
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Update on Vaccine-Derived Polioviruses --- Worldwide, January 2008--June 2009
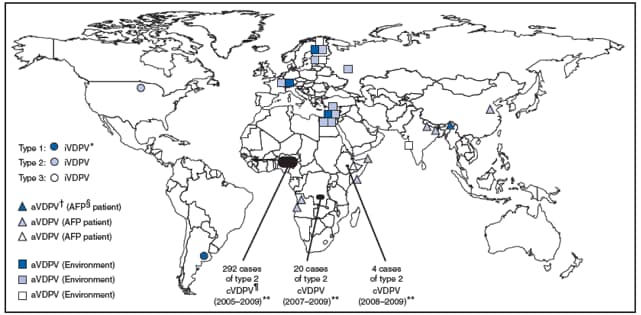
In 1988, the World Health Assembly resolved to eradicate poliomyelitis worldwide (1). Subsequently, the Global Polio Eradication Initiative of the World Health Organization (WHO) reduced the global incidence of polio associated with wild polioviruses (WPVs) from an estimated 350,000 cases in 125 countries in 1988 to 1,651 reported cases in 2008 and reduced the number of countries that have never interrupted WPV transmission to four (Afghanistan, India, Nigeria, and Pakistan) (1). Under current WHO plans, when the goal of eradicating all WPV transmission is attained, oral poliovirus vaccine (OPV) use worldwide eventually will be discontinued. However, because vaccine-derived polioviruses (VDPVs) can produce polio outbreaks in areas with low rates of Sabin OPV coverage and can replicate for years in immunodeficient persons, enhanced strategies are needed to limit emergence of VDPVs (2). This report updates previous summaries (3,4) and describes VDPVs detected worldwide during January 2008--June 2009. During this period, 1) two new outbreaks of circulating VDPVs (cVDPVs) (accounting for 4--20 cases) were identified in the Democratic Republic of Congo and Ethiopia; 2) a previously identified outbreak in Nigeria ultimately resulted in a cumulative total of 292 cases; 3) two newly identified paralyzed immunodeficient persons in Argentina and the United States were found to excrete VDPVs; and 4) isolated VDPVs were found among persons and environmental samples in 11 countries. All countries need to maintain 1) high rates of poliovirus vaccination coverage to prevent VDPV spread and 2) sensitive poliovirus surveillance to detect VDPVs.
Properties of VDPVs
VDPVs can cause paralytic polio in humans and have the potential for sustained circulation. VDPVs resemble WPVs biologically (2) and differ from most Sabin vaccine-related poliovirus (VRPV) isolates by having genetic properties consistent with prolonged replication or transmission. Because poliovirus genomes evolve at a rate of approximately 1% per year, Sabin VRPV isolates that differ from the corresponding OPV strain by >1% of nucleotide positions (usually determined by sequencing the genomic region encoding the major viral surface protein, VP1) are estimated to have replicated for at least 1 year in one or more persons after administration of an OPV dose. This is substantially longer than the normal period of vaccine virus replication of 4--6 weeks in an OPV recipient.
Poliovirus isolates are divided into three serotypes: type 1, type 2, and type 3. Isolates are divided further into three categories, based on the extent of VP1 nucleotide sequence divergence from the corresponding Sabin OPV strain: 1) Sabin VRPVs (≤1% divergent), 2) VDPVs (VRPVs that are >1% divergent from the corresponding Sabin strain), and 3) WPVs (no genetic evidence of derivation from any vaccine strain) (3). VDPVs are further categorized as 1) circulating VDPVs (cVDPVs), when evidence of person-to-person transmission in the community exists; 2) immunodeficiency-associated VDPVs (iVDPVs), which are isolated from persons with primary immunodeficiencies who have prolonged VDPV infections; and 3) ambiguous VDPVs (aVDPVs), which are either clinical isolates from persons with no known immunodeficiency or sewage isolates whose ultimate source is unknown (2).
Virologic Testing for VDPVs
Soon after the recognition of a cVDPV outbreak in Hispaniola in 2001 laboratories of the Global Polio Laboratory Network (GPLN) implemented a protocol to screen for VDPVs, using a combination of molecular and antigenic methods. VRPV isolates identified by molecular methods that had "non--vaccine-like" antigenic properties were candidate VDPVs and were sequenced (2). However, since 2007, some VDPVs, especially less divergent type 2 VDPV (VDPV2) isolates, have undergone limited antigenic evolution and were missed by this screening protocol. A new method based on real-time reverse transcription--polymerase chain reaction (rRT-PCR), which targets nucleotide substitutions that occur early in VDPV emergence, has been evaluated and shown to detect VDPVs with much higher sensitivity and is being implemented as a routine screening method by GPLN as of 2009 (5).
cVDPVs
Democratic Republic of Congo. Retrospective and ongoing characterization of Sabin 2-related isolates by rRT-PCR found 20 acute flaccid paralysis (AFP) cases associated with cVDPV2 (1.1%--2.0% divergent) during 2005--2009 (Figure). Most (n = 15) cases occurred in Katanga Province during 2008--2009, but others occurred in Bandundu (n = 2) in 2005, Sud-Kivu (n = 1) in 2007, Orientale (n = 1) in 2007, and Kasai-Occidental (n = 1) in 2008. The Katanga and Kasai-Occidental isolates had diverged into two main clusters of related lineages, whereas the remaining isolates were unlinked genetically. An additional 13 Sabin 2-related isolates with 0.6%--1.0% VP1 divergence were found in Katanga and elsewhere, some of which clustered geographically and genetically with outbreak viruses.
Ethiopia. Four closely-related cVDPV2 isolates (1.1%--1.2% divergent) were isolated during October 2008 and February 2009 from AFP patients in East Harerghe.
Guinea. A girl aged 6 years, who had received 1 dose of OPV in 2003 and was living in a camp for refugees from Côte d'Ivoire, had AFP onset in May 2009. A VDPV2 (3.5% divergent) was isolated and was found to be closely related to several 2008--2009 cVDPV2 isolates from northern Nigeria.
Nigeria. Since 2005, 292 AFP cases associated with an outbreak of cVDPV2 have been reported in 11 northern and three central states of Nigeria. The outbreak is ongoing, with one case in 2005, 20 in 2006, 68 in 2007, 63 in 2008, and 140 during January--June 2009. Twenty-eight percent (81 of 292) of all cVDPV isolates were from Kano state, which has been a major reservoir for WPV type 1 (WPV1) and WPV3 circulation within Nigeria (1,3). However, the proportion of cVDPV cases occurring outside of Kano increased to 81% during January 2008--June 2009. Genetic analysis of outbreak viruses indicated that the detected cases actually represent several concurrent outbreaks arising from multiple independent cVDPV2 emergences during 2004--2006.
VDPV circulation was largely limited to the northern Nigerian states, where WPV1 and WPV3 circulation has continued (1). Two independent introductions of cVDPV2 into the Republic of Niger from Nigeria were detected in 2006 (3), and an introduction into Guinea was found in 2009. By comparison, WPV1 and WPV3 from Nigeria have spread widely in neighboring countries of Africa (6).
Of the 26 targeted supplementary immunization activities (SIAs)* conducted in Nigeria since 2006, 16 have used monovalent OPV type 1 (mOPV1), five have used mOPV3, and sixhave used trivalent OPV (tOPV) (most recently during May 30--June 2, 2009 [as of June 30, 2009]). Routine immunization uses tOPV, but its use is estimated to be only 61% nationwide and much lower in the northern states.
iVDPVs
Since the introduction of OPV in 1961, approximately 40 persons with B-cell immunodeficiencies have been found to be excreting iVDPVs, which are indicative of prolonged infections. Currently, no effective therapies to clear iVDPV infections are available.
Argentina. A boy aged 15 months with x-linked agammaglobulinemia, who had received three OPV doses in his first months of life, developed AFP in April 2009. iVDPV1 (3.6%--3.8% divergent) was isolated from two serial stool specimens. No other VDPVs were detected among 87 contacts tested.
United States. OPV use in the United States ceased after 1999.† In December 2008, a woman aged 44 years with a >20 year history of common-variable immunodeficiency developed ascending paralysis in all limbs and respiratory insufficiency. She died in March 2009 from various complications of her chronic illness, including neurologic sequelae. Highly divergent (12.3%) iVDPV2 was isolated from a pre-mortem stool specimen. A household member had received three OPV doses 13 years before onset of AFP in the decedent, and the estimated age of the iVDPV2 suggests that one of those doses could have been the source of exposure. This infection is independent of the VDPV1 that circulated in an undervaccinated rural Minnesota community in 2005 (7).
aVDPVs
aVDPVs have been isolated in 11 countries during January 2008--June 2009 (Table). Descriptions of the most divergent aVDPVs, all from sewage samples, follow.
Estonia. Highly divergent (approximately 15%) aVDPV2 and aVDPV3 were isolated from separate sewage samples taken in September and December 2008. The isolates had sequence properties that suggested that they originated from a common infection, and the aVDPV3 is related to another Estonian aVDPV3 isolated from sewage described previously (2,8).
Finland. Highly divergent (approximately 15%) aVDPV1, aVDPV2, and aVDPV3 were isolated from sewage samples collected in Tampere in December 2008 and June 2009. The isolates had sequence properties that suggested that they originated from a common infection. The Finnish aVDPVs are distinct from the Estonian aVDPVs.
Israel. Environmental monitoring for polioviruses was implemented by Israel after its 1987--1988 WPV1 outbreak. Monitoring sewage samples from the Tel Aviv area (sampling populations of approximately 350,000 and 10,000) yielded two groups of type 2 aVDPVs (9). The first group was detected initially in 1998, and 19 more highly divergent representatives (approximately 15% divergent) were detected during 2008--2009. The second group, detected since 2006, is less divergent (approximately 7%) and is defined by 10 isolates. Despite follow-up investigations, no source for these VDPVs has been identified. An aVDPV1 (8.2% divergent) was isolated from an environmental sample collected from a site sampling a different population in Haifa on February 22, 2009.
Reported by: Polio Eradication Dept, World Health Organization, Geneva, Switzerland. Div of Viral Diseases, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC.
Editorial Note:
The recent VDPV emergences reinforce some key lessons for the Global Polio Eradication Initiative. The cVDPV2 outbreak in Nigeria, whose 4-year duration is surpassed only by the decade-long cVDPV2 outbreak in Egypt during 1983--1993 (10), further demonstrates that cVDPVs, like WPV, can circulate indefinitely in settings with low rates of poliovirus vaccination coverage. The emergence of multiple independent cVDPV2 lineages in Nigeria and the unrelated cVDPV2 outbreaks in the Democratic Republic of Congo and Ethiopia highlight the particular risks for emergence of cVDPV2 in settings of low tOPV coverage (10). Improvements in laboratory methods for the identification of VDPV2 facilitated early detection of the outbreaks in the Democratic Republic of Congo and Ethiopia, but maintenance of sensitive AFP surveillance was crucial; any temporal and geographic clustering of vaccine-related isolates of the same serotype should prompt further investigation.
The appearance of an iVDPV case in the United States 13 years after the likely exposure and 9 years after cessation of OPV use illustrates the continued risk among immunodeficient persons from past OPV use. Chronic iVDPV excretors (i.e., excretion for >5 years) have been described in several countries that have shifted to inactivated poliovirus vaccine (IPV) (2), and the highly divergent aVDPVs found in sewage in Israel, Estonia, and Finland have similar genetic properties to iVDPVs from chronic excretors. The appearance of an iVDPV case in Argentina further underscores the risks of prolonged iVDPV excretion in middle-income countries (2,3).
Several of the aVDPVs described in this report show only limited divergence (1.1%--1.5%) and were detected after implementation of the new rRT-PCR screening methods. In some settings such isolates are observed sporadically, and no genetically linked VDPVs are found subsequently. However, in settings of potential low local tOPV coverage, the sporadic detection of aVDPVs should prompt further clinical investigation (when the patient is identified), review of surveillance and polio vaccination coverage data, and implementation of vaccination campaigns (mop-ups and SIAs, usually with tOPV) to prevent virus spread.
Experience has underscored the importance of routine immunization either with IPV or tOPV to prevent VDPV spread (10). In countries with low rates of routine vaccination, closing the immunity gaps to all three poliovirus serotypes by periodic but regular use of tOPV in SIAs is important. However, high rates of tOPV coverage will not prevent or clear VDPV infections in immunodeficient hosts. WHO, in collaboration with other partners, is exploring antiviral compounds for their potential to clear iVDPV infections (3).
References
- CDC. Progress toward interruption of wild poliovirus transmission---worldwide, 2008. MMWR 2009;58:308--12.
- CDC. Update on vaccine-derived polioviruses. MMWR 2006;55:1093--7.
- CDC. Update on vaccine-derived polioviruses---worldwide, January 2006--August 2007. MMWR 2007;56:996--1001.
- CDC. Laboratory surveillance for wild and vaccine-derived polioviruses---worldwide, January 2007--June 2008. MMWR 2008;57:967--70.
- CDC. Laboratory surveillance for wild and vaccine-derived polioviruses---worldwide, January 2008--June 2009. MMWR 2009;58:950--4.
- CDC. Wild poliovirus type 1 and type 3 importations---15 countries, Africa, 2008--2009. MMWR 2009;58:357--62.
- Alexander JP, Ehresmann K, Seward J, et al. Transmission of imported vaccine-derived poliovirus in an under-vaccinated community---Minnesota, USA. J Infect Dis 2009;199:391--7.
- Blomqvist S, Savolainen C, Laine P, et al. Characterization of a highly evolved vaccine-derived poliovirus type 3 isolated from sewage in Estonia. J Virol 2004;78:4876--83.
- Shulman LM, Manor Y, Sofer D, et al. Neurovirulent vaccine-derived polioviruses in sewage from highly immune populations. PLoS One 2006;1:e69.
- Kew OM, Sutter RW, de Gourville EM, Dowdle WR, Pallansch MA. Vaccine-derived polioviruses and the endgame strategy for global polio eradication. Annu Rev Microbiol 2005;59:587--635.
* Mass campaigns conducted during a short period (days to weeks) during which a dose of OPV is administered to all children aged <5 years, regardless of previous vaccination history. Campaigns can be conducted nationally or in portions of the country.
† Additional information available at http://www.cdc.gov/mmwr/preview/mmwrhtml/rr4905a1.htm.
* Immunodeficiency-associated VDPV.
† Ambiguous VDPV.
§ Acute flaccid paralysis.
¶ Circulating VDPV.
** Spread of cVDPVs followed the elimination of the corresponding serotype of indigenous wild poliovirus, but with continued introduction of oral poliovirus vaccine into communities with growing immunity gaps. All of the cVDPV outbreaks were detected first by the laboratory, using sequence data and evolutionary analyses.
Alternative Text: The figure above shows vaccine-derived polioviruses (VDPVs) detected worldwide, January 2008-June 2009. Retrospective and ongoing characterization of Sabin 2-related isolates by rRT-PCR found 20 acute flaccid paralysis cases associated with cVDPV2 (1.1%-2.0% divergent) during 2005-2009.
|
TABLE. Vaccine-derived polioviruses (VDPVs) detected worldwide, January 2008--June 2009 |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
Category |
Country |
Year(s) detected* |
Source |
Serotype |
No. of isolates† |
VP1 divergence from Sabin OPV§ strain |
Routine coverage with 3 doses of poliovirus |
Estimated duration of VDPV replication** |
Current status (date of last outbreak case, last patient isolate, |
||
|
Cases |
Contacts |
Environmental samples |
|||||||||
|
cVDPV†† |
Nigeria§§ |
2005--2009 |
Outbreak (292 cases)¶¶ |
2 |
292 |
--- |
--- |
1.0--5.1 |
61 |
5 yrs |
June 27, 2009 |
|
Guinea |
2009 |
Importation (1 case)*** |
2 |
1 |
--- |
--- |
3.5 |
71 |
--- |
May 12, 2009 |
|
|
Democratic Republic of Congo |
2005--2009 |
Outbreak (20 cases)¶¶ |
2 |
33 |
--- |
--- |
1.0--2.0 |
68 |
4 yrs |
March 7, 2009 |
|
|
Ethiopia |
2008--2009 |
Outbreak (4 cases) |
2 |
4 |
--- |
--- |
1.2 |
75 |
1 yr |
February 16, 2009 |
|
|
iVDPV††† |
Argentina |
2009 |
AFP§§§ patient (XLA¶¶¶) |
1 |
1 |
--- |
2 |
3.6--3.8 |
94 |
≥15 mos |
Alive (April 23, 2009) |
|
United States |
2009 |
AFP patient (CVID****) |
2 |
1 |
--- |
--- |
12.3 |
96 (IPV††††) |
13 yrs |
Died in March 2009 |
|
|
aVDPV§§§§ |
Angola |
2008 |
AFP patient |
2 |
1 |
--- |
--- |
1.1 |
75 |
1 yr |
May 5, 2008 |
|
2008 |
AFP patient |
2 |
1 |
--- |
--- |
1.1 |
1 yr |
May 25, 2008 |
|||
|
China |
2009 |
AFP patient |
2 |
1 |
--- |
--- |
1.2 |
99 |
1 yr |
February 22, 2009 |
|
|
Egypt |
2008 |
Environment |
2 |
--- |
1 |
1.7 |
97 |
1.5 yrs |
April 7, 2008 |
||
|
Estonia |
2008 |
Environment |
2 |
--- |
--- |
1 |
14.5 |
95 |
>15 yrs |
September 25, 2008 |
|
|
2008 |
Environment |
3 |
--- |
1 |
15.6 |
>15 yrs |
December 29, 2008 |
||||
|
Ethiopia |
2009 |
AFP patient |
3 |
1 |
--- |
--- |
1.3 |
75 |
1 yr |
April 30, 2009 |
|
|
Finland |
2008--2009 |
Environment |
1 |
--- |
--- |
1¶¶¶¶ |
12.4 |
97 (IPV) |
13 yrs |
December 15, 2008 |
|
|
2008--2009 |
Environment |
2 |
--- |
--- |
1 |
12.7 |
13 yrs |
December 15, 2008 |
|||
|
2009 |
Environment |
3 |
--- |
--- |
1 |
14.6 |
14 yrs |
June 26, 2009 |
|||
|
India |
2009 |
AFP patient |
1 |
1 |
--- |
--- |
1.1 |
66 |
1 yr |
April 7, 2009 |
|
|
2009 |
AFP patient |
2 |
1 |
--- |
--- |
1.3 |
1 yr |
April 30, 2009 |
|||
|
2009 |
AFP patient |
2 |
1 |
--- |
--- |
1.1 |
1 yr |
June 29, 2009 |
|||
|
2009 |
Environment |
3 |
--- |
--- |
1 |
1.2 |
1 yr |
May 20, 2009 |
|||
|
Israel |
2009 |
Environment |
1 |
--- |
--- |
1 |
8.2 |
95 (IPV) |
8 yrs |
February 22, 2009 |
|
|
1998--2009 |
Environment |
2 |
--- |
--- |
33***** |
8.8--15.3 |
>15 yrs |
January 20, 2009 |
|||
|
2006--2009 |
Environment |
2 |
--- |
--- |
10***** |
6.6--9.7 |
10 yrs |
November 25, 2008 |
|||
|
Malawi |
2008††††† |
AFP patient |
3 |
1 |
--- |
--- |
3.1 |
92 |
3 yrs |
January 14, 2008 |
|
|
Russia |
2008 |
Healthy child |
1 |
1 |
--- |
--- |
1.4 |
98 (IPV) |
1 yr |
Alive (March 2008) |
|
|
Somalia |
2008 |
AFP patient |
2 |
1 |
--- |
--- |
1.1 |
24 |
1 yr |
April 5, 2008 |
|
|
2008 |
AFP patient |
2 |
1 |
1 |
--- |
1.6 |
1 yr |
June 24, 2008 |
|||
|
Switzerland |
2008 |
Environment |
2 |
--- |
--- |
1 |
1.2 |
95 (IPV) |
1 yr |
January 2008 |
|
|
2008 |
Environment |
1 |
--- |
--- |
1 |
1.1 |
1 yr |
March 2008 |
|||
|
* Total years detected and cumulative totals for the previously reported cVDPV outbreak (Nigeria). † Includes environmental aVDPV isolates (Israel). § Oral poliovirus vaccine. ¶ Based on 2008 data from the World Health Organization (WHO) Vaccine Preventable Diseases Monitoring System (2009 global summary) and WHO-UNICEF coverage estimates, available at http://www.who.int/immunization_monitoring/en/globalsummary/countryprofileselect.cfm. National data might not reflect weaknesses at subnational levels. ** Duration of cVDPV circulation was estimated from extent of VP1 nucleotide divergence from the corresponding Sabin OPV strain; duration of immunodeficiency-associated VDPV replication was estimated from clinical record by assuming that exposure was from initial receipt of OPV; duration of ambiguous VDPV replication was estimated from sequence data. †† Circulating VDPV. Most cVDPV isolates from Nigeria, Democratic Republic of Congo, Ethiopia, and Guinea were vaccine/nonvaccine recombinants. §§ Previously reported outbreak; OPV coverage <50% around cases. ¶¶ Excludes isolates 0.5%--1.0% divergent from Sabin 2 that are closely related to the cVDPV isolates: 16 from Nigeria and 13 from Democratic Republic of Congo. Some of the isolates formed genetic lineages. *** Importation from Nigerian cVDPV outbreak. Isolate shared >60% of nucleotide differences from Sabin 2 with cVDPV isolates from northern Nigeria. ††† Immunodeficiency-associated VDPV. None of the iVDPV isolates appeared to be vaccine/nonvaccine recombinants. §§§ Acute flaccid paralysis. ¶¶¶ X-linked agammaglobulinemia. **** Common variable immunodeficiency. †††† Inactivated poliovirus vaccine. §§§§ Ambiguous VDPV. None of the aVDPV isolates appeared to be vaccine/nonvaccine recombinants. ¶¶¶¶ Types 1 and 2 aVDPVs were isolated from the same environmental sample. ***** Two separate lineages of type 2 aVDPVs were isolated from environmental samples in Israel. ††††† AFP onset on December 23, 2007. |
|||||||||||
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/17/2009