|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
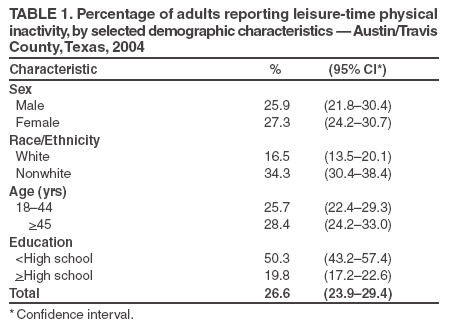
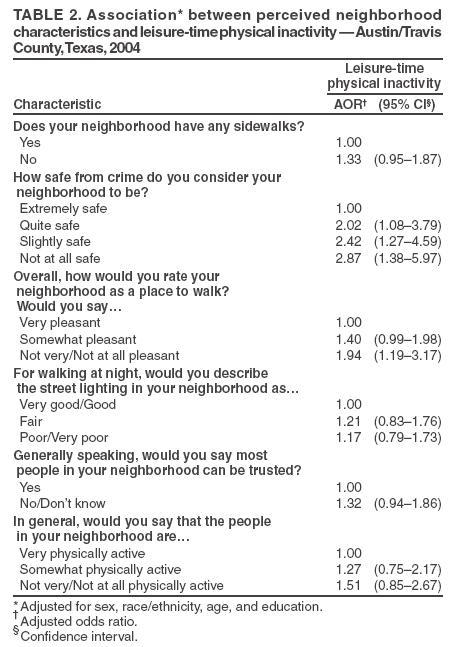
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Perceptions of Neighborhood Characteristics and Leisure-Time Physical Inactivity --- Austin/Travis County, Texas, 2004Regular physical activity improves quality of life and reduces risk for coronary heart disease, colon cancer, hypertension, diabetes, and overall mortality (1). Physical activity also has been associated with reduced symptoms of depression and greater independence (1,2). A sedentary lifestyle is associated with obesity (1,3). However, despite the health benefits of physical activity, 23.1% of adults in the United States report they do not engage in any leisure-time physical activity (4). Neighborhood environment (e.g., sidewalks and street lighting) (5,6), perceived trustworthiness of neighbors (5), and perceptions of neighborhood safety (6,7) all have been associated with levels of physical activity. During 2004, to assess the association between these factors and leisure-time physical inactivity in eastern Travis County, Texas, the local health department collected and analyzed data by using the methodology of the Behavioral Risk Factor Surveillance System (BRFSS). This report describes the results of that analysis, which indicated that persons who perceived their neighborhoods as less than extremely safe were more than twice as likely to have no leisure-time physical activity, and those who perceived their neighborhoods as not at all safe were nearly three times as likely to have no leisure-time physical activity. Public health agencies promoting physical activity in neighborhoods should consider how residents perceive their safety and design programs that specifically address those safety concerns. Austin/Travis County Health and Human Services Department interviewed 1,635 adult residents of eastern Travis County, Texas, by using a random-digit--dialed telephone survey. Applying BRFSS methodologies and core questions, data were collected during a 3-month period in late summer and early fall of 2004. Leisure-time physical inactivity was defined as a response of "no" to the BRFSS core exercise question: "During the past month, other than your regular job, did you participate in any physical activities or exercises such as running, calisthenics, golf, gardening, or walking for exercise?" Self-reported neighborhood environmental characteristics were assessed by using questions from a module added to the 2004 Texas BRFSS. Questions included perceptions of neighborhood safety, presence of sidewalks, adequacy of streetlights, and perceived characteristics of neighbors. For the purposes of the survey, respondents were told that their neighborhoods were defined as the areas within one-half mile or a 10-minute walk from their homes. The survey was conducted as part of the baseline data collection for the Steps to a HealthierUS program in an area of 20 contiguous postal codes in eastern Travis County with an approximate population of 460,000. Data were weighted to reflect the demographic composition of the area. The overall response rate for the survey was 51.8%, determined by using the Council of American Survey Research Organizations method (8). The association between leisure-time physical inactivity and perceived neighborhood characteristics was measured by using adjusted odds ratios (AOR) and 95% confidence intervals (CIs). Odds ratios were obtained by using logistic regression and were adjusted for sex, race/ethnicity (i.e., white non-Hispanic or nonwhite), age, and education level. Overall, 26.6% of those surveyed were physically inactive during their leisure time. No statistically significant differences in prevalence existed by sex or age (Table 1). A higher prevalence of leisure-time physical inactivity was reported among nonwhite respondents (34.3%) than whites (16.5%) and among those with less than a high school education (50.3%), compared with high school graduates (19.8%). After adjustment for sex, race/ethnicity, age, and education, associations were identified between respondent perceptions of the safety and pleasantness of their neighborhoods and their leisure-time physical inactivity. Persons who reported their neighborhood as slightly safe or quite safe were more than twice as likely to report being physically inactive during their leisure time as those reporting their neighborhood as extremely safe; persons who described their neighborhood as not at all safe were nearly three times more likely (AOR = 2.87; CI = 1.38--5.97) to be physically inactive during their leisure time than those describing their neighborhood as extremely safe (Table 2). In addition, persons describing their neighborhood as not very or not at all pleasant for walking were more likely to report leisure-time physical inactivity than persons describing their neighborhood as very pleasant for walking (AOR = 1.94; CI = 1.19--3.17). However, the survey identified no association between leisure-time physical inactivity and the presence of sidewalks, adequacy of street lighting, perceived trustworthiness of neighbors, or perceived level of physical activity within the neighborhood. Reported by: J Vest, MPH, A Valadez, MD, Austin/Travis County Health and Human Svcs Dept, Austin, Texas. Editorial Note:Although previous research has implicated physical neighborhood conditions and other characteristics as determinants of levels of physical activity (6), the findings in this report indicate that perceived safety was the factor with the strongest association with leisure-time physical inactivity. Local public health departments have traditionally worked with law enforcement in programs to eliminate intimate partner violence and to promote traffic, pedestrian, and bicycle safety. These findings suggest that one aspect of the physical inactivity of residents might be addressed by health departments' encouraging and aiding law enforcement in its primary role of ensuring public safety and reducing neighborhood crime. The findings in this report are subject to at least five limitations. First, the study was a cross-sectional survey; therefore, no temporal sequence could be established. Second, the response rate was 51.8%, so these findings might not be generalizable to nonrespondents. Third, all information, including physical activity levels and perceptions of neighborhood safety and other characteristics, was self-reported and not validated by any other means. Fourth, the survey was conducted during months with long hours of daylight, and street lighting might not be valued as highly for physical activity as during months when days are shorter. Finally, questions on adequacy of street lighting and overall pleasantness of the neighborhood both specifically mentioned walking; results might be different if walking was the only physical activity examined or if the two questions were more general. A comprehensive plan to increase physical activity in neighborhoods, such as the Steps to a Healthier Austin program in the Austin/Travis County area, should consider interventions that improve safety and perceptions of safety, in addition to physical improvements (e.g., sidewalks, street lighting, parks, and beautification). Information about that program is available at http://www.healthierus.gov/steps/grantees/austin.html and http://ithriveaustin.org. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/22/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|