone-marrow transplant recipients) may be considered immune (see Evidence of Immunity). The association between
positive histories of varicella in bone-marrow donors and susceptibility to varicella in recipients after transplants has not been
studied adequately. Thus, persons who receive bone-marrow transplants should be considered nonimmune, regardless of
previous history of varicella disease or varicella vaccination in themselves or in their donors. Bone-marrow recipients in whom
varicella or HZ develops after transplantation should subsequently be considered immune.
VZIG is not indicated for persons who received 2 doses of varicella vaccine and became immunocompromised as a
result of disease or treatment later in life. These persons should be monitored closely; if disease occurs, treatment with acyclovir
should be instituted at the earliest signs or symptoms. For patients without evidence of immunity and on steroid therapy doses
>2 mg/kg of body weight or a total of 20 mg/day of prednisone or equivalent, VariZIG is indicated.
Types of Exposure
Certain types of exposure can place persons without evidence of immunity at risk for varicella. Direct contact exposure
is defined as face-to-face contact with an infectious person while indoors. The duration of face-to-face contact that
warrants administration of VZIG is not certain. However, the contact should not be transient. Certain experts suggest a contact of
>5 minutes as constituting significant exposure for this purpose, whereas others define close contact as >1 hour
(200). Substantial exposure for hospital contacts consists of sharing the same hospital room with an infectious patient or direct,
face-to-face contact with an infectious person (e.g., HCP). Brief contacts with an infectious person (e.g., contact with x-ray technicians
or housekeeping personnel) are less likely than more
prolonged contacts to result in VZV transmission.
Persons with continuous exposure to household members who have varicella or disseminated HZ are at greatest risk
for infection. Varicella occurs in approximately 85% (range: 65%--100%) of susceptible household contacts exposed to
VZV. Localized HZ is much less infectious than varicella or disseminated HZ
(52). Transmission from localized HZ is more
likely after close contact, such as in household settings. Physicians may consider recommending postexposure prophylaxis
with VZIG in such circumstances. After household exposure to varicella, attack rates among immunocompromised children
who were administered VZIG were up to 60%
(197). No comparative data are available for immunocompromised
children without evidence of immunity who were not administered VZIG. However, the incidence of severe disease
(defined as >100 skin lesions) was less than that predicted from the natural history of disease in normal children (27% and 87%,
respectively), and the incidence of pneumonia was less than that described in children with neoplasm (6% and 25%, respectively)
(201). The risk for varicella after close contact (e.g., contact with playmates) or hospital exposure is estimated to be
approximately 20% of the risk occurring from household exposure.
The attack rate in healthy neonates who were exposed in utero within 7 days of delivery and who received VZIG after
birth was 62%, which does not differ substantially from rates reported for neonates who were similarly exposed but not treated
with VZIG (49). However, the occurrence of complications and fatal outcomes was substantially lower for neonates who
were treated with VZIG than for those who were not.
In a study of pregnant women without immunity to VZV who were exposed to varicella and administered VZIG,
the infection rate was 30%. This is substantially lower than the expected rate of >70% in unimmunized women exposed
to varicella (199,202).
Recommendations for the Use of VZIG
The following patient groups are at risk for severe disease and complications from varicella and should receive VZIG:
Immunocompromised patients. VZIG is used primarily for passive immunization of immunocompromised
persons without evidence of immunity after direct exposure to varicella or disseminated HZ patients, including persons who 1)
have primary and acquired immune-deficiency disorders, 2) have neoplastic diseases, and 3) are receiving
immunosuppressive
treatment. Patients receiving monthly high-dose IGIV
(>400 mg/kg) are likely to be protected and probably do not
require VZIG if the last dose of IGIV was administered
<3 weeks before exposure (200).
Neonates whose mothers have signs and symptoms of varicella around the time of
delivery. VZIG is indicated for neonates whose mothers have signs and symptoms of varicella from 5 days before to 2 days after delivery. VZIG is
not necessary for neonates whose mothers have signs and symptoms of varicella more than 5 days before delivery, because
those infants should be protected from severe varicella by transplacentally acquired maternal antibody. No evidence suggests
that infants born to mothers in whom varicella occurs >48 hours after delivery are at increased risk for serious complications
(e.g., pneumonia or death).
Premature neonates exposed postnatally. Transmission of varicella in the hospital nursery is rare because the majority
of neonates are protected by maternal antibody. Premature
infants who have substantial postnatal exposure should be
evaluated on an individual basis. The risk for complications of postnatally acquired varicella in premature infants is
unknown. However, because the immune system of premature infants is not fully developed, administration of VZIG to premature infants born
at >28 weeks of gestation who are exposed during the neonatal period and whose mothers do not have evidence of immunity
is indicated. Premature infants born at <28 weeks of gestation or who weigh
<1,000 g at birth and were exposed during
the neonatal period should receive VZIG regardless of maternal immunity because such infants might not have acquired
maternal antibody. The majority of premature infants born at
>28 weeks of gestation to immune mothers have enough
acquired maternal antibody to protect them from severe disease and complications.
Although infants are at higher risk than older children for serious and fatal complications, the risk for healthy, full-term infants who have varicella after postnatal exposure
is substantially less than that for infants whose mothers were infected
5 days before to 2 days after delivery. VZIG is
not recommended for healthy, full-term infants who are exposed postnatally, even if their mothers have no history of
varicella infection.
Pregnant women. Because pregnant women might be at higher risk for severe varicella and complications
(37,42,203), VZIG should be strongly considered for pregnant women without evidence of immunity who have been
exposed. Administration of VZIG to these women has not been found to prevent viremia, fetal infection, congenital varicella
syndrome, or neonatal varicella. Thus, the primary indication for VZIG in pregnant women is to prevent complications of
varicella in the mother rather than to protect the fetus.
Neonates born to mothers who have signs and symptoms of varicella from 5
days before to 2 days after delivery should receive VZIG, regardless of whether the mother received VZIG.
Interval Between Administration of VZIG and Varicella Vaccine
Any patient who receives VZIG to prevent varicella should receive varicella vaccine subsequently, provided the vaccine is
not contraindicated. Varicella vaccination should be delayed until 5 months after VZIG administration. Varicella vaccine is
not needed if the patient has varicella after administration of VZIG.
Antiviral Therapy
Because VZIG might prolong the incubation period by
>1 week, any patient who receives VZIG should be observed
closely for signs or symptoms of varicella for 28 days after exposure. Antiviral therapy should be instituted immediately if signs
or symptoms of varicella disease occur. The route and duration of antiviral therapy should be determined by specific host
factors, extent of infection, and initial response to therapy. Information regarding how to obtain VariZIG is available at
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5508a5.htm
(204).
Acknowledgments
Gregory Wallace, MD, Mary Mulholland, MA, Tony Richardson, MS, MPH, Immunization Services Division, National Center
for Immunization and Respiratory Diseases, CDC, assisted in the writing of the section on vaccine storage and handling. Fangjun
Zhou, PhD, Immunization Services Division, National Center for Immunization and Respiratory Diseases, CDC, performed the
economic analysis. Jessica Leung, MPH, Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC, helped
with the graphs, tables, and references.
Lopez AS, Guris D, Zimmerman L, et al. One dose of varicella vaccine does not prevent school outbreaks: is it time for a second dose?
Pediatrics 2006;117:e1070--7.
Tugwell BD, Lee LE, Gillette H, Lorber EM, Hedberg K, Cieslak PR. Chickenpox outbreak in a highly vaccinated school
population. Pediatrics 2004;113:455--9.
Parker AA, Reynolds M, Leung J, et al. Challenges to implementing second dose varicella vaccination during an outbreak in the absence of a
routine two-dose vaccination requirement---Maine, 2006. J Infect Dis (suppl). In press 2007.
LaRussa P. Clinical manifestations of varicella. In: Arvin A, Gershon A, eds. Varicella-zoster virus. Cambridge, UK: Cambridge University
Press; 2000:206--19.
Wharton M. The epidemiology of varicella-zoster virus infections.
Infect Dis Clin N Amer 1996;10:571--81.
Finger R, Hughes JP, Meade BJ, et al. Age-specific incidence of chickenpox. Pub Health Rep 1994;190:750--5.
Yawn BP, Yawn RA, Lydick E. Community impact of childhood
varicella infections. J Pediatr 1997;130:759--65.
Kilgore PE, Kruszon-Moran D, Seward JF, et al. Varicella in Americans from NHANES III: implications for control through routine
immunization. J Med Virol 2003;70 Suppl 1:S111--8.
Longfield JN, Winn RE, Gibson RL, Juchau SV, Hoffman PV. Varicella outbreak in army recruits from Puerto Rico. Varicella susceptibility in
a population from the tropics. Arch Intern Med 1990;150:970--3.
Garnett GP, Cox MJ, Bundy DAP, Didier JM, St. Catherine J. The age of infection with varicella-zoster virus in St. Lucia, West Indies.
Epidemiol Infect 1993;110:361--72.
Lolekha S, Tanthiphabha W, Sornchai P, et al. Effect of climatic factors and population density on varicella zoster virus epidemiology within
a tropical country. Am J Trop Med Hyg 2001;64:131--6.
Mandal BK, Mukherjee PP, Murphy C, Mukherjee R, Naik T. Adult susceptibility to varicella in the tropics is a rural phenomenon due to the lack
of previous exposure. J Infect Dis 1998;178(Suppl):S52--4.
Seward J, Galil K, Wharton M. Epidemiology of varicella. In: Arvin A, Gershon A, eds. Varicella-zoster virus. Cambridge, UK:
Cambridge University Press; 2000:187--205.
Lee BW. Review of varicella zoster seroepidemiology in India and Southeast Asia. Trop Med Int Health 1998;3:886--90.
Galil K, Brown C, Lin F, Seward J. Hospitalizations for varicella in the United States, 1988 to 1999. Pediatr Infect Dis J 2002;21:931--5.
Ratner AJ. Varicella-related hospitalizations in the vaccine era. Pediatr Infect Dis J 2002;21:927--30.
Davis MM, Patel MS, Gebremariam A. Decline in varicella-related hospitalizations and expenditures for children and adults after introduction
of varicella vaccine in the United States. Pediatrics 2004;114:786--92.
Zhou F, Harpaz R, Jumaan AO, Winston CA, Shefer A. Impact of varicela vaccination on health care utilization. JAMA 2005;294: 797--802.
Hurwitz ES, Barrett MJ, Bregman D, et al. Public Health Service study on Reye's syndrome and medications. Report of the pilot phase. New Engl
J Med 1985;313:849--57.
Remington RL, Rowley D, McGee H, et al. Decreasing trends in Reye's syndrome and aspirin use in Michigan 1979 to 1984. Pediatrics
1986;77:93--8.
Belay ED, Bresee JS, Holman RC, et al. Reye's syndrome in the United States from 1981 through 1997. New Engl J Med 1999;340:1377--82.
Meyer P, Seward JF, Jumaan AO, Wharton M. Varicella mortality: trends before vaccine licensure in the United States, 1970--1994. J Infect
Dis 2000;182:383--90.
Nguyen HQ, Jumaan AO, Seward JF. Decline in mortality due to
varicella after implementation of varicella vaccination in the United States. N
Engl J Med 2005;352:450--8.
Enders G, Miller E. Varicella and herpes zoster in pregnancy and newborn. In: Arvin A, Gershon A, eds. Varicella-zoster virus. Cambridge,
UK: Cambridge University Press; 2000:317--47.
Luman ET, Ching PLYH, Jumaan AO, Seward JF. Uptake of varicella vaccination among young children in the United States: a success story
in eliminating racial and ethnic disparities. Pediatrics 2006;117: 999--1008.
Seward JF, Watson BM, Peterson CL, et al. Varicella disease after introduction of varicella vaccine in the United States, 1995--2000.
JAMA 2002;287:606--11.
Guris D, Jumaan AO, Mascola L, et al. Changing varicella epidemiology in active surveillance sites---United States, 1995--2005. J Infect
Dis (Suppl). In press 2007.
Galil K, Pletcher MJ, Wallace BJ, et al. Tracking varicella deaths: accuracy and completeness of death certificates and hospital discharge records,
New York State, 1989--1995. Am J Public Health 2002;92:1248--50.
Gershon AA, Raker R, Steinberg S, Topf-Olstein B, Drusin LM. Antibody to varicella-zoster virus in parturient women and their offspring
during the first year of life. Pediatrics 1976;58:692--6.
Paryani SG, Arvin AM. Intrauterine infection with varicella-zoster
virus after maternal varicella. N Engl J Med 1986;314:1542--6.
Brunell PA, Kotchmar GS. Zoster in infancy: failure to maintain virus latency following intrauterine infection. J Pediatr 1981;98:71--3.
Brunell PA. Varicella in pregnancy, the fetus, and the newborn: problems in management. J Infect Dis 1992;166(Suppl 1):S42--7.
Laforet EG, Lynch C. Multiple congenital defects following maternal varicella. N Engl J Med 1947;236:534--7.
Enders G. Varicella-zoster virus infection in pregnancy. Prog Med Virol 1984;29:166--96.
Enders G, Miller E, Cradock-Watson J, Bolley I, Ridehalgh M. Consequences of varicella and herpes zoster in pregnancy: prospective study of
1739 cases. Lancet 1994;343:1548--51.
Pastuszak AL, Levy M, Schick B, et al. Outcome after maternal varicella infection in the first 20 weeks of pregnancy. N Engl J Med
1994;330:901--5.
Meyers JD. Congenital varicella in term infants: risks reconsidered. J Infect Dis 1974;129:215--7.
Brunell PA. Fetal and neonatal varicella-zoster infections. Semin Perinatol 1983;7:47--56.
Tan MP, Koren G. Chickenpox in pregnancy: revisited. Reprod Toxicol 2006;21:e410--20.
Bai PV, John TJ. Congenital skin ulcers following varicella in late
pregnancy. J Pediatr 1979. 94:65--7.
Miller E, Cradock-Watson JE, Ridehalgh MK. Outcome in newborn babies given anti-varicella-zoster immunoglobin after perinatal
maternal infection with varicella-zoster virus. Lancet 1989;2:371--3.
Hope-Simpson RE. The nature of herpes zoster: a long-term study and a new hypothesis. Proc R Soc Med 1965;58:9--20.
Brisson M, Edmunds WJ, Law B, et al. Epidemiology of varicella zoster virus infection in Canada and the United Kingdom. Epidemiol
Infect 2001;127:305--14.
Seiler HE. A study of herpes zoster particularly in its relationship to chickenpox. J Hyg (Lond) 1949;47:253--62.
Takayama N, Takayama M, Takita J. Herpes zoster in healthy children immunized with varicella vaccine. Pediatr Infect Dis J 2000;19: 169--70.
Hardy I, Gershon AA, Steinberg S, et al. The incidence of zoster after immunization with live attenuated varicella vaccine. A study in children
with leukemia. N Engl J Med 1991;325:1545--50.
Lawrence R, Gershon AA, Holzman R, Steinberg SP, NIAID Varicella Vaccine Collaborative Study Group. The risk of zoster after
varicella vaccination in children with leukemia. N Engl J Med 1988;318: 543--8.
Black S, Shinefield H, Ray P, et al. Postmarketing evaluation of the safety and effectiveness of varicella vaccine. Pediatr Infect Dis J 1999;18:1041--6.
White CJ. Clinical trials of varicella vaccine in healthy children. Infect Dis Clin N Amer 1996;10:595--608.
Gershon AA. Varicella vaccine: rare serious problems---but the
benefits still outweigh the risks. J Infect Dis 2003;188:945--7.
Brisson M, Edmunds WJ, Gay NJ, Law B, De Serres G. Modeling the impact of immunization on the epidemiology of varicella-zoster
virus. Epidemiol Infect 2000;125:651--69.
Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF.
Incidence of herpes zoster, before and after
varicella-vaccination-associated decreases in the incidence of varicella, 1992--2002. J Infect Dis 2005;191:2002--7.
Insinga RP, Itzler RF, Pellissier JM, Saddier P, Nikas AA. The incidence of herpes zoster in a United States administrative database. J Gen
Intern Med 2005;20:748--53.
Mullooly JP, Riedlinger K, Chun C, Weinmann S, Houston H.
Incidence of herpes zoster, 1997--2002. Epidemiol Infect 2005; 133:245--53.
Yih WK, Brooks DR, Lett SM, et al. The incidence of varicella and herpes zoster in Massachusetts as measured by the Behavioral Risk
Factor Surveillance System (BRFSS) during a period of increasing varicella vaccine coverage, 1998--2003. BMC Public Health 2005;5:68.
Donahue JG, Choo PW, Manson JE, Platt R. The incidence of herpes zoster. Arch Intern Med 1995;155:1605--9.
Civen RH, Maupin TJ, Xiao H, Seward J, Jumaan AO, Mascola L. A population-based study of herpes zoster in children and adolescents
post-varicella vaccine licensure. Presented at the 41st Annual Meeting of the Infectious Disease Society of America, San
Diego, California; October 9--12, 2003.
Prober CG, Kirk LE, Keeney RE. Acyclovir therapy of chickenpox in immunosuppressed children---a collaborative study. J Pediatr 1982;101:622--5.
Balfour HH Jr. Intravenous acyclovir therapy for varicella in immunocompromised children. J Pediatr 1984;104:134--6.
Nyerges G, Meszner Z, Gyarmati E, Kerpel-Fronius S. Acyclovir
prevents dissemination of varicella in immunocompromised children. J Infect
Dis 1988;157:309--13.
Balfour HH, Kelly JM, Suarez CS, et al. Acyclovir treatment of
varicella in otherwise healthy children. J Pediatr 1990;116:633--9.
Dunkle LM, Arvin AM, Whitley RJ, et al. A controlled trial of acyclovir for chickenpox in normal children. N Engl J Med 1991;325:1539--44.
Balfour HH Jr, Rotbart HA, Feldman S, et al. Acyclovir treatment of varicella in otherwise healthy adolescents. J Pediatr 1992;120:627--33.
Wallace MR, Bowler WA, Murray NB, Brodine SK, Oldfield EC III. Treatment of adult varicella with oral acyclovir. Ann Intern
Med 1992;117:358--63.
Feder HM Jr. Treatment of adult chickenpox with oral acyclovir. Arch Intern Med 1990;150:2061--5.
Committee on Infectious Diseases, American Academy of Pediatrics. The use of oral acyclovir in otherwise healthy children with varicella.
Pediatrics 1993;91:674--6.
Stone KM, Reiff-Eldridge R, White AD, et al. Pregnancy outcomes following systemic prenatal acyclovir exposure: conclusions from
the International Acyclovir Pregnancy Registry, 1984--1999. Birth Defects Research 2004 (Pt A)70:201--7.
Huff JC, Bean B, Balfour HH Jr., et al. Therapy of herpes zoster with oral acyclovir. Am J Med 1988;85 (Suppl 2A):84--9.
Anonymous Famciclovir for herpes zoster. The Medical Letter on Drugs and Therapeutics 1994;36:97--8.
Takahashi M, Otsuka T, Okuno Y, Asano Y, Yazaki T. Live vaccine used to prevent the spread of varicella in children in hospital.
Lancet 1974;2:1288--90.
White CJ, Kuter BJ, Hildebrand CS, et al. Varicella vaccine (VARIVAX) in healthy children and adolescents: results from clinical trials, 1987
to 1989. Pediatrics 1991;87:604--10.
Michalik DE, LaRussa PS, Steinberg SP, Wright P, Edwards K, Gershon AA. Primary immune failure after one dose of varicella vaccine are likely
a cause of breakthrough infections in healthy vaccinated children. In: 44th Infectious Disease Society of America Annual Meeting, Toronto,
Ontario, Canada; October 11--14, 2006.
Chan ISF, Li S, Matthews H, et al. Use of statistical models for evaluating antibody response as a correlate of protection against varicella. Stat
Med 2002;21:3411--30.
Li S, Chan ISF, Matthews H, et al. Inverse relationship between six week postvaccination varicella antibody response to vaccine and likelihood
of long term breakthrough infection. Pediatr Infect Dis J 2002;21:337--42.
Kuter B, Matthews H, Shinefield H, et al. Ten year follow-up of healthy children who received one or two injections of varicella
vaccine. Pediatr Infect Dis J 2004;23:132--7.
Johnson CE, Stancin T, Fattlar D, Rome LP, Kumar ML. A long-term prospective study of varicella vaccine in healthy children.
Pediatrics 1997;100:761--6.
Asano Y, Nagai T, Miyata T, et al. Long-term protective immunity of recipients of the OKA strain of live varicella vaccine. Pediatrics
1985;75:667--71.
Asano Y, Suga S, Yoshikawa T, et al. Experience and reason: twenty-year follow-up of protective immunity of the Oka strain live varicella
vaccine. Pediatrics 1994;94:524--6.
Watson B, Rothstein E, Bernstein H, et al. Safety and cellular and humoral immune responses of a booster dose of varicella vaccine 6 years
after primary immunization. J Infect Dis 1995;172:217--9.
Shinefield H, Black S, Digilio L, et al. Evaluation of a quadrivalent measles, mumps, rubella and varicella vaccine in healthy children. Pediatr
Infect Dis J 2005;24:665--9.
Reisinger KS, Hoffman Brown ML, Xu J, et al. A combination measles, mumps, rubella, and varicella vaccine (ProQuad) given to 4- to
6-year-old healthy children vaccinated previously with M-M-RII and Varivax. Pediatrics 2006;117:265--72.
Kuter BJ, Ngai A, Patterson CM, et al. Safety, tolerability, and
immunogenicity of two regimens of Oka/Merck varicella vaccine
(Varivax®) in healthy adolescents and adults. Vaccine 1995;13: 967--72.
Gershon AA, Steinberg SP, LaRussa P, et al. NIAID
-Varicella-Vaccine-Collaborative -Study-Group. Immunization of healthy adults with
live attenuated varicella vaccine. J Infect Dis 1988;158:132--7.
Saiman L, LaRussa P, Steinberg SP, et al. Persistence of immunity to varicella-zoster virus vaccination among health care workers. Inf Cont
Hosp Epidemiol 2001;22:279--83.
Ampofo K, Saiman L, LaRussa P, Steinberg S, Annunziato P, Gershon A. Persistence of immunity to live attenuated varicella vaccine in
healthy adults. Clin Infect Dis 2002;34:774--9.
Zerboni L, Nader S, Aoki K, Arvin AM. Analysis of the persistence of humoral and cellular immunity in children and adults immunized
with varicella vaccine. J Infect Dis 1998;177:1701--4.
Watson B, Boardman C, Laufer D, et al. Humoral and cell-mediated immune responses in healthy children after one or two doses of
varicella vaccine. Clin Infect Dis 1995;20:316--9.
Nader S, Bergen R, Sharp M, Arvin AM. Age-related differences in cell-mediated immunity to varicella-zoster virus in children and
adults immunized with live attenuated varicella vaccine. J Infect Dis 1995;171:13--7.
White CJ, Kuter BJ, Ngai A, et al. Modified cases of chickenpox after varicella vaccination: correlation of protection with antibody
response. Pediatr Infect Dis J 1992;11:19--23.
Krah DL, Cho I, Schofield T, Ellis RW. Comparison of gpELISA and neutralizing antibody responses to Oka/Merck live varicella
vaccine (VARIVAX®) in children and adults. Vaccine 1997;15:61--4.
Arbeter AM, Starr SE, Plotkin SA. Varicella vaccine studies in healthy children and adults. Pediatrics 1986;78 (Suppl):748--56.
Krause PR, Klinman DM. Efficacy, immunogenicity, safety, and use of live attenuated chickenpox vaccine. J Pediatr 1995;127:518--25.
Weibel RE, Neff BJ, Kuter BJ, et al. Live attenuated varicella virus vaccine: efficacy trial in healthy children. N Engl J Med 1984;310:1409--15.
Gershon AA, Takahashi M, Seward J. Varicella vaccine. In: Plotkin SA, Orenstein WA, eds. Vaccines. 4th ed. Philadelphia: WB Saunders
Company; 2004.
Kuter BJ, Weibel RE, Guess HA, et al. Oka/Merck varicella vaccine in healthy children: final report of a 2-year efficacy study and 7-year
follow-up studies. Vaccine 1991;9:643--7.
Seward JF, Marin M, Vasquez M. Varicella vaccine effectiveness in the United States vaccination program: a review. J Infect Dis (Suppl). In
press 2007.
Buchholz U, Moolenaar R, Peterson C, Mascola L. Varicella outbreaks after vaccine licensure: should they make you chicken?
Pediatrics 1999;104:561--3.
Dworkin MS, Jennings CE, Roth-Thomas J, et al. An outbreak of varicella among children attending preschool and elementary school in
Illinois. Clin Infect Dis 2002;35:102--4.
Izurieta HS, Strebel PM, Blake PA. Postlicensure effectiveness of
varicella vaccine during an outbreak in a child care center. JAMA
1997;278:1495--9.
Galil K, Fair E, Mountcastle N, Britz P, Seward J. Younger age at vaccination may increase risk of varicella vaccine failure. J Infect
Dis 2002;186:102--5.
Marin M, Nguyen HQ, Keen J, et al. Importance of catch-up vaccination: experience from a varicella outbreak, Maine, 2002--2003.
Pediatrics 2005;115:900--5.
Haddad MB, Hill MB, Pavia AT, et al. Vaccine effectiveness during a varicella outbreak among schoolchildren: Utah, 2002--2003.
Pediatrics 2005;115:1488--93.
Galil K, Lee B, Strine T, et al. Outbreak of varicella at a day-care center despite vaccination. N Engl J Med 2002;347:1909--15.
Lee BR, Feaver SL, Miller CA, Hedberg CW, Ehresmann KR. An elementary school outbreak of varicella attributed to vaccine failure:
policy implications. J Infect Dis 2004;190:477--83.
Clements DA, Moreira SP, Coplan PM, Bland CL, Walter EB. Postlicensure study of varicella vaccine effectiveness in a day-care
setting. Pediatr infect Dis J 1999; 18:1047--50.
Vázquez MD, LaRussa PS, Gershon AA, Steinberg SP,
Freudigman KF, Shapiro E. The effectiveness of the varicella vaccine in clinical
practice. N Engl J Med 2001;344:955--60.
Vázquez MD, LaRussa PS, Gershon AA, et al. Effectiveness over time of varicella vaccine. JAMA 2004;291:851--5.
Seward JF, Zhang JX, Maupin TJ, Mascola L, Jumaan AO. Contagiousness of varicella in vaccinated cases: a household contact study.
JAMA 2004;292:704--8.
Bernstein HH, Rothstein EP, Pennridge Pediatric Associates, et al. Clinical survey of natural varicella compared with breakthrough
varicella after immunization with live attenuated Oka/Merck
varicella vaccine. Pediatrics 1993;92:833--7.
Watson BM, Piercy SA, Plotkin SA, Starr SE. Modified chickenpox in children immunized with the Oka/Merck varicella
vaccine. Pediatrics 1993;91:17--22.
Arbeter AM, Starr SE, Preblud SR, et al. Varicella vaccine trials in healthy children: a summary of comparative and follow-up studies. Am J
Dis Child 1984;138:434--8.
Vessey SJR, Chan CY, Kuter BJ, et al. Childhood vaccination against varicella: persistence of antibody, duration of protection, and vaccine
efficacy. J Pediatr 2001;139:297--304
Chaves SS, Zhang J, Civen R, et al. Varicella disease in vaccinated persons: clinical and epidemiologic characteristics, 1997--2005. J Infect
Dis (Suppl). In press 2007.
Verstraeten T, Jumaan AO, Mullooly JP, et al. Vaccine Safety Datalink Research Group. A retrospective cohort study of the association of
varicella vaccine failure with asthma, steroid use, age at vaccination, and measles-mumps-rubella vaccination. Pediatrics 2003;112: e98--103.
Chaves SS, Gargiullo P, Zhang JX, et al. Loss of vaccine-induced
immunity to varicella over time. N Engl J Med 2007;356:1121--9.
Black S, Ray P, Shinefield H, Saddier P and Nikas A. Lack of association of age at varicella vaccination with risk of breakthrough disease
within Northern California Kaiser Permanente. J Infect Dis. In press 2007.
Peterson CL, Vugia DJ, Meyers HB, et al. Risk factors for invasive group A streptococcal infections in children with varicella: a case-control
study. Pediatr Infect Dis J 1996;15:151--6.
Dowell SF, Bresee JS. Severe varicella associated with steroid use.
Pediatrics 1993;92:223--8.
Alter SJ, Hammond JA, McVey CJ, Myers MG. Susceptibility to
varicella-zoster virus among adults at high risk for exposure. Am J Infect
Control 1986;7:448--51.
Struewing JP, Hyams KC, Tueller JE, Gray GC. The risk of measles, mumps, and varicella among young adults: a serosurvey of US Navy
and Marine Corps recruits. Am J Public Health 1993;83:1717-- 20.
McKinney WP, Horowitz MM, Battiola RJ. Susceptibility of hospital-based health care personnel to varicella-zoster virus infections. Am J
Infect Control 1989;17:26--30.
Perella D, Fiks A, Spain CV, et al. Validity of reported varicella history as a marker for varicella-zoster virus immunity [Poster]. 2005
Pediatric Academic Societies Annual Meeting, Washington, DC; May 14--17, 2005.
Englund JA, Suarez CS, Kelly J, Tate DY, Balfour HH.
Placebo-controlled trial of varicella vaccine given with or after
measles-mumps-rubella vaccine. J Pediatr 1989;114:37--44.
Black SB, Cimino CO, Hansen, J, et al. Immunogenicity and safety of measles-mumps-rubella, varicella and
Haemophilus influenzae type b vaccines administered concurrently with a fourth dose of heptavalent pneumococcal conjugate vaccine compared with the vaccines
administered without heptavalent pneumococcal conjugate vaccine. Pediatr Infect Dis J 2006;25:306--11.
Shinefield H, Black S, Thear M, et al. Safety and immunogenicity of a measles, mumps, rubella and varicella vaccine given with
combined Haemophilus influenzae type b conjugate/hepatitis B vaccines and combined diphteria-tetanus-acellular pertusis vaccines. Pediatr Infect Dis
J 2006;25:287--92.
Lieu TA, Cochi SL, Black SB, et al. Cost-effectiveness of a routine varicella vaccination program for U.S. Children. JAMA 1994; 271:375--81.
Ngai AL, Stahele BO, Kuter BJ, et al. Safety and immunogenicity of one vs. two injections of Oka/Merck varicella vaccine in healthy
chidren. Pediatr infect Dis J 1996;15:49--54.
Sharrar RG, LaRussa P, Galea SA, et al. The postmarketing safety profile of varicella vaccine. Vaccine 2001;19:916--23.
Wise RP, Salive ME, Braun MM, et al. Postlicensure safety surveillance for varicella vaccine. JAMA 2000;284:1271--9.
Guess HA, Broughton DD, Melton LJ, 3rd, Kurland LT.
Population-based studies of varicella complications. Pediatrics 1986;78 (4 Pt 2):723--7.
Ghaffar F, Carrick K, Rogers BB, Margraf LR, Krisher K, Ramilo O. Disseminated infection with varicella-zoster virus vaccine strain presenting
as hepatitis in a child with adenosine deaminase deficiency. Pediatr Infect Dis J 2000;19:764--6.
Levy O, Orange JS, Hibberd P, et al. Disseminated varicella infection due to the vaccine strain of varicella-zoster virus, in a patient with a
novel deficiency in natural killer T cells. J Infect Dis 2003;188: 948--53.
Levin MJ, Dahl KM, Weinberg A, Giller R, Patel A, Krause PR.
Development of resistance to acyclovir during chronic infection with the
Oka vaccine strain of varicella-zoster virus, in an immunosuppressed child. J Infect Dis 2003;188:954--9.
Grossberg R, Harpaz R, Rubtcova E, Loparev V, Seward JF, Schmid DS. Secondary transmission of varicella vaccine virus in a chronic care
facility for children. J Pediatr 2006;148:842--4.
Salzman MB, Sharrar RG, Steinberg S, LaRussa P. Transmission of
varicella-vaccine virus from a healthy 12 month old child to
his pregnant mother. J Pediatr 1997;131:151--4.
Tsolia M, Gershon AP, Steinberg SP, Gelb L. Live attenuated varicella vaccine: evidence that the virus is attenuated and the importance of
skin lesions in transmission of varicella-zoster virus. J Pediatr 1990;116:184--9.
Lee SY, Komp DM, Andiman W. Thrombocytopenic purpura following varicella-zoster vaccination. Am J Pediatr Hematol Oncol 1986;8:78--80.
Sunaga Y, Hikima A, Ostuka T, Morikawa A. Acute cerebellar ataxia with abnormal MRI lesions after varicella vaccination. Pediatr
Neurol 1995;13:340--2.
Wirrell E, Hill MD, Jadavji T, Kirton A, Barlow K. Stroke after
varicella vaccination. J Pediatr 2004;145:845--7.
Singer S, Johnson CE, Mohr R, Holowecky C. Urticaria following varicella vaccine associated with gelatin allergy. Vaccine 1999;17: 327--9.
Bronstein DE, Cotliar J, Votava-Smith JK, et al. Recurrent papular urticaria after varicella immunization in a fifteen-month-old girl. Pediatr
Infect Dis J 2005;24:269--70.
Guess HA, Broughton DD, Melton LJ, Kurland LT. Epidemiology of herpes zoster in children and adolescents: a population-based study.
Pediatrics 1985;76:512--7.
Diaz PS, Au D, Smith S. Lack of transmission of the live attenuated varicella vaccine virus to immunocompromised children after immunization
of their siblings. Pediatrics 1991;87:166--70.
Brunell PA, Argaw T. Chickenpox attributable to a vaccine virus
contracted from a vaccinee with zoster. Pediatrics 2000;106:e28.
Levin MJ, Gershon AA, Weinberg A, Song LY, Fentin T, Nowak B; Pediatric AIDS Clinical Trials Group 265 Team. Administration of live
varicella vaccine to HIV-infected children with current or past significant depression of CD4(+) T cells. J Infect Dis 2006;194: 247--55.
Takahashi M, Kamiya H, Baba K, Ozaki T, Horiuchi K. Clinical
experience with Oka live varicella vaccine in Japan. Postgrad Med
J 1985;61(Suppl):61--7.
Bohlke K, Galil K, Jackson LA, et al. Postpartum varicella vaccination: is the vaccine virus excreted in breast milk? Obstet Gynecol 2003;102:970
--7.
Dolbear GL, Moffat J, Falkner C, Wojtowycz M. A pilot study: is attenuated varicella virus present in breast milk after postpartum
immunization? Obstet Gynecol 2003;101(Suppl):S47.
Meyers JD, MacQuarrie MB, Merigan TC, Jennison MH. Nosocomial varicella. Part 1: outbreak in oncology patients at a children's hospital.
West J Med 1979;130:196--9.
Morens DM, Bregman DJ, West CM, et al. An outbreak of varicella-zoster virus infection among cancer patients. Ann Intern Med
1980;93:414--9.
Baltimore RS. Nosocomial infections in the pediatric intensive care unit. Yale J Biol Med 1984;57:185--97.
Gustafson TL, Shehab Z, Brunell PA. Outbreak of varicella in a newborn intensive care nursery. Am J Dis Child 1984;138:548--50.
Hyams PJ, Stuewe MC, Heitzer V. Herpes zoster causing varicella (chickenpox) in hospital employees: cost of a casual attitude. Am J Infect
Control 1984;12:2--5.
Shehab ZM, Brunell PA. Susceptibility of hospital personnel to
varicella-zoster virus. J Infect Dis 1984;150:786.
Weitekamp MR, Schan P, Aber RC. An algorithm for the control of nosocomial varicella-zoster virus infection. Am J Infect Control
1985;13:193--8.
Krasinski K, Holzman RS, LaCouture R, Florman A. Hospital experience with varicella-zoster virus. Infect Control 1986;7:312-- 6.
Haiduven-Griffiths D, Fecko H. Varicella in hospital personnel: a challenge for the infection control practitioner. Am J Infect
Control 1987;15:207--11.
Weber DJ, Rutala WA, Parham C. Impact and costs of varicella
prevention in a university hospital. Am J Public Health 1988;78: 19--23.
Garner JS. Guidelines for isolation precautions in hospitals. Infect Cont Hosp Epid 1996;17:54--80.
Bolyard EA, Tablan, OC, Williams WW. Et al. Guideline for infection control in healthcare personnel, 1998: Hospital Infection Control
Practices Advisory Committee. Infect Cont Hosp Epid 1999;19:407--63.
Asano Y, Iwayama S, Miyata T, et al. Spread of varicella in hospitalized children having no direct contact with an indicator zoster case and
its prevention by a live vaccine. Biken J 1980;23:157--61.
Leclair JM, Zaia JA, Levine MJ, Congdon RG, Goldmann DA. Airborne transmission of chickenpox in a hospital. N Engl J Med
1980;302:450--3.
Gustafson TL, Lavely GB, Brawner ER, Hutcheson RH, Wright PF, Schaffner W. An outbreak of airborne nosocomial varicella.
Pediatrics 1982;70:550--6.
Josephson A, Gombert ME. Airborne transmission of nosocomial varicella from localized zoster. J Infect Dis 1988;158:238--41.
Sawyer MH, Chamberlin CJ, Wu YN, Aintablian N, Wallace MR. Detection of varicella-zoster virus DNA in air samples from hospital room.
J Infect Dis 1994;169:91--4.
Steinberg SP, Gershon AA. Measurement of antibodies to varicella-zoster virus by using a latex agglutination test. J Clin Microbiol
1991;29:1527--9.
Gershon AA, LaRussa PS, Steinberg SP. Detection of antibodies to varicella zoster virus using a latex agglutination assay. Clin Diag
Virol 1994;2:271--7.
Behrman A, Schmid DS, Crivaro A, Watson B. A cluster of primary varicella cases among healthcare workers with false-positive varicella
zoster virus titers. Infect Control Hosp Epidemiol 2003;24:202--6.
Hall S, Galil K, Seward J and Watson B. The use of school-based vaccination clinics to control varicella outbreaks in two schools.
Pediatrics 2000; 105:e17--20.
Lydick E, Kuter BJ, Zajac BA, Guess HA, The National Institute of Allergy and Infectious Diseases Varicella Vaccine Collaborative Study
Group. Association of steroid therapy with vaccine-associated rashes in children with acute lymphocytic leukaemia who received Oka/Merck
varicella vaccine. Vaccine 1989;7:549--53.
Shields KE, Galil K, Seward J, Sharrar RG, Cordero JF, Slater E.
Varicella vaccine exposure during pregnancy: data from the first
5 years of the pregnancy registry. Obstet Gynecol 2001;98:14--9.
Wilson E, Goss MA, Marin M, et al. Varicella vaccine exposure during pregnancy: data from ten years of the pregnancy registry. J Infect Dis.
In press 2007.
Dennehy PH, Saracen CL, Peter G. Seroconversion rates to combined measles-mumps-rubella-varicella (MMRV) vaccine of children with
upper respiratory tract infection. Pediatrics 1994;94:514--6.
Farizo KM, Stehr-Green PA, Markowitz LE, Patriarca PA. Vaccination levels and missed opportunities for measles vaccination: a record audit in
a public pediatric clinic. Pediatrics 1992;89:589--92.
Siber GR, Werner BG, Halsey NA, et al. Interference of immune globulin with measles and rubella immunization. J Pediatr 1993;122:204--11.
Asano Y, Nakayama H, Yazaki T, et al. Protection against varicella in family contacts by immediate inoculation with live varicella
vaccine. Pediatrics 1977;59:3--7.
Salzman MB and Garcia C. Post exposure varicella vaccination in siblings of children with active varicella. Pediatr Infect Dis J 1998;17:256--7.
Watson B, Seward J, Yang A, et al. Postexposure effectiveness of varicella vaccine. Pediatrics 2000;105:84--8.
Zaia J, Levin MJ, Preblud SK, et al. Evaluation of varicella-zoster
immune globulin: protection of immunosuppressed children after
household exposure to varicella. J Infect Dis 1983;147:737--43.
Levin MJ, Nelson WL, Preblud SR, Zaia JA. Clinical trials with varicella-zoster imunoglobulins, in Movell A, Nydegger, eds. Clinical use
of intravenous imunoglobulins. London, UK: Academic Press Inc., Ltd; 1986:255--67.
American Academy of Pediatrics. Varicella-zoster infections. In: Pickering LK, ed. Red book: 2006 report of the Committee on Infectious
Diseases. 27th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006:711--25.
Zaia JA, Levin MJ, Preblud SR. The status of passive immunization for Herpesvirus infections. In: Alving BM, Finlayson JS,
eds. Immunoglobulins: characteristics and use of intravenous preparations. Bethesda, MD: US Department of Health and Human Services;
1980 (DHHS publication no. [FDA] 80-9005):111--21.
Wallace MR, Bowler WA, Murray NB, Brodine SK, Oldfield EC III. Treatment of adult varicella with oral acyclovir. Ann Intern
Med 1992;117:358--63.
Haris RE, Rhoades ER. Varicella pneumonia complicating pregnancy: report of a case and review of the literature. Obstet Gynecol
1965;25:734--40.
* During the preparation of this report, Dalya Güris was an employee with the Division of Viral Diseases, National Center for Immunization and
Respiratory
Diseases, CDC. She presently is employed by Merck, Inc., Whitehouse Station, New Jersey.
† In this report, efficacy refers to the extent to which a specific intervention produces a beneficial result under ideal conditions.
§ The en dash in numeric ranges is used to represent inclusive years, hours, days, ages, dosages, or a sequence of numbered items.
¶ In this report, effectiveness refers to the extent to which a specific intervention, when deployed in the field, does what it is intended to do for a
defined population.
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Appendix
Summary of Recommendations for Varicella Vaccination
Routine Childhood Schedule
Routine childhood vaccination should be 2 doses.
Preschool-aged children should receive the first dose of varicella vaccine at age 12--15 months.
School-aged children should receive the second dose at age 4--6 years (may be administered earlier provided
>3 months have elapsed after the first dose)
Persons Aged >13 Years
Persons aged >13 years should receive 2 doses of vaccine, doses (4--8 weeks apart).
All adolescents and adults without evidence of immunity should be vaccinated.
Because of their increased risk for transmission to persons at high risk for severe disease or their increased risk of
exposure, vaccination is especially important for persons without evidence of immunity in the following groups:
--- persons who have close contact with persons at high risk for serious complications (e.g., health-care personnel and
household contacts of immunocompromised persons);
--- persons who live or work in environments in which transmission of varicella zoster virus is likely (e.g., teachers,
child-care workers, and residents and staff in institutional settings);
--- persons who live and work in environments in which transmission has been reported (e.g., college students, inmates
and staff members of correctional institutions, military personnel);
--- nonpregnant women of childbearing age;
--- adolescents and adults living in households with
children; and
--- international travelers.
Prenatal Assessment and Postpartum Vaccination
Prenatal assessment of women for evidence of varicella
immunity is recommended. Upon completion or termination
of pregnancy, women who do not have evidence of varicella immunity should be vaccinated.
Vaccination of HIV-Infected Persons
Vaccination should be considered for HIV-infected children with age-specific CD4+ T-lymphocyte percentage
>15% and may be considered for adolescents and adults in with CD4+ T-lymphocyte count
>200 cells/µL.
Outbreak Control
2-dose vaccination policy
Postexposure Prophylaxis
Recommended within 3--5 days
Requirements for Entry to Child Care, School, College, and Other
Postsecondary Educational Institutions
All states should require that students at all grade levels
(including college) and those in child care centers
receive varicella vaccine unless they have other evidence of immunity of varicella.
Evidence of Immunity to Varicella
Evidence of immunity to varicella includes any of the
following:
documentation of age-appropriate vaccination with a varicella vaccine:
--- preschool-aged children (i.e., aged
>12 months): 1 dose
--- school-aged children, adolescents, and adults: 2 doses*
laboratory evidence of
immunity† or laboratory confirmation of disease;
birth in the United States before
1980§;
diagnosis or verification of a history of varicella disease by a health-care
provider¶; or
diagnosis or verification of a history of herpes zoster by a health-care provider.
* For children who received their first dose at age <13 years and for whom the interval between the 2 doses was
>28 days, the second dose is considered valid.
† Commercial assays can be used to assess disease-induced immunity, but they lack sensitivity to always detect vaccine-induced immunity (i.e., they might
yield false-negative results).
§ For health-care personnel, pregnant women, and immunocompromised persons, birth before 1980 should not be considered evidence of immunity.
¶ Verification of history or diagnosis of typical disease can be provided by any health-care provider (e.g., school or occupational clinic nurse, nurse
practitioner, physician assistant, or physician). For persons reporting a history of, or reporting with, atypical or mild cases, assessment by a physician or their designee
is recommended, and one of the following should be sought: 1) an epidemiologic link to a typical varicella case or to a laboratory-confirmed case or 2)
evidence of laboratory confirmation if it was performed at the time of acute disease. When such documentation is lacking, persons should not be considered as having
a valid history of disease because other diseases might mimic mild atypical varicella.
Advisory Committee on Immunization Practices Varicella Working Group
Chair: Judith R. Campbell, MD, Houston, Texas
Members: Ann M. Arvin, MD, Stanford, California; David W. Kimberlin, MD, Birmingham, Alabama; James L. Hadler, MD, Hartford,
Connecticut; Barbara Watson, MB ChB, Philadelphia, Pennsylvania; Penina Haber, MPH, Atlanta, Georgia; William Atkinson, MD, Atlanta, Georgia; Anne
A. Gershon, MD, New York, New York; Tracy Lieu, MD, Boston, Massachusetts; Teresa Thornton, Des Moines, Iowa; Myron J. Levin, Denver,
Colorado; John F. Modlin, MD, Lebanon, New Hampshire; Dale L. Morse, MD, Albany, New York; Reginald Finger, MD, Colorado Springs, Colorado;
Dalya Guris, MD, Atlanta, Georgia; Mona Marin, MD, Atlanta, Georgia; Sandra S. Chaves, MD, Atlanta, Georgia; Paul Gargiullo, PhD, Atlanta,
Georgia; John W. Glasser, PhD, Atlanta, Georgia; Rafael Harpaz, MD, Atlanta, Georgia; Gregory Wallace, MD, Atlanta, Georgia; Jane F. Seward, MBBS,
Atlanta, Georgia; Scott Schmid, PhD, Atlanta, Georgia; Philip LaRussa, MD, New York, New York; Angela Calugar, MD, Atlanta, Georgia; H. Cody
Meissner, MD, Boston, Massachusetts; Philip R. Krause, MD, Bethesda, Maryland; Keith Powell, MD, Akron, Ohio; Gustavo H. Dayan, MD, Atlanta, Georgia.
Advisory Committee on Immunization Practices
Membership List, June 2006
Chairman: Jon Abramson, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
Executive Secretary: Larry Pickering, MD, CDC, Atlanta, Georgia.
Members: Ban Mishu Allos, MD, Vanderbilt University School of Medicine, Nashville, Tennessee; Judith Campbell, MD, Baylor College of
Medicine, Houston, Texas; Robert Beck, JD, Consumer Representative, Palmyra, Virginia; Reginald Finger, MD, Focus on the Family, Colorado
Springs, Colorado; Janet Gilsdorf, MD, University of Michigan, Ann Arbor, Michigan; Harry Hull, MD, Minnesota Department of Health, St. Paul,
Minnesota; Tracy Lieu, MD, Harvard Pilgrim Health Care and Harvard Medical School, Boston, Massachusetts; Edgar Marcuse, MD, Children's Hospital
and Regional Medical Center, Seattle, Washington; Dale Morse, MD, New York State Department of Health, Albany, New York; Julia Morita, MD,
Chicago Department of Public Health, Chicago, Illinois; Gregory Poland, MD, Mayo Medical School, Rochester, Minnesota; Patricia Stinchfield,
MSN, Children's Hospitals and Clinics of Minnesota, St. Paul, Minnesota; John J. Treanor, MD, University of Rochester, Rochester, New York;
Robin Womeodu, MD, University Hospital, Memphis, Tennessee.
Ex-Officio Members: James E. Cheek, MD, Indian Health Services, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense,
Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National
Vaccine Program Office, Washington, DC; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD,
National Institutes of Health, Bethesda, Maryland; Kristin Lee Nichol, MD, Department of Veterans Affairs, Minneapolis, Minnesota.
Liaison Representatives: American Academy of Family Physicians, Jonathan Temte, MD, Madison, Wisconsin, and Doug Campos-Outcalt,
MD, Phoenix, Arizona; American Academy of Pediatrics, Keith Powell, MD, Akron, Ohio, and Carol Baker, MD, Houston, Texas; America's
Health Insurance Plans, Andrea Gelzer, MD, Hartford, Connecticut; American College Health Association, James C. Turner, MD, Charlottesville,
Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, MD, Louisville, Kentucky; American College of Physicians, Kathleen M.
Neuzil, MD, Seattle, Washington; American Medical Association, Litjen Tan, PhD, Chicago, Illinois; American Pharmacists Association, Stephan L.
Foster,
PharmD, Memphis, Tennessee; Association of Teachers of Preventive Medicine, W. Paul McKinney, MD, Louisville, Kentucky; Biotechnology
Industry Organization, Clement Lewin, PhD, Cambridge, Massachusetts; Canadian National Advisory Committee on Immunization, Monica Naus,
MD, Vancouver, British Columbia; Healthcare Infection Control Practices Advisory Committee, Steve Gordon, MD, Cleveland, Ohio; Infectious
Diseases Society of America, Samuel L. Katz, MD, Durham, North Carolina; London Department of Health, David Salisbury, MD, London, United
Kingdom; National Association of County and City Health Officials, Nancy Bennett, MD, Rochester, New York, and Jeffrey S. Duchin, MD, Seattle,
Washington; National Coalition for Adult Immunization, David A. Neumann, PhD, Alexandria, Virginia; National Foundation for Infectious Diseases,
William Schaffner, MD, Nashville, Tennessee; National Immunization Council and Child Health Program, Romeo S. Rodriquez, Mexico City, Mexico;
National Medical Association, Patricia Whitley-Williams, MD, New Brunswick, New Jersey; National Vaccine Advisory Committee, Gary Freed,
MD, Swiftwater, Pennsylvania, and Peter Paradiso, PhD, Collegeville, Pennsylvinia; Society for Adolescent Medicine, Amy B. Middleman, MD,
Houston, Texas; Pharmaceutical Research and Manufacturers of America, Damian A. Araga, Swiftwater, Pennsylvania.
Advisory Committee on Immunization Practices
Membership List, June 2005
Chairman: Myron J. Levin, MD, University of Colorado Health Sciences Center, Denver, Colorado.
Executive Secretary: Larry K. Pickering, MD, Senior Advisor to the Director, National Immunization Program, CDC, Atlanta, Georgia.
Members: Jon S. Abramson, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina; Ban Mishu Allos, MD,
Vanderbilt University School of Medicine, Nashville, Tennessee; Guthrie S. Birkhead, MD, New York State Department of Health, Albany, New York;
Judith Campbell, MD, Baylor College of Medicine, Houston, Texas; Reginald Finger, MD, Focus on the Family, Colorado Springs, Colorado; Janet
R. Gilsdorf, MD, University of Michigan, Ann Arbor, Michigan; Tracy Lieu, MD, Harvard Pilgram Healthcare and Harvard Medical School,
Boston, Massachusetts; Edgar K. Marcuse, MD, Children's Hospital and Regional Medical Center, Seattle, Washington; Julie Morita, MD, Chicago
Department of Public Health, Chicago, Illinois; Gregory A. Poland, MD, Mayo Medical School, Rochester, Minnesota; John B. Salamone, National Italian
American Foundation, Washington, D.C.; Patricia, Stinchfield, MS, Children's Hospitals and Clinics, St. Paul, Minnesota; John J. Treanor, MD, University
of Rochester School of Medicine and Dentistry, Rochester, New York; and Robin J. Womeodu, MD, University of Tennessee Health Sciences
Center, Memphis, Tennessee.
Ex-Officio Members: James E. Cheek, MD, Indian Health Service, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense,
Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National
Vaccine Program Office, Washington, DC; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD,
National Institutes of Health, Bethesda, Maryland; Norman Baylor, PhD, Office of Vaccines Research Review, Rockville, Maryland; Kristin Lee Nichol,
MD, Department of Veterans Affairs, Minneapolis, Minnesota.
Liaison Representatives: Jonathan Temte, MD, Madison, Wisconsin, Richard D. Clover, MD, Louisville, Kentucky, American Academy of
Family Physicians; Margaret Rennels, MD, Baltimore, Maryland, Carol Baker, MD, Houston, Texas, American Academy of Pediatrics; Andrea Gelzer,
MD, Hartford, Connecticut, America's Health Insurance Plans; James C. Turner, MD, Charlottesville, Virginia, American College Health
Association; Stanley Gall, MD, Louisville, Kentucky, American College of Obstetricians and Gynecologists; Kathleen M. Neuzil, MD, Seattle,
Washington, American College of Physicians; Litjen Tan, PhD, Chicago, Illinois, American Medical Association; Stephan L. Foster, PharmD, Memphis,
Tennessee, American Pharmacists Association; W. Paul McKinney, MD, Louisville, Kentucky, Association of Teachers of Preventive Medicine; Clement
Lewin, PhD, Orange, Connecticut, Biotechnology Industry Organization; Monika Naus, MD, Vancouver, British Columbia, Canada, Canadian
National Advisory Committee on Immunization; Steve Gordon, MD, Cleveland, Ohio, Healthcare Infection Control Practices Advisory Committee, Samuel
L. Katz, MD, Durham, North Carolina, and William Schaffner, MD, Nashville, Tennessee, Infectious Diseases Society of America; David M.
Salisbury, MD, London, United Kingdom, London Department of Health; Nancy Bennett, MD, Rochester, New York, National Association of County and
City Health Officials; David A. Neumann, PhD, Alexandria, Virginia, National Coalition for Adult Immunization; Romeo Rodriguez, Mexico City,
Mexico, National Immunization Council and Child Health Program; Dennis A. Brooks, MD, Baltimore, Maryland, National Medical Association;
Charles Helms, MD, Iowa City, Iowa, National Vaccine Advisory Committee; Amy B. Middleman, MD, Houston, Texas, Society for Adolescent
Medicine; Damian A. Braga, MBA, Swiftwater, Pennsylvania, Peter Paradiso, PhD, Collegeville, Pennsylvania, Pharmaceutical Research and Manufacturers
of America.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.