|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
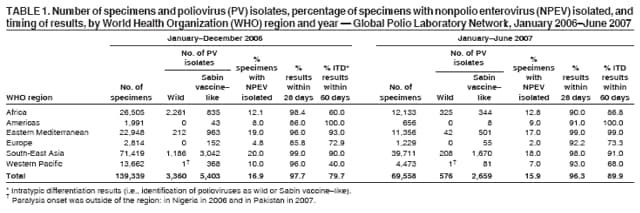
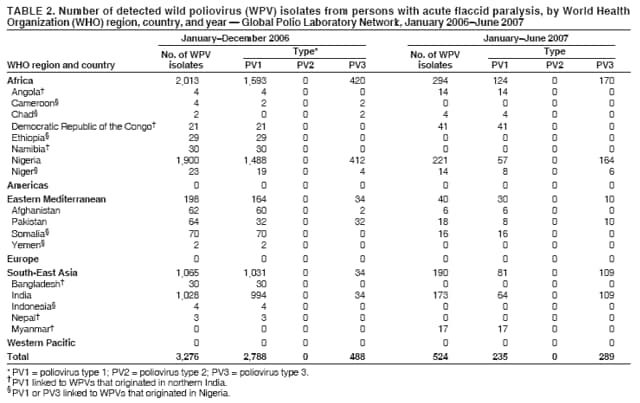
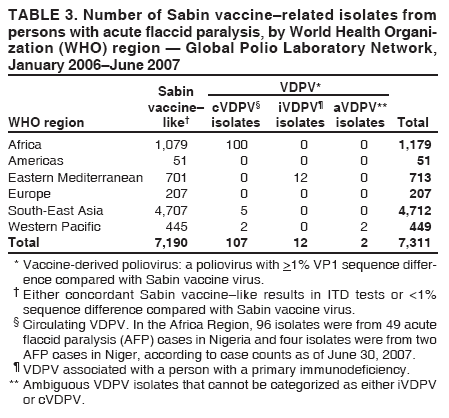
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Laboratory Surveillance for Wild and Vaccine-Derived Polioviruses --- Worldwide, January 2006--June 2007The Global Polio Laboratory Network (GPLN) was established after announcement of the 1988 World Health Assembly resolution to eradicate poliomyelitis. Operating in all six World Health Organization (WHO) regions, the network currently has 146 laboratories that test stool specimens from acute flaccid paralysis (AFP) patients* for polioviruses. The virologic data provided by GPLN underpin the global polio eradication initiative, guiding decisions regarding where targeted immunization activities should be conducted, based on confirmed wild or vaccine-derived poliovirus circulation. The data also are used to monitor progress toward polio eradication by documenting the genetic diversity and transmission links of viral isolates. This report updates previous reports (1--6) and describes GPLN performance and initiatives during January 2006--June 2007. Laboratory Network PerformanceGPLN uses standardized methods, and the quality, timeliness, and accuracy of network results are evaluated against performance targets through an accreditation program administered by WHO that includes proficiency testing and periodic on-site performance reviews. By 2006, WHO had accredited 93% of the network laboratories. Nonaccredited laboratories continue to test specimens, but in parallel with accredited laboratories until any performance problems are resolved. During January 2006--June 2007, GPLN analyzed 208,897 stool specimens, a 55% increase from January 2005--June 2006 (1). The number of tests increased primarily as a result of a decision to increase AFP surveillance sensitivity in polio-endemic regions (Africa, Eastern Mediterranean, and South-East Asia), but also as a result of an upsurge in wild poliovirus transmission in Nigeria and India and virus importations into several other countries. All six WHO regions met the program target of >80% of laboratories providing virus isolation results within 28 days (Table 1). A second target, >80% of laboratories obtaining intratypic differentiation (ITD) (i.e., identification of polioviruses as wild or Sabin vaccine--like) results within 60 days of paralysis onset, was not met in three regions (Africa, Europe, and Western Pacific). However, failure to meet the 60-day target usually resulted from shipping delays that were beyond the control of laboratories. Detection and Characterization of Wild PoliovirusesDuring January 2006--June 2007, GPLN confirmed wild polioviruses in 18 countries (Table 2). Only wild poliovirus types 1 (PV1) and 3 (PV3) were detected. Wild poliovirus type 2 (PV2) was last detected in Uttar Pradesh, India, in 1999 and appears to have been eradicated (7). To monitor pathways of virus transmission, GPLN sequences and analyzes the genomic region encoding the major virus surface protein (VP1) (approximately 900 nucleotides) of all wild polioviruses. Detected viruses belonged to four genotypes: South Asia (SOAS) PV1, West Africa B (WEAF-B) PV1, SOAS PV3, and WEAF-B PV3. During January 2006--June 2007, indigenous PV1 and PV3 were identified in four countries (Afghanistan, India, Nigeria, and Pakistan). Imported viruses of Nigerian origin were identified in eight countries (Cameroon, Chad, Ethiopia, Indonesia, Kenya, Niger, Somalia, and Yemen) where polio is not endemic; viruses of Indian origin were identified in six countries (Angola, Bangladesh, Democratic Republic of the Congo, Myanmar, Namibia, and Nepal) where polio is not endemic. Most of the imported virus was PV1 introduced in 2005 (five countries) or 2006 (eight additional countries). Single-case importations of PV3 of Nigerian origin were reported in 2006 in Niger (two episodes), Cameroon, and Chad. Myanmar was the only country with a newly reported PV1 importation in 2007. Detection of Vaccine-Derived PoliovirusesVaccine-derived polioviruses (VDPVs) are polioviruses with >1% VP1 nucleotide sequence difference from the parental Sabin vaccine strain of the same type. Concern has increased over the potential for VDPV epidemics since confirmation of a VDPV outbreak in Hispaniola in 2000 (8). VDPVs are subdivided into three categories: 1) circulating VDPVs (cVDPVs) with transmission resulting in more than one patient with paralysis; 2) VDPVs obtained from persons with primary immunodeficiencies (iVDPVs); and 3) ambiguous VDPVs (aVDPVs) isolated from nonimmunodeficient persons, non-AFP patient sources, or a single AFP patient whose case cannot be assigned to the other two VDPV categories (9). GPLN has screened all Sabin vaccine--related isolates from AFP cases since 1999. During January 2006--June 2007, vaccine-related isolates were observed in 7,311 specimens from AFP cases (Table 3), including 7,190 (98.3%) categorized as Sabin vaccine--like viruses† and 121 (1.7%) categorized as VDPVs; 107 VDPVs were detected during cVDPV outbreaks, 12 were iVDPVs, and two were aVDPVs. The cVDPV outbreaks occurred in Myanmar (four cases of type 1; data as of September 7, 2007) and Nigeria (66 cases of type 2; data as of September 7, 2007); in 2006, two single-case importations of VDPVs from Nigeria were reported in Niger. Four specimens from Nigeria yielded type 2 VDPV and wild poliovirus mixtures (two with wild PV1 and two with wild PV3). Two specimens from one AFP case in Cambodia in 2006 had type 3 VDPVs genetically linked to cVDPVs detected in 2005. iVDPVs were isolated from seven persons with primary immunodeficiencies during the same period. Three persons had type 2 viruses (detected in Iran, in Syria, and in France in a child of Tunisian origin), one was coinfected with types 1 and 2 VDPVs (in Iran), and three had type 3 VDPVs (in Egypt, Iran, and Kuwait). Six of the immunodeficient persons were paralyzed, and their viruses were detected through AFP surveillance; the seventh was not paralyzed and had iVDPV isolated in France during clinical investigations for a bone marrow transplant. Type 1 aVDPVs were isolated from single AFP cases in Guangxi (where seven healthy contacts also had VDPVs) and Shanxi, China. aVDPVs also were detected in non-AFP sources: a healthy child in Shanghai, China (type 3) and sewage water in Israel (type 2). GPLN InitiativesRecognizing the role of laboratories in early detection of transmission, GPLN is implementing a plan to increase the speed of poliovirus confirmation. One element of the plan is use of a new test algorithm§ that was proven through field evaluations in India, Pakistan, and the United States to decrease the time for completing laboratory analyses from 42 to 21 days without compromising poliovirus detection sensitivity. The algorithm was adopted by GPLN in June 2006, with priority given initially to the 43 laboratories located in polio-endemic regions where its use is required. These laboratories will be evaluated against new reporting targets (14 days for virus isolation and 7 days for ITD from date of arrival in the laboratory) beginning January 2008. A second goal is to increase (from 58% to 75%) by December 2007 the percentage of stool specimens from polio-endemic regions that are tested in laboratories with on-site capacity for both virus isolation and ITD. In addition, GPLN plans to expand its use of real-time polymerase chain reaction (PCR) assays to reduce the use of virus cultivation in cell culture and minimize opportunities for breaches of poliovirus containment in the laboratory. The impact of GPLN measures to reduce reporting times already is evident. During January--June 2007, approximately 80% of wild virus importations or outbreaks were detected within 21 days of paralysis onset in the first patient, compared with 50% of importations and outbreaks during the same period in 2006. Reported by: Polio Eradication Initiative Dept, WHO, Geneva, Switzerland. Div of Viral Diseases, Global Immunization Div, National Center for Immunization and Respiratory Diseases, CDC. Editorial Note:GPLN continues to provide important data to monitor progress toward polio eradication and to direct immunization and other services to areas of greatest need. During 2006--2007, GPLN identified specific areas in Nigeria and India as the ultimate sources of wild poliovirus transmission occurring elsewhere, underscoring the need to interrupt transmission in these areas to avoid jeopardizing the polio-free status of other countries. High vaccination coverage must be achieved and maintained in all WHO regions to prevent circulation of endemic or imported wild poliovirus or VDPVs. The recent outbreak of cVDPV in Nigeria has implications for the GPLN procedure for VDPV detection. All poliovirus isolates are screened using two complementary ITD tests (usually enzyme-linked immunosorbent assay [ELISA] using specific cross-absorbed antisera and diagnostic PCR using strain-specific reagents). Isolates with discordant results from the two tests are flagged for sequencing for definitive identification of VDPVs. Follow-up clinical and epidemiologic investigations are used to categorize the VDPVs (i.e., as cVDPVs, iVDPVs, or aVDPVs). This approach has successfully identified cVDPV outbreaks in five countries (Cambodia, China, Indonesia, Myanmar, and the Philippines) since 2000 but failed to flag multiple type 2 VDPVs from Nigeria and type 2 and type 3 VDPVs from Madagascar (in 2001 and 2005) because they reacted as Sabin vaccine--like in both ITD tests (ELISA and PCR). In Nigeria, sequencing was performed because the temporal and geographic clustering of type 2 Sabin vaccine--like isolates suggested virus circulation. In Madagascar, the viruses had profiles that were not Sabin vaccine--like in a PCR-restriction fragment length polymorphism assay used in a multilaboratory collaborative study of Sabin vaccine--related polioviruses (10). Although the GPLN screening procedure appears successful in detecting type 1 VDPVs, recent evidence suggests that it lacks sufficient sensitivity for detection of type 2 and type 3 VDPVs. A real-time PCR assay developed at a Global Specialized Laboratory appears to increase VDPV detection sensitivity for all types and is being evaluated for use by GPLN. GPLN contributes to the expanding understanding of factors related to the occurrence and spread of VDPVs. GPLN detected several VDPVs in middle- and low-income countries where follow-up investigations led to diagnoses of underlying primary immunodeficiency conditions. Investigators have observed no evidence of prolonged iVDPV excretion or virus spread to family contacts from those patients. The two cases in Niger demonstrate the potential for importation of VDPVs from areas where they circulate. In Nigeria, four persons excreted both wild poliovirus and VDPV, documenting that coinfection can occur where the viruses cocirculate. Additionally, several Nigerian PV2 viruses had five to nine VP1 nucleotide differences from Sabin vaccine virus type 2, with some mutations shared with isolates classified as VDPV, suggesting they are directly ancestral to the VDPVs. The definition of VDPV might need revision to accommodate such observations. Greater testing volume, ongoing measures to reduce reporting times in polio-endemic regions, and the need to maintain laboratory support in polio-free regions are the major challenges facing GPLN. Because the newly introduced test algorithm initially places additional burdens (e.g., added complexity and increased costs) on laboratories, WHO is mobilizing the additional necessary resources for GPLN. However, faster confirmation of poliovirus enables more rapid targeted interventions to prevent virus spread, which should reduce the overall costs of immunization programs. More laboratories in polio-free areas are expected to adopt the new algorithm for early detection of VDPVs and wild poliovirus importations. Because of the continuing need for global poliovirus surveillance, WHO continues to advocate with national authorities and partner agencies for continued support for GPLN. References
* Some laboratories also test specimens or isolates collected from non-AFP patient sources (e.g., non-AFP patients, healthy children, and sewage). † Sabin vaccine--like polioviruses are those with either concordant Sabin vaccine--like results in ITD tests or <1% sequence difference when compared with Sabin vaccine virus. The presence of a Sabin vaccine--like poliovirus usually is indicative only of coincidental receipt by a person with AFP of the Sabin oral poliovirus vaccine, which is rarely the cause of the AFP. § Available at http://www.who.int/immunization_monitoring/Supplement_polio_lab_manual.pdf.
Table 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/19/2007 |
|||||||||
|