 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Status of the Global Laboratory Network for Poliomyelitis Eradication, 1994-1996In 1988, the World Health Assembly adopted the goal of global poliomyelitis eradication by the year 2000 (1). Since then, appropriate strategies have been developed, and substantial progress toward the implementation of these strategies has been reported from each region of the World Health Organization (WHO) (2,3). The establishment of sensitive surveillance systems to detect polio cases and poliovirus is critical to guide program activities and eventually permit the certification of polio eradication. This report describes the proficiency of the global laboratory network, which operates in each WHO region and provides virologic laboratory support to all countries with endemic polio. The WHO Global Laboratory Network comprises 67 national laboratories, 14 regional reference laboratories, and six specialized reference laboratories (Figure_1). The national laboratories process stool specimens from cases of acute flaccid paralysis (AFP) to detect poliovirus and identify serotypes. The regional reference laboratories confirm the identity of polioviruses isolated by national laboratories and determine whether the viruses are wild or vaccine-derived. The specialized reference laboratories develop and distribute virus reference reagents, prepare training materials, organize workshops, offer extended bench training, collaborate on special surveillance studies, and conduct research to improve the methods of virologic surveillance. These laboratories also perform genomic sequencing of epidemiologically important polio-viruses. The sequence information can be used to distinguish between imported and indigenous polioviruses, estimate the temporal link between cases, identify reservoirs sustaining poliovirus endemicity, track chains of virus transmission, and recognize potential laboratory contaminants (4). To ensure the quality of the laboratory network, in 1996 an annual accreditation program was initiated to be completed by all national and regional laboratories by the end of 1997. Six criteria are used for accreditation: 1) completeness and timeliness of reporting; 2) minimum number of specimens tested; 3) nonpolio enterovirus isolation rate of greater than or equal to 10% from all stool specimens; 4) accuracy of poliovirus detection and identification; 5) scores from annual proficiency tests; and 6) score from an annual on-site review of laboratory operating procedures and practices. The laboratory network must have the capacity and capability to process a minimum of 26,000 stool specimens per year, based on the expected occurrence of at least one case of nonpolio AFP per 100,000 population aged less than 15 years. To assess the quality of performance, during 1994-1996, a total of 100 proficiency tests were completed by the 67 national laboratories in five of the eight WHO regions. The proficiency test panels were prepared by the National Institute of Public Health and Environmental Protection (RIVM) in Bilthoven, Netherlands, and consisted of five stool samples containing zero, one, two, or three poliovirus serotypes and/or nonpolio enteroviruses. Correct results were obtained for 332 (66%) of the 500 total samples. Of the samples containing one poliovirus type, 90% were correctly identified; of the samples containing two poliovirus types, 71% were correctly identified; and of the samples containing three poliovirus types, 33% were correctly identified. Of the 168 (34%) samples with incorrect results, 26% were caused by errors in virus isolation or typing and 8% by virus contamination of negative samples or cross-contamination of virus-containing samples. Samples containing any poliovirus, regardless of the number or type, were identified with a sensitivity and specificity of 92% and 91%, respectively. For all national and regional laboratories, the goal of proficiency testing is a score of greater than or equal to 80%. In the 1997 proficiency tests, each of the 30 provincial laboratories in China scored 100%. All regional reference laboratories scored 100% on the most recent panels designed to test the proficiency in distinguishing wild from vaccine-derived polioviruses. Reported by: Global Program for Vaccines and Immunization, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Polio Eradication Activity, National Immunization Program, CDC. Editorial NoteEditorial Note: Polio eradication depends on effective global surveillance to guide vaccination strategy, verify outcome, and certify success. Surveillance consists of detecting, reporting, and investigating all cases of AFP in patients aged less than 15 years or suspected polio cases in patients of any age, collecting stool specimens from each patient for testing in the laboratory, and reporting the virologic findings to national immunization managers. An essential component of surveillance is a global network of high-quality laboratories capable of detecting wild poliovirus. Building the network began in 1986 in the Americas (4) -- the first region to declare its intention to eradicate polio
Effective surveillance for polio begins in the field and requires early detection of AFP cases, collection of specimens within 2 weeks of onset of AFP, prompt shipment of specimens on ice to the laboratory, and prompt reporting of laboratory results. Maintaining an effective poliovirus surveillance system is a dynamic process, requiring regular review of training and resource needs for optimal performance. Organizations supporting continued development of the surveillance system include Rotary International, the Japanese International Cooperation Agency, the U.S. Agency for International Development, and other partner organizations. The Polio Plus Partners Program of Rotary International, through the donations of individual clubs and districts to assist individual laboratories, also contributes support to polio surveillance. The 1994-1996 proficiency test results are an indication of the range of capabilities of national laboratories and serve as a basis for further improvement, particularly by newer and less-experienced laboratories. Samples containing more than one poliovirus type or a poliovirus and nonpolio enterovirus mixture caused the greatest difficulty, skewing the scores downward. However, samples containing more than one poliovirus or a mixture of polioviruses and nonpolio enteroviruses may not be routinely encountered in poliovirus surveillance. Of the proficiency testing samples, 45% contained more than one virus; of stool specimens from AFP cases, 5%-20% can be expected to contain more than one virus, depending on the prevalence of virus in the community or the recent administration of trivalent oral poliovirus vaccine. Proficiency testing samples with one or more polioviruses were identified as containing poliovirus with a sensitivity and specificity of 92% and 91%, respectively. In practice, the identification of poliovirus in a sample is sufficient cause to ship the isolate to a regional reference laboratory, where virus mixtures can be separated and characterized using additional tests. WHO is committed to further enhancing laboratory proficiency through the introduction of a poliovirus-specific cell substrate, improvement of procedures, and continued training. The results of the 1997 network-wide process of laboratory accreditation will provide additional assessment of progress in national and regional poliovirus surveillance. The role of the laboratory network becomes increasingly important as progress is made toward polio eradication. The laboratory network in the Americas monitored the successive elimination of the eight distinct wild poliovirus genotypes indigenous to the Americas (7), which culminated in the reporting of the last case in 1991 (8). The polioviruses that had been indigenous to China were last detected in 1994 (9), and wild poliovirus type 2 is nearing extinction. References
Figure_1 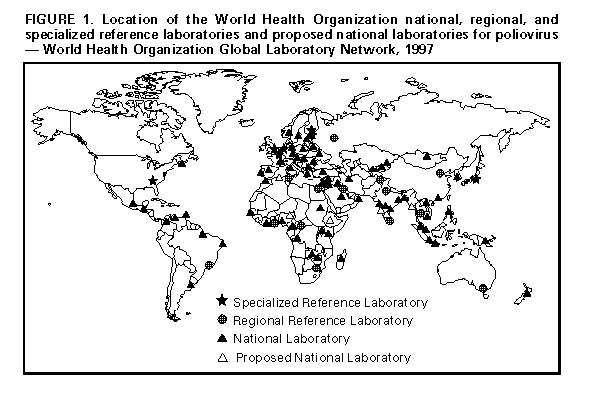 Return to top. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 09/19/98 |
|||||||||
This page last reviewed 5/2/01
|
{kind=link}