|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
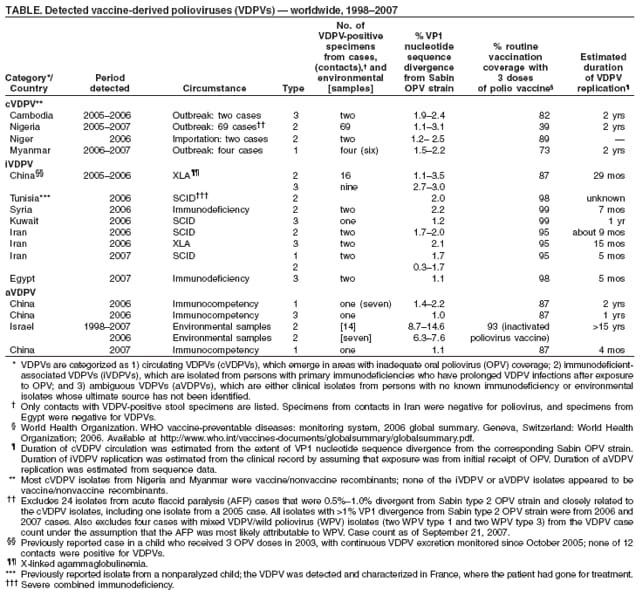
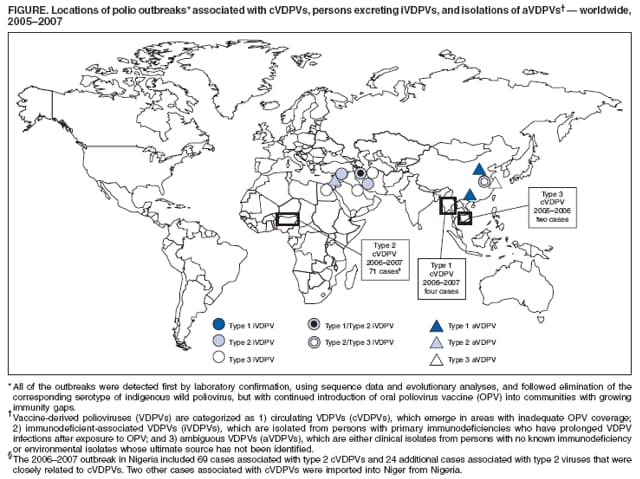
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update on Vaccine-Derived Polioviruses --- Worldwide, January 2006--August 2007In 1988, the World Health Assembly resolved to eradicate poliomyelitis worldwide. Subsequently, the Global Polio Eradication Initiative of the World Health Organization (WHO) reduced the global incidence of polio associated with wild polioviruses (WPVs) from an estimated 350,000 cases in 1988 to 1,998 reported cases in 2006 and reduced the number of countries that have never succeeded in interrupting WPV transmission to four (Afghanistan, India, Nigeria, and Pakistan) (1). However, because vaccine-derived polioviruses (VDPVs) can produce polio outbreaks in areas with low rates of Sabin oral poliovirus vaccine (OPV) coverage and can replicate for years in immunodeficient persons, enhanced strategies are needed to limit emergence of VDPVs and stop all use of OPV once WPV transmission is eliminated (2,3). This report updates a summary of VDPV activity published in 2006 (3) and describes VDPVs detected during January 2006--August 2007. Properties of VDPVsVDPVs can cause paralytic polio in humans and the potential for sustained circulation of poliovirus. VDPVs resemble WPVs biologically (3) and differ from the majority of Sabin vaccine--related poliovirus isolates by having genetic properties consistent with prolonged replication or transmission. Because poliovirus genomes evolve at a rate of approximately 1% per year, Sabin vaccine--related isolates that differ from the corresponding OPV strain by more than 1% of nucleotide positions (usually determined by sequencing the genomic region encoding the major viral surface protein, VP1) are estimated to have replicated for at least 1 year after administration of an OPV dose. This is substantially longer than the normal period of vaccine virus replication of 4--6 weeks. Poliovirus isolates can be distinguished by their three serotypes: type 1, type 2, and type 3. Isolates also can be divided into three categories, based on the extent of VP1 nucleotide sequence divergence from the corresponding Sabin OPV strain: 1) Sabin vaccine--like viruses (<1% divergent), 2) VDPVs (1%--15% divergent), and 3) WPVs (>15% divergent) (4). VDPVs are further categorized as 1) circulating VDPVs (cVDPVs), which emerge in areas with inadequate OPV coverage; 2) immunodeficient-associated VDPVs (iVDPVs), which are isolated from persons with primary immunodeficiencies who have prolonged VDPV infections after exposure to OPV; and 3) ambiguous VDPVs (aVDPVs), which are either clinical isolates from persons with no known immunodeficiency or environmental isolates whose ultimate source has not been identified (3). cVDPVsCambodia. In Phnom Penh, a second case associated with a type 3 cVDPV was detected in January 2006 (the first was in November 2005) (3). In response, three high-coverage supplementary immunization activity (SIA*) rounds were conducted in March, April, and May 2006 in areas where persons are at high risk for infection. Nigeria. During January 1, 2006--August 17, 2007, a total of 69 polio cases associated with type 2 cVDPV were detected in nine northern states of Nigeria in children with acute flaccid paralysis (AFP) (Figure, Table).† An additional 24 type 2 case isolates with 0.5%--1.0% VP1 divergence from the Sabin type 2 OPV strain and belonging to the same lineages as the cVDPV isolates were detected in eight of the nine northern states. At least 46 (49%) of the cVDPV isolates and closely related isolates were from Kano state, which has been a major reservoir for WPV type 1 (WPV1) and type 3 (WPV3) circulation (5). Phylogenetic analysis based on sequences of the complete capsid region (2,643 nucleotides) revealed at least seven distinct cVDPV genetic lineages, suggesting independent emergence of multiple cVDPV transmission chains in 2005 and 2006. VDPV circulation has been limited to the northern Nigerian states, where WPV circulation occurred during 2006--2007 (5). Individual lineages generally have been geographically restricted, with spread mostly limited to neighboring states. Circulation of five separate chains of transmission continued at least into July 2007, and 48 of the cVDPV isolates and closely related isolates were from 2007 cases (Figure). The most recent VDPV case was reported in a person with onset of paralysis August 17. Two AFP cases associated with two distinct type 2 VDPV lineages from Nigeria were reported in border communities in Niger in June and October 2006. SIAs have been conducted throughout 2006 and 2007, using three different vaccine preparations. In states with both VDPV and WPV cases, SIA rounds using trivalent OPV (tOPV) were conducted during February 11--14 and November 16--24, 2006, and during January 25--28, March 1--4, and September 1--4, 2007. SIA rounds using monovalent OPV type 1 (mOPV1)§ were conducted in affected states during March 11--14, May 27--30, June 29--July 3, and September 7--11, 2006, and during March 29--April 1 and June 23--26, 2007. Administration of mOPV3 was conducted in affected states during July 28--31, 2007. Myanmar. Four cases of polio associated with a type 1 cVDPV were detected in Myanmar (in Mandalay, April 19, 2006; Yangon, May 2, 2007; Kayin, June 11, 2007; and Bago East, July 21, 2007). Case isolates differed from the Sabin type 1 OPV strain at 1.5%--2.2% of VP1 positions, consistent with up to 2 years of circulation of the cVDPV, beginning as early as mid-2005. Seven contacts of the first polio patient, from two adjacent townships, also were infected with the cVDPV. In response to the cVDPV outbreak, two rounds of SIAs were conducted in 2006 in townships in close proximity to the first case. SIAs with mOPV1 were conducted in 17 townships in five states during September 3--5, 2007, followed by nationwide SIAs with mOPV1 in November and December. iVDPVsChina. In Anhui Province, a child with X-linked agammaglobulinemia who received 3 OPV doses in fall 2003 was previously reported with onset of paralysis in August 2005 (3). Serial stool specimens taken from the child during October 2005--February 2006 were positive for type 2 and 3 iVDPVs. Treatment with intravenous immunoglobulin did not clear the infections, and the child died from severe pneumonia in April 2006. Tests determined that none of 12 contacts were excreting poliovirus. Iran. In Iran, the detection of AFP cases associated with VDPVs was followed up by detailed clinical investigations. Type 2 iVDPVs with self-limiting clinical courses had been detected previously in 1995 and 2005 (3). During 2006--2007, three immunodeficient AFP patients were excreting iVDPVs; two of the patients, both with severe combined immunodeficiency, died. The third patient, who had X-linked agammaglobulinemia, was infected with a type 3 iVDPV, and stopped excreting poliovirus after December 2006. Tests determined that none of 21 contacts of the three patients were excreting poliovirus. Syria. Syria has detected and investigated VDPVs since 2001 (3). In 2006, humoral and cell-mediated immunodeficiency was diagnosed in an AFP patient, and stool specimens collected 4--8 days after onset of paralysis were positive for type 2 iVDPV. Tests determined that none of five contacts were excreting poliovirus. Kuwait and Egypt. An Egyptian child with severe combined immunodeficiency residing in Kuwait was determined to be excreting type 3 iVDPV. A second immunodeficient child in Egypt was infected with a different type 3 iVDPV and died. aVDPVsChina. In June 2006, a type 1 aVDPV was isolated from an immunocompetent AFP patient and seven close contacts in rural Guangxi Province. Sequence diversity among the isolates was consistent with localized VDPV circulation (Table). A type 3 aVDPV was isolated from a healthy patient in Shanghai in August 2006; subsequent stool specimens were negative. In addition, type 1 aVDPV was isolated from a child with AFP in Shanxi Province in 2007. Israel. Environmental monitoring for polioviruses was implemented by Israel after its 1987--1988 outbreak of WPV1. Monitoring sewage samples from the Tel Aviv area (sampling populations of approximately 350,000 and 10,000) has yielded two groups of type 2 aVDPVs. The first group was detected initially in 1998, and six more highly divergent representatives (approximately 14% VP1 divergence from the Sabin type 2 OPV strain) were detected during 2006--2007; the most recent positive sample was collected on July 23, 2007 (6). The second group is less divergent from the Sabin type 2 OPV strain (approximately 7%) and is defined by seven 2006 isolates; the most recent positive sample was collected on December 12, 2006. Despite follow-up investigations, no source for these VDPVs has been identified. Genetic properties of the isolates (highly diverse antigenic structures and absence of vaccine/nonvaccine recombination) are more similar to iVDPVs than to cVDPVs (6). Reported by: Global Specialized Polio Reference Laboratory, National Institute for Infectious Diseases, Tokyo, Japan. National Polio Laboratory, Univ of Maiduguri Teaching Hospital, Maiduguri; National Polio Laboratory, Univ of Ibadan, Ibadan, Nigeria. National Polio Laboratory, Institut Pasteur, Dakar, Senegal. African Regional Polio Reference Laboratory, National Institute for Communicable Diseases, Johannesburg, South Africa. National Polio Laboratory, National Health Laboratory, Yangon, Myanmar. Regional Polio Reference Laboratory, Virus Research Institute, Bangkok, Thailand. National Polio Laboratory, Central Laboratory, Damascus, Syria. National Polio Laboratory, Kuwait. National Polio Laboratory, Univ of Tehran, Tehran, Iran. Regional Polio Reference Laboratory, Vacsera, Cairo, Egypt. Global Specialized Polio Reference Laboratory, National Institute for Public Health and Environmental Protection, Bilthoven, Netherlands. Regional Polio Reference Laboratory, China CDC, Beijing, China. National Polio Laboratory, Central Virology Laboratory, Tel Hashomer, Israel. Polio Eradication Initiative Dept, World Health Organization, Geneva, Switzerland. Div of Viral Diseases and Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:The close integration of AFP surveillance with detailed poliovirus characterization by the Global Polio Laboratory Network (3) has led to detection of VDPVs in more diverse settings and identification of key biologic and genetic properties of VDPVs. Further understanding through laboratory findings will be vital to improving strategies for managing risk factors associated with emergence of VDPVs (7). The Nigerian cVDPVs and related isolates detected during 2006--2007 differ from previously described cVDPVs by the absence of antigenic changes detectable by enzyme-linked immunosorbent assay screening (3). Temporal and geographic clustering of vaccine-related type 2 poliovirus isolates in northern Nigeria prompted further laboratory investigations. To close this gap in laboratory detection of VDPVs, new molecular reagents and methods based on real-time polymerase chain reaction have been developed (8). Testing of the new molecular methods has been accelerated, which should increase substantially the sensitivity of laboratory screening for all VDPVs, especially type 2 VDPVs. Multiple Nigerian type 2 polioviruses in the recent outbreak had <1% VP1 divergence but shared distinctive nucleotide substitution patterns and recombination sites with the recognized cVDPVs, which indicated their epidemiologic role; all were associated with paralytic illness. cVDPVs detected in 2006--2007 provide further evidence that the key risk factor for spread of VDPVs is low vaccination coverage (3,4). In Nigeria in 2005, 15%--50% of children aged <5 years with cVDPVs, in seven of the nine states, had not received an OPV dose. This was reduced to 6%--30% by the end of 2006 (5,9) through steadily improving SIAs (5). The low rates of routine tOPV coverage combined with the finding of multiple independent cocirculating cVDPV lineages in much of northern Nigeria suggest that conditions favorable for type 2 cVDPV emergence and spread existed in multiple locations in that part of the country. In Niger, routine tOPV coverage has been greater (89%) than in Nigeria (39%), and the 2006--2007 SIAs administered tOPV, which limited further VDPV transmission. In Myanmar, high rates of routine OPV coverage also appear to have limited cVDPV circulation, with cases reported only in low-coverage communities. Experience suggests that cVDPV outbreaks can be terminated if high OPV coverage can be achieved during follow-up SIAs (3). Outbreaks can be prevented by maintaining high polio vaccination coverage through routine vaccination and SIAs. The first detections of iVDPVs and all of the long-term iVDPV chronic infections (>3 years) detected to date were in countries with high-income economies¶ (e.g., Japan and countries in Western Europe and North America) (3). More recent reports of iVDPVs have come from countries with middle-income economies such as Argentina, Kazakhstan, Thailand, Iran, and Syria (3), with no evidence of chronic infections or spread of VDPVs to household or community contacts. Repeated detection of iVDPVs in varied settings underscores the continuing risks for iVDPV emergence as long as OPV is used. Unlike cVDPVs, which can be prevented from emerging by high rates of OPV coverage, iVDPVs potentially can arise any time a person with a primary immunodeficiency is exposed to OPV, either as an OPV recipient or as a contact of a recipient. The only way to prevent new iVDPV infections is to stop OPV use. The environmental aVDPV isolates from Israel, as with those previously isolated from sewage in Estonia (type 3) and Slovakia (type 2) (3), likely are iVDPVs, based on their genetic and antigenic properties, and might have resulted in limited transmission to close contacts. However, measures to identify infected persons have been unsuccessful, and the possibility exists that the VDPV infections were asymptomatic. Continued cVDPV outbreaks, emergence and detection of iVDPVs in certain persons with B-cell immunodeficiencies, and detection of aVDPVs in diverse settings underscore the risks associated with continuing use of OPV after WPV has been eradicated. However, until that time, OPV must be used at high rates of coverage to interrupt WPV transmission and prevent the spread of VDPVs, particularly in countries with low-income economies, high population densities, poor sanitation, and tropical climates. Although chronic iVDPV infections are rare, no effective means exist for clearing such infections (10). Consequently, while working to interrupt all remaining WPV transmission, the Global Polio Eradication Initiative also must continue to reduce the risk for VDPV emergence and transmission by strengthening routine vaccination in underperforming countries,** developing strategies to clear iVDPV infections with new antiviral drugs (10), and refining strategies for stopping all OPV use after global eradication of WPVs (2,7). References
* Mass campaigns conducted during a short period (days to weeks) in which a dose of OPV is administered to all children aged <5 years, regardless of previous vaccination history. Campaigns can be conducted nationally or in portions of the country. † Data as of September 21, 2007, representing 100% of laboratory analyses for AFP cases with onset of paralysis through July 2007 and approximately 61% of cases with onset in August. A total of 197 cases of confirmed WPV were reported provisionally in the country for the period January 1--August 31, 2007 (60 WPV1 cases and 137 WPV3 cases), compared with 543 in 2005 (333 WPV1 and 210 WPV3), and 941 in 2006 (764 WPV1 and 177 WPV3) during the same period. § mOPV1 contains polio vaccine against PV1 only and does not provide protection against other poliovirus types. However, mOPV1 and mOPV3 provide greater immunity to their respective poliovirus types than that provided by the same number of doses of tOPV. Because the type 2 component of tOPV is highly immunogenic, an mOPV2 formulation is unnecessary, leaving polio programs to maximize their immunization activities against the type 1 and type 3 serotypes. ¶ World Bank country groups, by income, available at http://www.worldbank.org/data/countryclass/classgroups.htm. ** Additional information is available http://www.who.int/vaccines-documents/docspdf05/givs_final_en.pdf.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/26/2007 |
|||||||||
|