 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Racial and Socioeconomic Disparities in Breastfeeding --- United States, 2004The American Academy of Pediatrics recommends breastfeeding for at least the first year of life, and beyond for as long as mutually desired by mother and child (1). Not breastfeeding is associated with increased health risks for children, including otitis media, respiratory tract infections, diarrhea, and necrotizing enterocolitis (1,2). In addition, breastfeeding duration is inversely associated with risk for childhood overweight (3). Breastfeeding also is associated with health benefits for mothers, including reduced risk for ovarian cancer and premenopausal breast cancer (1,2). Breastfeeding rates differ substantially by race, socioeconomic level, and other demographic factors (4). For example, among children born during 1982--1993, non-Hispanic black children were less likely than non-Hispanic white children to be breastfed at birth and at age 6 months, even when comparisons were among children in the same socioeconomic or other demographic subgroup (4). To obtain current estimates of racial and economic disparities in breastfeeding among U.S. children, CDC analyzed data from the 2004 National Immunization Survey (NIS). This report describes the results of that analysis, which indicated that 71.5% of non-Hispanic white children were ever breastfed compared with 50.1% of non-Hispanic black children. Among those ever breastfed, 53.9% of non-Hispanic white and 43.2% of non-Hispanic black children continued breastfeeding until at least age 6 months. Disparities between black and white children existed within most socioeconomic subgroups studied. Public health programs should continue to promote breastfeeding initiation and increase support of breastfeeding continuation, especially among subgroups with the lowest rates (i.e., black, poor, and young mothers; mothers with less than a high school education; and mothers residing in rural areas). CDC conducts the NIS annually to obtain national, state, and selected urban-area estimates of vaccination rates among children (5,6). The NIS uses random-digit dialing to survey households with children aged 19--35 months at the time of the telephone interview; thus, the 2004 NIS represents children born from February 2001 through May 2003. Interviews are conducted via telephone with the household member most knowledgeable about the child's vaccination history and collect data about the child, mother, and household. The survey is designed to collect nationally representative data on the noninstitutionalized U.S. civilian population. From the last quarter of 2001 through 2005, the NIS included the following questions on breastfeeding: "Was [child's name] ever breastfed or fed breast milk?" and "How long was [child's name] breastfed or fed breast milk?" In the analyses, "maternal age" was the mother's age at the child's birth. U.S. Census Bureau definitions were used to classify residence, region, and poverty status; thus, residence was classified by Metropolitan Statistical Area (MSA), and poverty was based on household size, composition, and income. These analyses included only children classified as non-Hispanic white or non-Hispanic black and are referred to in this report as white and black, respectively. Weighted percentages were calculated using statistical software to account for complex sample design. The statistical significance of percentage point differences between races and between demographic subgroups within races were estimated using contrast analysis. The results indicated that 71.5% of white and 50.1% of black children (Table 1) were ever breastfed. Breastfeeding rates were lower among black than white children within every subgroup studied and significantly lower (p<0.05) in all subgroups except children ineligible for WIC,* children residing in the Northeast,† and children born to mothers aged <20 years. The greatest percentage point difference between races was among children in rural areas, whereas the smallest percentage point differences were among children ineligible for WIC, children residing in the Northeast, and children born to married mothers. Among both races, children were more likely to have ever been breastfed if they were ineligible for WIC; had mothers who were aged >20 years, married or had at least some college education; lived in the West or in urban areas; or were above the federal poverty threshold. Among children ever breastfed, 53.9% of whites and 43.2% of blacks were still breastfed at age 6 months (Table 2). A significantly smaller proportion of black than white children continued breastfeeding to at least 6 months among both sexes; children first born or not; children ineligible for WIC; children born to mothers aged <20 years or >30 years, or to mothers who had attended college; children living in urban areas, the Midwest, South, and West; and children whose household incomes ranged from 185% to <350% of the poverty level. Among children of both races, older maternal age, higher maternal education, mother being married, and living in the Northeast were positively associated with continuing to breastfeed at 6 months. Among white children, breastfeeding continuation at 6 months was also positively associated with being female, being first born, not participating in WIC, and higher poverty-to-income ratio. Reported by: L Grummer-Strawn, PhD, KS Scanlon, PhD, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion; N Darling, MPH, National Immunization Program; EJ Conrey, PhD, EIS Officer, CDC. Editorial Note:The findings in this report indicate substantial racial and economic disparities in rates of breastfeeding initiation and breastfeeding continuation to at least age 6 months. The findings also demonstrate that race is associated with breastfeeding status independent of socioeconomic and other demographic factors, but also that socioeconomic and other factors are associated with breastfeeding independent of race. Within each income group, the proportion of black children who were ever breastfed was 10 to 17 percentage points lower than that of white children; within each race, the proportion of children ever breastfed was 23 to 26 percentage points higher among those in the highest income group compared with the lowest. Racial differences in breastfeeding continuation rates to 6 months were generally smaller than differences observed in breastfeeding initiation. A comparison of breastfeeding rates and disparities described in this report with the rates measured in the NHANES III survey (4,7), which collected data on breastfeeding among children born from 1982 through 1993, suggests that progress has been made in recent decades to increase breastfeeding initiation and decrease breastfeeding disparities between whites and blacks and between economic strata. Breastfeeding initiation rates increased from 60.3% in NHANES III to 71.5% in the 2004 NIS among white children and from 25.5% to 50.1% among black children. During the same period, the proportion of breastfed children who continued breastfeeding for at least 6 months increased from 44.4% to 53.9% among white children and from 33.3% to 43.2 % among black children, indicating that although both groups improved, the absolute racial disparity did not diminish greatly (11.1% in NHANES III; 10.7% in the 2004 NIS). Because differences existed between NIS and NHANES III methodologies, comparisons between the two surveys should be interpreted with caution. For example, the NHANES interview was conducted in person for children aged 12--72 months, whereas the NIS used telephone interviews and covered children aged 19--35 months. Duration of breastfeeding was assessed in the NHANES interview with the following question: "How old was [child's name] when [child's name] completely stopped breastfeeding or being fed breast milk?" The findings in this report are subject to at least four limitations. First, breastfeeding behavior was based on retrospective self-reports by mothers or other caregivers, whose responses might be subject to recall bias. However, maternal recall has been determined to be valid and reliable for estimating breastfeeding initiation and duration, especially when duration is recalled after a short period (e.g., <3 years) (8). Second, family income and place of residence reported might differ from those at the time the child was being breastfed. Third, survey data were weighted to make them as representative as possible of all children aged 19--35 months; however, the statistical adjustments might not fully account for all survey complexities. Finally, this report does not address exclusive breastfeeding, defined as the consumption of human milk with no supplementation of any type except for vitamins, minerals, and medications (1). Exclusive breastfeeding enhances protection against many diseases and is recommended for the first 6 months of life by the American Academy of Pediatrics (1). Increasing rates of breastfeeding is a crucial strategy for improving children's health, reducing childhood overweight, and reducing health-care costs. For example, increasing the proportion of children breastfed in the early postpartum period from 64% in 2000 to the Healthy People 2010 goal of 75% would save an estimated $3.6 billion in health-care costs annually (1). Although racial and economic disparities in breastfeeding initiation rates appear to have decreased in recent decades, they have not been eliminated. Barriers to breastfeeding initiation and continuation include lack of social support, lack of proper guidance from health-care providers, lack of adequate or timely postpartum follow-up care, and disruptive hospital maternity-care practices (e.g., delays in breastfeeding initiation, use of pacifiers by newborns, and hospital promotion of formula through the provision of free formula in hospital discharge packs) (1,9). Public health measures to promote breastfeeding should continue and should target groups with the lowest initiation rates, such as black mothers in rural (i.e., non-MSA) areas or aged <20 years, mothers who have not completed high school, and participants in the WIC program. Public health programs also should increase protection and support of breastfeeding continuation among the same target groups. For policy makers and others interested in decreasing breastfeeding disparities through improving breastfeeding initiation and duration, The CDC Guide to Breastfeeding Interventions (9) provides an introduction to interventions aimed at promoting and supporting breastfeeding. In addition, breastfeeding interventions should account for racial, ethnic, and socioeconomic variations in attitudes towards breastfeeding and perceived barriers to breastfeeding (1,10). Acknowledgments The findings in this report are based, in part, on contributions by J Chen, MS, R Li, MD, PhD, Div of Nutrition and Physical Activity, National Center for Chronic Disease Prevention and Health Promotion, and E Luman, PhD, National Immunization Program, CDC. References
* Special Supplemental Nutrition Program for Women, Infants, and Children. † Northeast: Connecticut, Maine, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Vermont; Midwest: Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South: Alabama, Arkansas, Delaware, District of Columbia, Florida, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, Virginia and West Virginia; West: Alaska, Arizona, California, Colorado, Hawaii, Idaho, Montana, Nevada, New Mexico, Oregon, Utah, Washington, and Wyoming.
Table 1 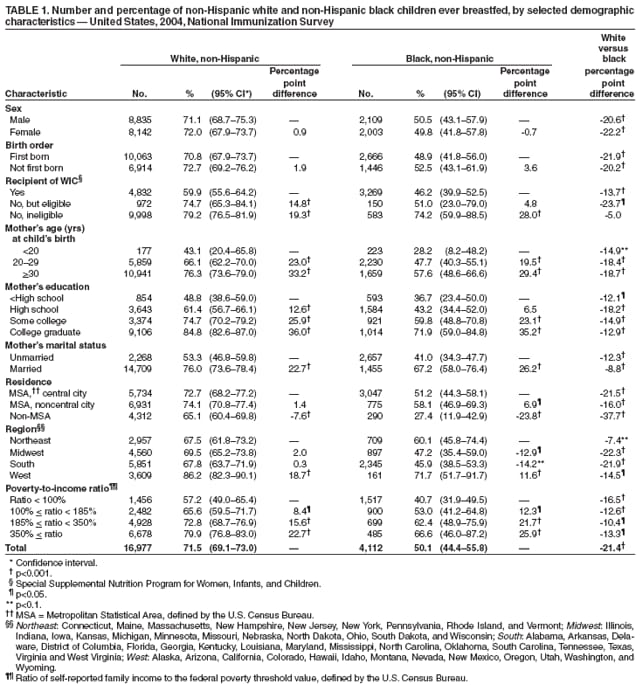 Return to top. Table 2 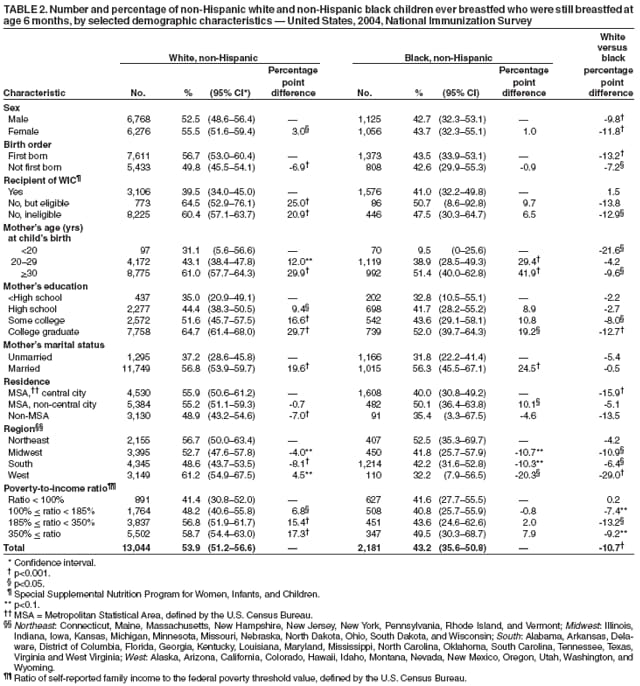 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/29/2006 |
|||||||||
|