|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
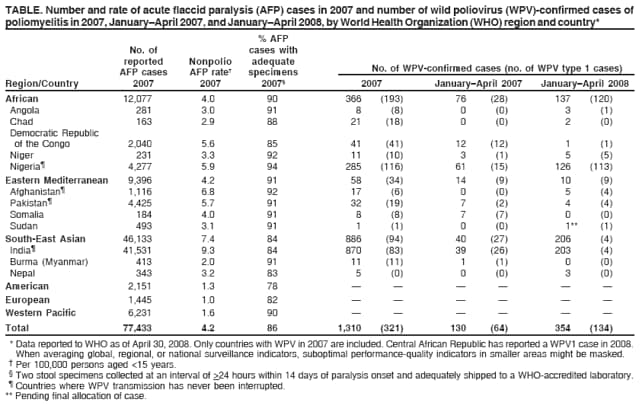
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Interruption of Wild Poliovirus Transmission --- Worldwide, January 2007--April 2008In 1988, the World Health Assembly resolved to eradicate poliomyelitis. Subsequently, the Global Polio Eradication Initiative reduced the global incidence of polio associated with wild polioviruses (WPVs) from an estimated 350,000 cases in 1988 to 1,997 reported cases in 2006 and reduced the number of countries that have never succeeded in interrupting WPV transmission from 125 to four (Afghanistan, India, Nigeria, and Pakistan) (1--4). Type 2 WPV (WPV2) circulation was last observed in October 1999 (5). In February 2007, the World Health Organization (WHO) convened a stakeholders meeting to agree on an accelerated polio-eradication effort to be used during 2007--2008 and establish milestones to monitor progress. Programmatic strategies implemented in 2007 included expanded use of type 1 monovalent oral poliovirus vaccine (OPV) (mOPV1) to eliminate type 1 WPV (WPV1) transmission before type 3 WPV (WPV3)* (6) and targeted use of type 3 monovalent OPV (mOPV3) in selected areas (1--4). This report summarizes these strategies and overall progress toward reaching the milestones, including a decline in the overall number of WPV cases to 1,310 in 2007 and substantial progress toward interruption of WPV1 circulation in India in 2008. Routine OPV VaccinationRoutine vaccination remains an integral component of the polio eradication initiative. Global routine vaccination coverage for infants with 3 doses of trivalent OPV (tOPV) was estimated at 80% in 2006† (7), an increase from 73% in 2001. Estimated coverage varied among WHO regions: 65% in the South-East Asian, 75% in the African, 86% in the Eastern Mediterranean, and >93% in the Western Pacific, European, and Americas regions. In the four polio-endemic countries, 3-dose tOPV coverage was estimated at 77% in Afghanistan, 58% in India, 61% in Nigeria, and 83% in Pakistan; however, substantially lower coverage (<40%) has been reported in subnational areas with ongoing polio transmission (i.e., northern Nigeria and the northern Indian states of Uttar Pradesh and Bihar) (2,3). Supplementary Immunization Activities (SIAs)§ in 2007In 2007, 164 SIAs were conducted in 27 countries (60 national immunization days, 86 subnational immunization days, and 18 mop-up rounds with OPV), using a total of 2.32 billion OPV doses delivered to 400 million children aged <5 years. Use of mOPV1 increased from 22% of all administered SIA doses in 2005 to 46% in 2006 and to 52% in 2007, reflecting the programmatic emphasis on interrupting WPV1 transmission (6). A total of 76 (46%) of the 164 SIAs were conducted in the four polio-endemic countries: 25 in India, 19 in Pakistan, and 16 each in Afghanistan and Nigeria. Of the remaining 88 SIAs, 56 (34% of all SIAs) were conducted in eight countries where WPV was reintroduced through importation,¶ and 32 (20% of all SIAs) were conducted in 15 countries with no WPV-confirmed cases in 2007 in response to earlier outbreaks or as a precaution against poliovirus importations. To improve SIA quality, strategies that were introduced in 2006 in the four polio-endemic countries were continued in 2007. Nigeria continued "immunization-plus days" that offered other vaccines (e.g., measles, hepatitis B, and diphtheria and tetanus toxoids and pertussis vaccines) and health interventions (e.g., bednets and deworming medication) in addition to OPV during SIAs (2). Despite repeated SIAs and because of lower routine vaccination coverage in high-risk areas, the proportion of "zero-dose children"** in 2007 was substantially higher in polio-affected (18%) areas in Nigeria than in polio-free areas (2%). In India, the government maintained intensive large-scale SIAs in districts of Bihar and western Uttar Pradesh with the highest polio risk, primarily using mOPV1 and concentrating on improving coverage among children aged <2 years. The proportion of zero-dose children in India was <1% in both polio-affected areas and polio-free areas. Afghanistan and Pakistan implemented an approach that included improved cross-border synchronization of polio campaigns. In addition, access during SIAs in insecure areas of Afghanistan that previously were inaccessible by vaccinators improved beginning September 2007, after obtaining the support of antigovernment groups; nonetheless, the proportion of zero-dose children overall for 2007 was 9% in those areas. Otherwise, the proportion of zero-dose children was essentially the same in both countries in polio-affected areas (<1%) and polio-free areas (<1%). Acute Flaccid Paralysis (AFP) SurveillanceThe quality of AFP surveillance is monitored by two performance indicators: 1) the rate of AFP cases not caused by WPV (i.e., the nonpolio AFP rate; target for certification: more than one case per 100,000 persons aged <15 years), and 2) the proportion of AFP cases with adequate stool specimens†† (target for certification: >80%). In 2007, each WHO region maintained sensitivity of AFP surveillance to detect paralytic polio cases at certification-standard levels (Table). Globally, AFP case reporting increased 13%, from 68,519 cases in 2006 to 77,433 cases in 2007, primarily as a result of increased reporting from India. Since 2005, a target reporting rate for all polio-endemic countries and countries at high risk for WPV importation has been more than two nonpolio AFP cases per 100,000 persons aged <15 years (8). In 2007, all four polio-endemic countries and the eight countries with cases reported in 2007 (because of reintroduced WPV) reached this target rate. Global Polio Laboratory NetworkIn 2007, WHO accredited 98% of the 145 global poliovirus network laboratories, which together analyzed approximately 157,000 stool specimens from persons with AFP. In addition, the laboratory network finalized implementation of a testing approach in countries of WHO regions with WPV circulation that reduces poliovirus confirmation time by 50% (to 21 days), compared with previous methods.§§ The percentage of stool specimens tested from polio-endemic regions in laboratories with capacity for both virus isolation in cell culture and differentiation of wild or vaccine-like viruses increased from 57% in 2006 to 69% in 2007. WPV IncidenceAs of April 30, 2008, a total of 1,310 polio cases with onset of paralysis in 2007 had been reported worldwide (Table), a decrease of 34% from the 1,997 cases reported in 2006. With the strategic emphasis on WPV1 elimination, WPV1 cases decreased 81% from 1,666 in 2006 to 321 cases in 2007; however, WPV3 cases tripled from 331 in 2006 to 989 in 2007 (Figure 1). The reported number of polio-affected districts in all countries decreased 26% from 463 in 2006 to 342 in 2007. A total of 106 (8%) cases in 2007 were in countries where WPV was reintroduced through importation, compared with 1,301 (40%) of 3,234 cases during 2004--2005 (9). As of April 30, a total of 134 WPV1 cases and 220 WPV3 cases with onset of paralysis in 2008 had been reported (Figure 2), compared with 64 WPV1 cases and 66 WPV3 cases reported during the same period in 2007. India. Reported WPV1 cases declined 87% in India, from 646 in 2006 to 83 in 2007, associated with expanded use of mOPV1 (3). Western Uttar Pradesh, which had been the primary reservoir of WPV1 circulation in recent years, reported five WPV1 cases in 2007. The number of WPV1-affected districts declined 61%, from 114 in 2006 to 45 in 2007. However, a WPV3 outbreak involving Uttar Pradesh and spreading to Bihar resulted in an increase in WPV3 cases from 28 in 2006 to 787 in 2007; the number of WPV3-affected districts increased from seven in 2006 to 77 in 2007. Primary use of mOPV1 in SIAs during 2006--2008 has accelerated the decline in WPV1 cases; as of April 30, 2008, only four cases had been reported in 2008 (in New Delhi, Orissa, Bihar, and West Bengal), compared with 26 cases during the same period in 2007. Monthly reported WPV3 cases decreased from a peak of 216 cases in December 2007 to 32 cases in March 2008; nonetheless, 199 cases of WPV3 had been reported in 2008, primarily in Bihar, compared with 13 during the same period in 2007. Nigeria. Reported WPV1 cases declined 86% in Nigeria, from 843 in 2006 to 116 in 2007, and reported WPV3 cases declined 39%, from 277 in 2006 to 169 in 2007. The number of WPV1-affected districts declined 62%, from 203 in 2006 to 78 in 2007. The number of WPV3-affected districts declined 14%, from 125 in 2006 to 108 in 2007; however, WPV3 outbreaks and isolated cases occurred in districts in certain previously polio-free southern states. As of April 30, 2008, a total of 113 WPV1 cases and 13 WPV3 cases with onset in 2008 had been reported, compared with 15 WPV1 cases and 46 WPV3 cases reported for the same period in 2007. Pakistan and Afghanistan. WPV circulates between Pakistan and Afghanistan. WPV1 cases decreased in Pakistan, from 20 in 2006 to 19 in 2007, whereas WPV3 cases decreased 35%, from 20 in 2006 to 13 in 2007. Twelve districts were affected with WPV1 in both 2006 and 2007, whereas the number of WPV3-affected districts declined 36%, from 14 in 2006 to nine in 2007. Transmission has remained confined to two known virus reservoirs along the Pakistan-Afghanistan border, with the southern reservoir extending well into nonborder districts in southern Pakistan provinces (4). By April 30, 2008, four WPV1 cases with onset in 2008 had been reported in Pakistan, compared with two WPV1 and five WPV3 cases during the same period in 2007. Although access during SIAs in Afghanistan did not improve until late in 2007 in the areas with security problems, the number of WPV1 cases decreased 79%, from 29 cases in 2006 to six in 2007; however, the number of WPV3 cases increased from two cases in 2006 to 11 in 2007 (4). WPV1 and WPV3 transmission continued in the Southern Region, and two cases of WPV1 were reported in the Eastern Region in areas bordering Pakistan. The number of WPV1-affected districts decreased 65%, from 17 in 2006 to six in 2007, whereas the number of WPV3-affected districts increased from two in 2006 to nine in 2007 (4). As of April 30, 2008, four WPV1 cases and one WPV3 case with onset in 2008 had been reported in Afghanistan, compared with no WPV cases during the same period in 2007. Other countries. Thirteen countries, once polio-free, reported WPV cases in 2006 following WPV importation¶¶; six of these countries reported polio cases in 2007 (Angola, Chad, Democratic Republic of the Congo [DRC], Nepal, Niger, and Somalia).*** In Angola and DRC, transmission in 2007 (with eight and 41 cases, respectively) followed importation of WPV1 originating in India; as of April 30, 2008, Angola and DRC each had reported one WPV1 case in 2008, compared with no cases and 12 cases, respectively, during the same period in 2007. In addition, two WPV3 cases were identified in Angola in 2008, both with onset in March, also genetically indicating origin in India. In Chad, circulation of WPV1 (18 cases) and WPV3 (three cases) in 2007 continued after introduction from Nigeria in past years and 2007. In Niger, with a total of 10 WPV1 cases and one WPV3 case, certain importations from neighboring Nigeria resulted in clusters of cases from internal transmission. As of April 30, 2008, two WPV3 cases had been reported in 2008 from Chad and five WPV1 cases from Niger.††† Nepal, bordering India, had five sporadic WPV3 importations in 2007; as of April 30, 2008, three WPV3 cases had been reported in Nepal in 2008. Somalia reported eight WPV1 cases in 2007 but has had >1 year without detection of cases after an outbreak during July 2005--March 2007. After several years without polio, Burma (Myanmar) had an outbreak of 11 WPV1 cases in 2007, with the last reported case occurring in May. Sudan, which had no reported polio cases in 2006, reported a single confirmed case of WPV1 circulating in Chad. However, as of April 30, 2008, a case with onset in February 2008 occurred on the Sudan-Ethiopia border; the exact location is under investigation. Genomic sequencing analysis indicates years of undetected WPV1 chains of transmission within Sudan, western Ethiopia, or both; the closest genetic relationship is with WPV1 isolated from a patient in Sudan in 2004. Reported by: Polio Eradication Dept, World Health Organization, Geneva, Switzerland. Div of Viral Diseases and Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:In 2007, substantial progress was made toward limiting the geographic extent and number of cases of WPV1 transmission in India as a result of intensive SIAs with increased use of mOPV1 in affected areas. However, WPV3 transmission increased in Uttar Pradesh and Bihar because of the intended focus on elimination of WPV1, limited mOPV3 supply in India, restricted tOPV use in SIAs in 2007, and underlying insufficient routine vaccination coverage (3). Combined use of mOPV1, mOPV3, and tOPV is expected to lead to interruption of WPV1 transmission and a substantial decrease in WPV3 transmission in India by the end of 2008. WPV1 cases and affected districts also decreased substantially in Nigeria during 2007, compared with 2006. However, this decrease has not been sustained; more WPV1 cases have occurred in 2008 than during the same period in 2007. The proportion of children entirely missed during SIAs and routine vaccinations remains high (>10%) in certain states in Nigeria. Major efforts to strengthen routine vaccination services and the quality of SIA implementation are continuing (2). The number of confirmed WPV1 cases decreased nearly 80% in Afghanistan but has not substantially decreased in Pakistan; security and access problems in border areas of Afghanistan and Pakistan are continuing, but improved access (compared with early 2007) in Afghanistan and continuing coordinated cross-border vaccination efforts might produce better results in 2008. Operational problems in vaccinating children in secure areas of Pakistan also are being addressed (4). The WHO stakeholders meeting in February 2007 established three milestones for the end of 2007 (6). The first milestone was to reduce the number of affected districts in the four polio-endemic countries by >50% compared with 2006. A 59% reduction in WPV1-affected districts has occurred, but WPV3-affected districts have increased 37% (for a net 24% reduction in WPV-affected districts). The second milestone, reducing the proportion of zero-dose children in polio-affected areas to less than that in polio-free areas, has been met in India and major portions of affected areas in Afghanistan and Pakistan. However, this milestone has not been achieved in the high-risk areas of Nigeria and Afghanistan. The third milestone involves interrupting transmission in all 13 countries with polio cases resulting from imported WPV in 2006. WPV transmission continued in Chad and DRC through 2007 and into 2008. New cases and transmission were reported in Angola and Niger during 2007, and Nepal experienced repeated WPV3 importations in 2007. However, Sudan or western Ethiopia, or both, have had longstanding WPV1 circulation since importation of WPV of Nigerian origin into Sudan in 2004 (9) without detection during 2006--2007, which indicates that surveillance quality should be monitored within each country by subnational area and strengthened where needed. Ongoing WPV transmission in Angola, Chad, DRC, and Sudan and/or Ethiopia requires continuing efforts to overcome the operational impediments limiting the vaccination of children. The technical feasibility of polio eradication has been demonstrated repeatedly by the ability to interrupt WPV transmission in some of the most difficult to access and insecure areas in the world, including areas that have limited health infrastructure, such as Somalia. In 2007, the feasibility of polio eradication was highlighted by the substantial progress toward WPV1 interruption in India. The concerted effort to interrupt WPV1 transmission worldwide continues in 2008, with a focus on administering mOPV1 in SIAs, combined with periodic use of mOPV3 and tOPV. Sustained commitment by governments and international partners with ongoing program evaluation and adaptation to changing circumstances is crucial for progress to continue. References
* WPV1 is more likely to cause paralytic disease and have a wide geographic spread than WPV3. † Most recent year for which data are available; WHO/UNICEF estimates. § Mass campaigns conducted during a brief period (days to weeks) in which 1 dose of OPV is administered to all children aged <5 years, regardless of vaccination history. ¶ Angola, Chad, Democratic Republic of the Congo, Burma (Myanmar), Nepal, Niger, Somalia, and Sudan. ** Children aged 6--35 months with nonpolio acute flaccid paralysis who had never been vaccinated with OPV, according to vaccination histories provided by their mothers. †† Two specimens collected >24 hours apart, both within 14 days of paralysis onset, and shipped on ice or frozen ice packs to a WHO-accredited laboratory, arriving at the laboratory in good condition. §§ Additional information available at http://www.who.int/immunization_monitoring/Supplement_polio_lab_manual.pdf. ¶¶ Angola, Bangladesh, Chad, Democratic Republic of the Congo, Ethiopia, Indonesia, Kenya, Namibia, Nepal, Niger, Somalia, Sudan, and Yemen. *** As determined by genetic lineage, 33 of 35 separate importations have been stopped (defined as lack of detection of related WPV cases since September 30, 2007) in 11 of the 13 countries; transmission of imported poliovirus lineages circulating in 2006 continues in Chad and Democratic Republic of the Congo. ††† Additionally, Central African Republic, last reporting WPV1 in 2004 (9), has identified a WPV1 case in the capital, Bangui, with onset in April 2008.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 5/8/2008 |
|||||||||
|