 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Linking Better Surveillance to Better OutcomesSeth L. Foldy
Corresponding author: Seth L. Foldy, 3061 N. Marietta Avenue, Milwaukee, WI 53211. Telephone: 414-906-0036; Fax: 414-906-9667; E-mail: sfoldy@sbcglobal.net. AbstractSyndromic surveillance aspires to achieve rapid outbreak detection and response, but stand-alone systems not integrated into local business processes might fail to offer better health outcomes. To describe how surveillance can most directly serve action, the author presents a model of local public health work as a series of outcome-driven business processes consisting of information input, information processing, actions, and outcomes. This report derives lessons for improving each of these elements from public health emergencies occurring in Milwaukee, Wisconsin. Lessons for improving input include 1) creatively mining internal or readily accessible information; 2) integrating information flow into routine business practices before an emergency; 3) reusing information in multiple business processes, and ensuring that information-management systems enable such recycling; 4) fostering relationships with information providers by reducing burdens and meeting their needs; and 5) using agile tools to focus surveillance on pressing problems. Lessons for better processing include 1) combining diverse information in well-organized visual displays ("surveillance dashboards"); 2) creating alerts that warn of unusual patterns; 3) using Internet tools to view and share information on demand; 4) using diverse expertise to interpret complex information; 5) assembling surveillance so as to be scalable (from local to global); and 6) ensuring sufficient environmental, laboratory, and clinical capacity for rapid confirmation and response. Lessons for linking surveillance to more efficient action include 1) building surveillance directly into response plans; 2) feeding surveillance information directly into response systems; and 3) employing those information and communications systems used in daily practice to the greatest extent possible. Using surveillance information systematically in outcome-driven business processes can improve emergency response while building day-to-day organizational effectiveness. IntroductionPublic health surveillance has been defined as "the ongoing collection, analysis, interpretation, and dissemination of data regarding a health-related event for use in public health action to reduce morbidity and mortality and to improve health" (1). The primary goal of surveillance is to support action. Because surveillance of established diagnoses might be too slow or insensitive to initiate timely countermeasures, the threats of biologic terrorism and emerging infections (e.g., severe acute respiratory syndrome [SARS]) have spurred interest in syndromic surveillance of near real-time illness indicators (e.g., chief complaints, laboratory test orders, and absenteeism). In addition to its new relevance for homeland security, syndromic surveillance or case management has been used to track influenza, polio, and sexually transmitted diseases for which laboratory confirmation is impractical (2--4). Excellent criteria have been proposed for determining whether syndromic surveillance systems provide reliable, useful information to decision-makers. (5). Different considerations are required to determine whether a system facilitates rapid, effective action, whether a system can be sustained, and whether it will be used in an actual emergency. Answers depend on how well surveillance is integrated into the day-to-day work of local public health agencies (LPHAs). Local professionals are best situated to validate a suspected threat (by rapid assessment of local health-care, environmental, and laboratory information); define the evolving direction of the threat and who is at risk (by interpreting local information on place, time, occupation, and environmental conditions); notify and mobilize the most immediately affected parties; and offer timely, locally relevant risk communications. State and federal resources can help but cannot supplant local knowledge and relationships. LPHAs are typically small but complex organizations working simultaneously on multiple desired community outcomes (e.g., improvements in infant nutrition, food safety, tobacco use, elder quality-of-life, or communicable disease). Work toward each outcome can be viewed as a series of business processes (Figure 1) in which information input (e.g., a referral, an inspection, a survey, a client assessment, or a disease report) is processed to reach an action decision. Actions (e.g., issuing a WIC coupon, a sanitation order, a citation for tobacco sales to minors, or an isolation order; conducting a home visit; or writing a prescription) aim to improve a population outcome. A community that tracks outcomes (e.g., teenage smoking rates) quantitatively also uses this information as input, creating a feedback loop to adjust the type, quality, or quantity of actions. An efficient organization will apply one piece of information to multiple business processes. For example, a patient address received in a disease report can be used to dispatch an investigator, locate household contacts, issue an isolation order, and map an outbreak. This idealized, informatic view of public health emphasizes the importance of considering how information is most effectively converted into action. Too often, information collection is emphasized over information use. Poorly processed information produces information glut and unread reports. Particularly when all staff are responding to an emergency, surveillance information must feed multiple action processes simultaneously (e.g., case finding, specimen collection, laboratory reporting, outbreak characterization [person-place-time patterns], isolation and quarantine, environmental surety, and risk communications). Various public health emergencies helped the Milwaukee (Wisconsin) Health Department (MHD) learn to integrate surveillance into well-organized business processes serving both emergency and everyday functions. This report describes these experiences and summarizes lessons that can help improve syndromic surveillance systems. Linking Surveillance to Outcomes --- Local ExperienceIn 1993, approximately 400,000 Milwaukee-area residents were sickened by a waterborne outbreak of cryptosporidiosis, a then-emerging disease for which reporting was not mandated and testing rarely performed. Although drinking water turbidity levels increased 10 days before reported onset of symptoms, the outbreak was recognized only after shortages of diarrhea medications and enteric culture media were reported (6). At the time, different agencies held information (e.g., on water turbidity, customer complaints, and employee or student absenteeism) that, viewed together, might have alerted authorities to the outbreak earlier. After the outbreak, MHD initiated surveillance of water quality, pharmacy sales, and diarrhea in nursing facilities. Fourteen LPHAs in Milwaukee County established a single disease-reporting site (SurvNet) to simplify reporting, improve outbreak recognition, and increase communication and feedback regarding public health trends to clinicians and laboratories (data reporters). An interagency task force was formed to monitor and improve water quality and to compile and interpret all available information when concerns arose. MHD upgraded clinical and environmental microbiology capabilities and established fax-broadcast and Internet-based communication with laboratories, physicians, infection-control practitioners, and emergency departments (EDs). Debriefings held after each outbreak identified needed changes in policy or procedures. MHD adopted a community outcome goal of 20 reportable enteric infections/100,000 residents (adapted from Healthy People 2010 goal 10-1) (7). These improvements helped speed effective response in 2000 when a nurse contacted SurvNet about four children from three health jurisdictions who had suspected but unconfirmed Escherichia coli O157:H7 infection. Patient interviews identified a restaurant, which was rapidly inspected and closed. Broadcasts to clinicians and laboratories provided diagnostic, treatment, and prevention advice and resulted in rapid identification of additional cases. Evidence from rapidly performed epidemiologic, environmental, and laboratory investigations demonstrated conclusively that processing of contaminated whole-beef cuts could cause sustained disease transmission in restaurants, which helped change national food policy (8). In this instance, one telephone call arising from clinical suspicion triggered rapid action and comprehensive investigation and contributed to health-policy change. Each such success increases interest and confidence in public health surveillance among clinicians and other reporters of public health information. The health effects of a 1995 Milwaukee heat wave were recognized belatedly after the medical examiner was overwhelmed by investigations of heat-related deaths (9). An extreme-heat plan was created, under which action is triggered by an environmental signal (weather forecast) and further accelerated if heat illness is observed by emergency medical services (EMS) or the medical examiner (10). MHD uses communications tools developed for outbreaks to alert multiple human service agencies to take planned action to protect those at greatest risk (9,11). The plan is updated annually and available continuously online. Heat-adjusted morbidity and mortality were reduced by 50% during a 1999 heat wave, compared with 1995 (12). In 1999, local hospitals established EMSystem,® a regional emergency medicine Internet (REMI) application that enables EDs to communicate when they must divert ambulances. When too many EDs simultaneously signal diversion, the paramedic system overrides diversion, generating an e-mail/text-page alert. In January 2000, REMI data were used to track influenza- related ED congestion, and a Health Care Capacity Alert Committee was formed (including public health, EMS, medical, and hospital representatives) to issue recommendations to ease ED crowding (13). In fall 2000, an unusual volume of diversion-override text pages alerted MHD to severe ED congestion, months before influenza season. Review of REMI data indicated that congestion was primarily attributable to inpatient bed shortages. Committee recommendations to adjust vacation leave, facilitate timely discharge, and control elective admissions were followed in 2 days by a rapid decline in ED diversions. REMI data were later used to justify a regulatory waiver permitting medical/surgical use of rehabilitation and psychiatric beds during the 2000--01 influenza season. REMI provided unexpected but useful surveillance information on health-care utilization and capacity that, linked to action, helped build stronger relationships between public health professionals and health-care providers. MHD adapted REMI in 2000 for heat-illness surveillance during heat waves and in 2002 for short-term surveillance of biologic terrorism syndromes during international-profile sporting events (14). This helped MHD establish multi-ED surveillance for SARS 3 days after CDC urgently requested surveillance in 2003. After successful deployment in Milwaukee, the SARS screening form was downloaded for use by hundreds of clinicians. Because the REMI application was then used in >25 cities, SARS surveillance was offered to other jurisdictions; 27 EDs reported surveillance of >146,500 visits to LPHAs in four states, and CDC staff were able to download these data for aberration analysis. REMI permitted agile deployment of a new syndromic surveillance system across widely distributed jurisdictions (15). In summer 2003, SurvNet received a report of a febrile blister illness in an animal dealer associated with sick prairie dogs. Wisconsin authorities linked this report to a similar case elsewhere in the state, triggering immediate trace-forward and trace-back investigation of animal sales. The illness was subsequently diagnosed as the hemisphere's first outbreak of monkeypox. Action to protect the public began before diagnosis. However, lack of interoperable data systems impeded information-sharing among the many health and veterinary agencies involved across multiple states. Lessons Learned --- Linking Better Surveillance to Better Action and OutcomesThese experiences indicated that 1) more syndromic information (input) is available than typically used, 2) information processing can improve the timeliness and quality of decision-making, and 3) action can be accelerated by good information-management practices. Recommendations follow for better integrating surveillance information into each of these business process steps (input, processing, and action). Improving the InputLPHAs can easily increase the type, quality, and sustainability of surveillance by 1) mining information from daily business processes found within or near the organization; 2) integrating information flow into routine business practices before an emergency; 3) reusing information in multiple business processes, and ensuring that information-management systems enable such recycling; 4) fostering relationships with information providers by reducing burdens and meeting their needs; and 5) using agile tools to focus surveillance on pressing problems. Within local agencies, diverse information streams on symptoms, environmental conditions (e.g., heat, water quality, and animal illness), health-care utilization (e.g., prescriptions, laboratory orders, ambulance diversion, and 911 dispatch calls), and behaviors (e.g., absenteeism or travel) are often readily available. Internal information sources might be as useful as more elaborate data gathering (e.g., MHD uses routine food-safety inspections to track the number of restaurants permitting smoking). Other local entities (e.g., the water utility or fire/EMS) also possess important, readily available information. Finally, the Milwaukee examples illustrate how environmental, health-care utilization, and other types of data can provide earlier warning or more robust validation of problems than clinical signs and symptoms alone. For surveillance of waterborne Cryptosporidium, heat-related illness, and monkeypox, environmental information provided longer alert lead-times than clinical findings. Although syndromic surveillance is often inspired by emergencies, an emergency is not the best time to begin work with unfamiliar information. Without daily practice, systems can fall into disuse and might complicate emergency response as much as facilitate it. Ideally, surveillance systems are both derived from and support daily local public health operations, thereby strengthening relationships and communications, which become even more critical during emergencies. The health agency that uses every datum for multiple purposes can improve alertness and effectiveness at minimal cost. Ideally, information is "entered once, used often," instead of being locked inside applications and unavailable for reuse. Various Internet applications collect information but do not permit local analysis of entered data. Internet-served applications also often fail to permit uploading of information from a local agency's own information-management system. This results in duplicate entry, poorer data quality, and difficulty using or reusing information efficiently or creatively. These considerations support the argument for full and rapid implementation of CDC's Public Health Information Network (PHIN) (16) vision of interoperable applications that truly exchange rather than hoard health information. The quality and quantity of surveillance information relies on the willingness of busy people to provide it. One way to improve surveillance is to make it less burdensome. Combining disease reporting for 14 jurisdictions in SurvNet made reporting easier, while also increasing the surveillance catchment area and exploiting economies of scale for more sophisticated data management. Calling one reporting site often instead of 14 infrequently helped infection-control professionals build relationships with SurvNet staff; such relationships can increase willingness to share observations of uncertain significance that enhance recognition of unusual outbreaks (e.g., monkeypox). However, such relationships are less likely within an office covering 300 jurisdictions; therefore, appropriate local scale remains important. Another way to minimize reporting burden is to use those communications tools already used by health professionals in their own day-to-day work (e.g., REMI) rather than expect busy professionals to log onto stand-alone public health utilities (e.g., certain health alert networks). Eliminating altogether the need for conscious effort in reporting is the goal of such surveillance initiatives as electronic laboratory reporting and secondary mining of health-information-management systems. However, engaging health providers in well-designed surveillance activities has other benefits. The SARS screening form was designed to trigger infection-control protection as well as to alert public health. Its use was also reported by ED managers to improve clinicians' index of suspicion. Providers are most likely to comply with surveillance when it aids them in activities on which they place high value, such as improving diagnosis. MHD attempts to issue timely situational alerts to cue clinicians to problems they might see in their practices (e.g., heat-related illness during a heat wave, biologic agents such as anthrax after September 11, 2001, or E. coli infection during an outbreak). Such alerts help focus surveillance while also helping clinicians appreciate that surveillance provides, as well as demands, useful information. Providing timely information that helps providers defend themselves from infection (e.g., SARS), send the right test, or offer special resources for affected patients also helps improve awareness of the benefits of surveillance. Finally, providers enjoy learning how surveillance contributes to healthy public policies, not just to tables and graphs. In a rapidly changing world, surveillance should be flexible enough to focus on the most immediate threat, based on warnings as diverse as weather forecasts, law-enforcement or international intelligence, global disease trends, or nearby outbreaks. This flexibility requires agile tools for surveillance. Agility is especially important for unexpected emerging diseases (e.g., SARS or monkeypox). Milwaukee EDs have become accustomed to implementing temporary surveillance by using REMI; the threat of the day might change, but the system used remains familiar. Networks of providers or laboratories already engaged in one surveillance system (e.g., for influenza-like illness) might also be amenable to participating in emergency surveillance for other agents, providing another source of agile surveillance. Improving ProcessingSurveillance information must be processed in a timely, meaningful way for providers to be guided by knowledge instead of overwhelmed with data. Effective processing is aided by 1) combining diverse information in well-organized visual displays ("surveillance dashboards"); 2) creating alerts that warn of unusual patterns; 3) using secure Internet sites to view and share information on demand; 4) using diverse expertise to interpret complex information; 5) assembling surveillance so as to be scalable (from local to global); and 6) ensuring sufficient environmental, laboratory, and clinical capacity for confirmation and response. Each different surveillance information stream provides only a fragmentary view of a complex world. The cryptosporidiosis outbreak illustrated how assembling and comparing different types of existing information might be more important than collecting new information. Fragmented views occur not only between organizations but just as often within a single agency. Until recently, different MHD units produced or received statistics on pneumonia and influenza deaths, influenza-like illness, and influenza laboratory cultures, but the agency had no single coherent view of respiratory illness. Creating a single visual display of all three types of data on a common time axis and mounting it on the Internet enabled MHD to transform little-used data into rich knowledge for multiple users, accessible on demand, day or night (Figure 2). Sharing different expertise might be as important as sharing different information. Milwaukee's Health Care Capacity Alert Committee and Water-Health Taskforce are multidisciplinary, multiagency groups that interpret and act on complex information. The Taskforce meets monthly for other tasks, which keeps it functioning smoothly, and convenes in response to unusual information or situations. Scale is important, but optimum scale varies from one situation to another. Milwaukee's SurvNet one-stop reporting system speeds detection of and response to outbreaks that cross local jurisdictional boundaries, but the system might not recognize rare events if implemented statewide. The capacity to build scalable surveillance across regions and states is enhanced by the growth of managed care networks, multiregional REMI systems, multistate surveillance systems (e.g., FoodNet), and the interoperable information environment promised by PHIN. Combined with automated tools (e.g., SaTScan™ (17) analysis) to test the significance of events over variable geographic and temporal scales, potential flexibility in the scale of surveillance might approach infinity. However, more often than not, local insight is needed to interpret local surveillance information intelligently, which is why national and international surveillance systems will only be as strong as their local building blocks. Confirmation (and control) of suspected events relies heavily on well-prepared clinical, laboratory, and environmental expertise. Unless these local capabilities are in place and integrated for rapid response, even the best and earliest surveillance alert will fail to generate timely effective action. Faster, Surer ActionBetter information inputs and processing matter only when they lead to effective action. Effectiveness can be improved by 1) building surveillance directly into response plans; 2) feeding surveillance information directly into emergency response systems; and 3) employing information and communication systems used for everyday practice to the greatest extent possible. Considerable time and effort can be saved when enhanced surveillance systems are specifically referenced in emergency plans. For example, certain types of health, environmental, or intelligence data automatically trigger higher stages of readiness in Milwaukee emergency response plans. Ideally, information from surveillance systems can directly feed information systems used for emergency response. For example, if a cluster of persons with febrile vesicular rash is detected, the next steps (investigation, laboratory diagnosis, isolation, and contact tracing) each require similar information, including names, addresses, clinical information, employers, travel, and contacts. Downloading such data from surveillance systems directly into the line lists used for outbreak investigation would reduce work and improve data quality in a rapidly evolving emergency. Emergencies are not optimal times to learn how to use unfamiliar information systems. To the extent possible, surveillance and communications with community partners should employ the same systems they use everyday, as close to the point-of-service as possible. This again emphasizes the need for information exchange between the systems used routinely in clinical and public health settings, rather than forcing users to switch to new systems. ConclusionPublic health's primary role goes beyond preparing for intermittent emergencies to reducing the leading causes of death, illness, and injury. If increased public health funding for homeland security is short-lived, resulting surveillance systems will be most sustainable if they also address long-term, common problems as well as extraordinary ones. Health departments that set quantifiable community outcome goals (e.g., to reduce enteric disease or smoking rates) place surveillance at the core of all work, not just communicable disease control. Syndromic and other surveillance systems that become an integral part of day-to-day business processes become indispensable. They don't just detect problems but also measure successes and identify what works. This doubles the value and sustainability of any surveillance system. Acknowledgments A partial list of those contributing to cited Milwaukee-area innovations includes Kathleen Blair, Paul Biedrzycki, Geoffrey Swain, CapriMara Fillmore, Douglas Gieryn, Susan Schultz, Sandy Coffaro, Marion Lee, Donna Rowe, Mary Ellen Bruesch, Alki Burdett, Jeffrey Davis, Edward Barthell, Kim Pemble, Nancy Healy-Haney, and the health officers of suburban Milwaukee County. References
Figure 1 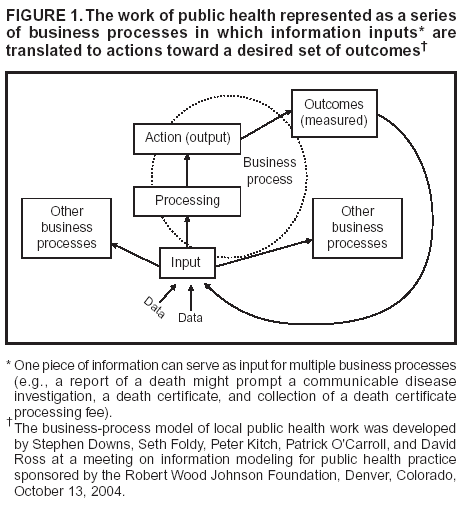 Return to top. Figure 2 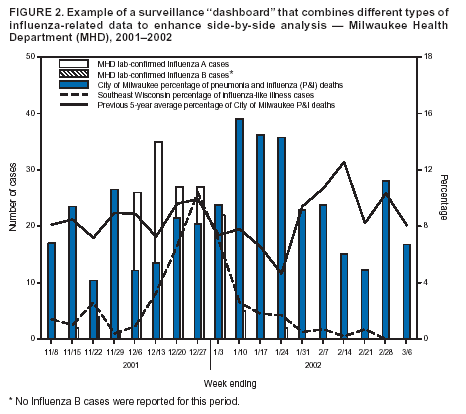 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/14/2004 |
|||||||||
This page last reviewed 9/14/2004
|