 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. International Notes -- Quarantine Measures Smallpox -- Stockholm, Sweden, 1963Reprinted below is the entire series of reports published during May-July 1963 about a smallpox outbreak in Sweden. Selected tables and figures from these reports also have been recreated to resemble the originals as closely as possible. A contemporary Editorial NoteEditorial Note follows the outbreak reports. {From the May 24, 1963, MMWR} Sweden -- Stockholm was declared a smallpox infected area on May 16. A seaman who returned from Indonesia in late March is the apparent source of an outbreak which has now spread through two generations of transmission and has resulted in one fatality. Preliminary information on cases to date, received from the Ministry of Health, Sweden, and forwarded by Dr. Reimert T. Ravenholt, Epidemiologic Consultant, Division of Foreign Quarantine, U.S. Public Health Service, Paris, is given below: The outbreak was recognized on May 13 when the diagnosis of smallpox was first suspected in Case #7. The disease was sufficiently mild in Cases 1, 4, 5 and 12 that medical assistance was not sought. The only fatality to date occurred in Case #2 who apparently suffered an acute hemorrhagic form of the disease, diagnosed as smallpox in retrospect. This outbreak is of unique interest in that it represents one of the few epidemics in Western nations in recent years not evidencing a predominant spread among hospital contacts. Recent immunization programs among hospital personnel presumably have altered the pattern of hospital spread observed in other recent outbreaks. The mildness of the disease in several of the earlier cases, resulting in the failure of these patients to seek medical care and hospitalization, has contributed to the pattern of community transmission. The outbreak emphasizes the sinister role of mild or vaccine-modified cases of smallpox in initiating and propagating outbreaks of severe disease. Since the outbreak was discovered during the second generation of indigenous cases, it is possible that Americans recently in Stockholm have been unknowingly exposed to the disease, and cases of suspicious febrile illness in such individuals should receive the utmost scrutiny by clinicians and public health authorities. {From the May 31, 1963, MMWR} Four additional cases of smallpox have been identified in Stockholm with onsets of illness since May 18. All four presumably acquired their disease as a result of hospital contact. The outbreak (See MMWR, Vol. 12, page 172) now totals 16 cases, with three generations of transmission following the importation of smallpox by a seaman who presumably acquired his disease in transit through Southeast Asia. Information on cases to date received from Dr. Bo Zetterberg, Chief, Epidemiology Division, State Bacteriology Laboratory, Stockholm, is summarized in the table below {See table, page 539} (Table_1). The pattern of spread of the illness is presented diagrammatically in the accompanying figure {See figure, page 540} (Figure_1). The first case to be identified occurred in an unvaccinated 19-year-old bricklayer (Case 7) who had onset of fever, vomiting, and backache on May 5. He was hospitalized three days later and subsequently developed an extensive maculo-papular rash which became pustular by May 12. Smallpox was suspected and confirmed the following day by the laboratory. Immediate epidemiologic investigation revealed that an aunt of the bricklayer (Case 2) had developed on April 18 an acute febrile illness, manifest by hemorrhagic skin lesions, and had died shortly after admission to the hospital on April 23. Ten other cases of smallpox were identified May 14-16. The original source of the outbreak was a 24-year-old seaman who after two weeks residence in Australia left Darwin on March 22 on BOAC Flight #709. In-transit stops of not more than 50 minutes each were made in Djakarta, Singapore, Rangoon, Calcutta, Karachi, Teheran, and Damascus en route to Zurich. At Zurich, the seaman deplaned and the following day boarded Swissair Flight #250, reaching Stockholm March 24. He apparently acquired his disease as a result of in-transit exposure either at a terminal or on the plane. On April 6, 15 days after the flight, he developed a moderate fever and mild rash and remained in the home of his grandmother (Case 3) throughout his illness. Cases 2, 3, 4, and 5 all had contact with him in the grandmother's home during the course of his illness. On April 21, the grandmother fell ill, subsequently exposing three women (Cases 8-10) who visited the home to provide nursing care to the elderly woman prior to her hospitalization on May 27. She was originally diagnosed as having chickenpox and recovered uneventfully. Another resident of the building (Case 11) who lived two stories above the grandmother, developed smallpox but denied acquaintance or contact with the grandmother. Case 2, the first fatality, apparently acquired the illness from the seaman during a visit to the grandmother's apartment and subsequently transmitted it to her husband (Case 6) and her nephew (Case 7) the first identified case. Case 12 who had only fever and serologic evidence of infection, acquired his disease presumably from his fiancee, Case 4. The appearance of cases among hospital contacts is more consistent with the previously observed patterns of imported smallpox in Western countries. Case 13 is a gardener at the Infectious Disease Hospital where Cases 3 and 6 were admitted as presumptive chickenpox on April 27 and May 7, respectively. He is thought to have handled laundry from these patients prior to the first suspicion of smallpox on May 12. He was initially employed by the hospital only two months previous and had not yet been vaccinated in the hospital's annual revaccination program. Case 14 was a patient admitted to the Infectious Disease Hospital with whooping cough on April 30. She was located in the same hospital vicinity as Case 6, although there was no connection between the rooms housing these patients. Cases 15 and 16 were patients on the same hospital ward to which Case 9 was admitted on May 9. Case 9 was originally thought to have a toxic drug eruption prior to her diagnosis of smallpox on May 15. With the exception of Case 12 who had an exceptionally mild illness, it is apparent that spread of the disease to date has been primarily among individuals vaccinated at times far distant in the past. Of the three fatalities to date, one occurred in a person never vaccinated and the other two in persons vaccinated more than 50 years prior to exposure. The absence of additional spread to hospital personnel is probably related to efforts in Sweden to emphasize revaccination of hospital personnel at frequent intervals. Notably, the last four cases have occurred in persons already identified and isolated by virtue of being known contacts. Some 8,000 persons living in neighborhoods of the earlier cases have been vaccinated. In addition, vaccination has been provided for other residents of Stockholm on request and to date some 300,000 persons have availed themselves of this protection. {From the June 7, 1963, MMWR} Three additional cases, two hospital acquired, were identified last week bringing to 19 the total number of smallpox cases comprising the current outbreak, according to information made available by Dr. Bo Zetterberg, Chief, Epidemiology Division, State Bacteriology Laboratory, Stockholm. Two of the three cases are actually part of the second generation of transmission (See MMWR Vol. 12, pg. 174), having now been identified retrospectively by serologic means. Neither patient developed a rash. Both were nurses in the Stockholm Infectious Disease Hospital in close contact with the smallpox cases admitted there. The first, a 44-year-old female, cared for Case No. 3 from April 27 to May 7 daily, including bathing and local treatment of the lesions. On May 9, the nurse developed fever and headache, as well as nausea and low back pain. Except for May 13 and 14, she continued to work throughout her illness until isolated on May 18. She was found to have a very high hemagglutination inhibition antibody titer suggesting recent infection. Her last vaccination prior to onset of illness was in 1962. She was also in daily contact with Cases 6 and 14, and directly or indirectly may have transmitted the disease to Case 14. The second nurse, a 22-year-old female, also employed in the Stockholm Infectious Disease Hospital, had daily contact with Case No. 2 during the period April 27-May 7. On May 11, she experienced onset of headache, fever, and sore throat and was absent from work May 11 through May 13. No rash developed. A high HAI titer verified the diagnosis of smallpox. She had previously been vaccinated in 1950 but at the time of exposure had not yet been revaccinated under the hospital's annual revaccination program. The final additional case is that of a 47-year-old man who had onset of illness May 21 while already isolated as a contact. He is the father of Case 7, the first identified case. He had never been vaccinated until 7 days before onset of illness. The total number of hospital-acquired cases now stands at 6, one-third of the secondary indigenous cases. The evidence supports close contact as the primary requisite for spread both in the hospital and in the community. The disease has spread among persons vaccinated more than 7 years prior to the time of their exposure with 2 notable exceptions, both patients with mild disease without rash. The table below presents data on the vaccination status of the 18 indigenous cases {See table below} (Table_2). {From the June 14, 1963, MMWR} Two additional cases of smallpox were identified in Stockholm last week bringing to 21 the total number of cases in the current outbreak. Unique circumstances involving these two persons, neither of whom were under surveillance as contacts at the time of their detection, indicates that the outbreak may perhaps be expected to continue. Information made available by Dr. Bo Zetterberg, Chief, Epidemiology Division, State Bacteriology Laboratory, Stockholm, indicates that on June 6 an 85-year-old woman, who lives with her daughter, went to a hospital out-patient department for routine follow-up of a chronic medical problem. The daughter called in advance informing clinic personnel that the elderly woman had developed a rash. On arrival at the out-patient clinic, the mother spent some time in the general waiting room and was then referred to the dermatology clinic, and again spent some time in the dermatology waiting room. When seen by physicians, a clinical diagnosis of smallpox was made. In all, she had spent some four hours at the hospital and presumably exposed some 450 persons in the two crowded waiting rooms. It was noted that on May 28 she had developed a low-grade fever with dizziness, followed by the appearance of rash on June 2. She and her 54-year-old daughter share an apartment in a boarding house for women housing some 100 occupants. The daughter works as a mortician and on April 26 had prepared the body of smallpox Case 2 of the outbreak for cremation. She had been placed under surveillance as a contact and 16 days after her exposure to the dead woman, having had no symptoms or signs of illness, she was released from quarantine. She denied any evidence of illness since being released from surveillance. The total elapsed time from her contact with the body of Case 2 and the onset of disease in her mother was 32 days, consistent with two incubation periods of smallpox. Except for the daughter's exposure, no epidemiologic evidence could be found linking the mother with a source of smallpox. Neither the mother nor daughter had been vaccinated since childhood. The daughter demonstrated a high HAI titer on June 6, suggesting a recent infection, and in the absence of an alternative explanation, it may be presumed that the daughter developed a sub-clinical infection and transmitted virus to her mother. Two very unusual aspects of smallpox transmission seem apparent. The daughter, unvaccinated since childhood and exposed to hemorrhagic smallpox, developed an infection so mild as to produce no symptoms, yet developed serologic evidence of infection. Despite the presumed absence of any rash or systemic manifestations of disease, she was apparently able to transmit the illness to her mother. The inadvertent exposure of the mother during her eruptive stage to some 450 persons at the hospital, as well as possible contacts in the boarding house, establishes an additional large group of contacts in which cases may yet occur. An epidemic curve for the outbreak to date is presented showing the chronologic relationship of the generations of transmission {See Figure below} (Figure_2). Using the median date in the span of onset dates for each generation, it is apparent that the median incubation periods for all generations are strikingly similar. {From the July 3, 1963, MMWR} No new cases have been reported during the past week. The total number of confirmed cases remains at 23, including four deaths. The fourth death reported involved an unvaccinated 47-year-old male who died on June 15, 25 days after onset of illness. He was the father of case 7, also a fatality (See MMWR, Vol. 12, No. 21, pp. 174 and 183). {From the July 19, 1963, MMWR} Two additional cases of smallpox were reported from Stockholm on July 11 and July 12, respectively. One of these, an 89-year-old female patient in a mental hospital, had onset of rash and fever on July 7, 15 days after onset of illness in Case 23, a 73-year-old woman also hospitalized at this institution. The total number of confirmed cases that has occurred during the outbreak is 25, including four deaths. Editorial Note -- 1996: Reading this MMWR account of the outbreak of imported smallpox in Sweden during April-July 1963 is as haunting now as it was frightening then. At the time, there was justifiable concern about possible spread of infection from Sweden to the United States, and when residents of Stockholm were offered vaccination during the outbreak, "some 300,000 persons...availed themselves of this protection." Sweden was the first major country to eliminate indigenous smallpox, a distinction it achieved in 1895 (1). This outbreak was the first appearance of imported smallpox there since 1932, except for a single case in 1945 (2). Infecting 25 persons over six indigenous generations of transmission, this was one of the larger such outbreaks in Europe (which had two other imported outbreaks in 1963, four in 1962, and 10 in 1961, for example) after 1958 (3). Despite Sweden's active vaccination efforts among hospital personnel, eight of the indigenous cases were acquired by hospital staff or patients; most of the remainder were infected by face-to-face contact in the homes of case-patients. However, the versatile virus apparently also spread in this one outbreak from a corpse, from laundry of another case-patient, and by remote airborne exposure, and its clinical presentation ranged from six cases (among persons with old vaccinations) who did not develop a rash at all to at least one hemorrhagic case. Several aspects of the outbreak in Sweden differed dramatically from smallpox outbreaks in Great Britain the previous winter following importations from Pakistan. In particular, this outbreak was not recognized until seven cases already had occurred; ambulatory cases with "mild" disease were important in early transmission; the overall case-fatality rate was substantially lower (15% in Sweden versus 40% in Great Britain). At the time, these differences were attributed to vaccine-modification of smallpox associated with the ameliorating influence of partial immunity from distant prior vaccinations. In retrospect, they may reflect infection with a strain of smallpox virus from Indonesia where smallpox historically seemed to be less lethal than on the Indo-Pakistan subcontinent. In the outbreak in Sweden, hospital transmission of smallpox was not prominent in the early generations of disease as it was in most other European outbreaks associated with importation. However, once patients began to be admitted to the hospital, the hospital became the focus of transmission. In addition, transmission also was associated with contact with fatal cases; indeed, handling smallpox corpses and attending funerals of smallpox victims resulted in outbreaks in Africa and other smallpox-endemic areas during the global smallpox eradication campaign (4). Dr. Ronald R. Roberto, an officer in CDC's Epidemic Intelligence Service Program during 1962-1964, went to Stockholm as an international observer during this outbreak. In addition to his role in rapidly communicating emerging information to CDC, he formed relationships with Swedish colleagues -- including epidemiologists H. B. Lundbeck and B. O. Ringertz and virologist J.
This outbreak also highlights how interconnected the world was already in 1963, and it illustrates vividly the potential danger posed to all other humans as long as smallpox existed anywhere on the planet. Even discounting the unknown, apparently chance encounter by which the index patient in this outbreak came to be infected, the capricious nature of many of the subsequent encounters that resulted in indigenous cases in Sweden is breathtaking. The painful lesson was not lost on Sweden, which contributed almost $16 million to the global Smallpox Eradication Program, beginning in 1967, making it the second largest donor after the United States (3). Sweden's generosity was especially important during the final battles against smallpox in India, Bangladesh, and Somalia. Finally, it is fitting that CDC marks the 50th Anniversary of its own founding by commemorating the 200 years since Edward Jenner discovered vaccination in May 1796 and the 30 years since the Nineteenth World Health Assembly resolved in May 1966 to eradicate smallpox over the next 10 years. The CDC effort in helping 20 West and Central African countries to eradicate smallpox early in the global campaign with support provided by the U.S. Agency for International Development and by the Public Health Service remains one of its finest and most beneficial achievements. The glorious legacy of the global Smallpox Eradication Program lives today in the campaigns to eradicate dracunculiasis and poliomyelitis. Others too will follow. Editorial Note by: Donald R. Hopkins, M.D., M.P.H., Carter Center/Global 2000, Atlanta, and Emeritus Deputy Director, CDC. J. Donald Millar, M.D., D.T.P.H. (Lond.), President, Don Millar & Associates, Inc., Atlanta, and Emeritus Director, National Institute for Occupational Safety and Health, Center for Environmental Health, Bureau of State Services, and Smallpox Eradication Program, CDC. References
Table_1 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
SMALLPOX - STOCKHOLM
Summary of Current Information on Cases
==========================================================================================================================
Case Date of Presumed Source Last
No. Age Sex Onset of Infection Vaccination Comment
--------------------------------------------------------------------------------------------------------------------------
1 24 M April 6 Southeast Asia 1959 Modified illness
2 58 F April 18 Case #1 Childhood Died April 23
3 80 F April 21 Case #1 Childhood
4 24 F April 25 Case #1 1943 Modified illness
5 20 F Not known Case #1 1950 No rash (Lab diagnosis)
6 53 M May 3 Case #2 1920 Husband of Case #1
7 19 M May 5 Case #2 Never Died May 28
8 50 F May 5 Case #3 Childhood Home Nurse of Case #3
9 55 F May 5 Case #3 1916 Home Nurse of Case #3
10 67 F May 6 or 9 Case #3 1918
11 72 F May 8 Case #3 1915 No known direct contact
12 22 M May 11 Case #4 1961 Laboratory diagnosis only
13 61 M May 18 Case #3 or 6 1949** Hospital acquired
14 1 F May 19 ? Case #6 Never** Hospital acquired
15 72 F May 24 Case #9 Childhood Hospital acquired--
Died May 27
16 75 F ? May 24 Case #9 Childhood Hospital acquired
-------------------------------------------------------------------------------------------------------------------------
* First identified case.
** Revaccinated within 8 days of onset.
=========================================================================================================================
Return to top. Figure_1 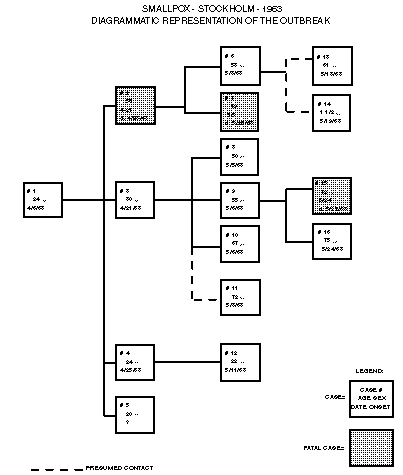 Return to top. Table_2 Note: To print large tables and graphs users may have to change their printer settings to landscape and use a small font size.
==========================================================================================
Clinical Characteristics
Time Lapse Since Last Indigenous -------------------------
Vaccinated Cases Rash No Rash Deaths
------------------------------------------------------------------------------------------
7 yrs. or less 2 - 2 -
8-14 yrs. 3 1 2 -
15-24 yrs. 2 2 - -
25-50 yrs. 4 3 1 -
More than 50 years 4 4 - 2
Never 3 3 - 1
Totals 18 13 5 3
==========================================================================================
Return to top. Figure_2  Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}
{kind=link}