|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
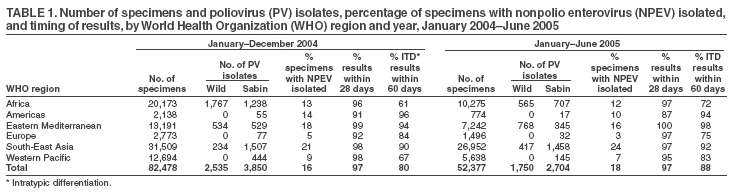
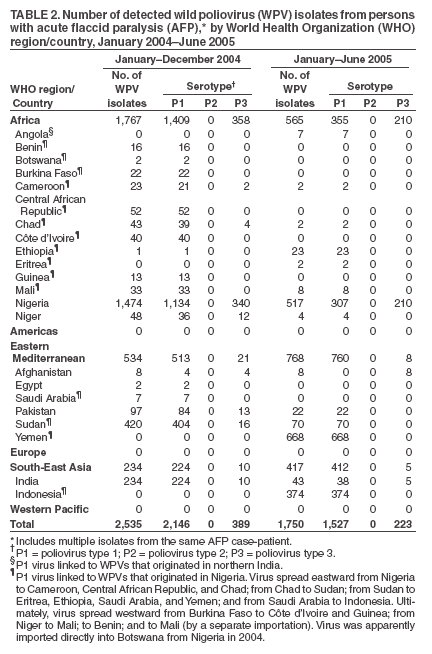
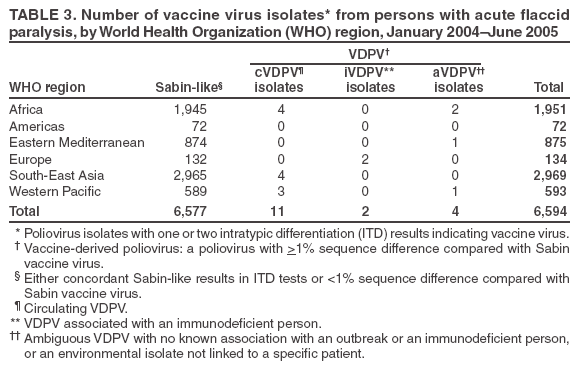
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Laboratory Surveillance for Wild and Vaccine-Derived Polioviruses, January 2004--June 2005A global network of 145 virology laboratories has been established by the World Health Organization (WHO) to support surveillance activities of the Polio Eradication Initiative (PEI). The Global Polio Laboratory Network analyzes stool specimens from patients with acute flaccid paralysis (AFP) and environmental samples for the presence of polioviruses. Surveillance systems detect at least one AFP case per 100,000 persons aged <15 years, collect adequate stool samples* from patients, and send the samples to network laboratories for analysis. Laboratory data are used to identify locations where wild polioviruses (WPVs) or vaccine-derived polioviruses (VDPVs) are circulating, target supplementary immunization activities (SIAs) to interrupt transmission chains, and investigate genetic relationships among viral isolates. This report updates previous publications (1--3) and describes the laboratory network's performance during the period January 2004--June 2005. Laboratory Network PerformanceThe Global Polio Laboratory Network operates in all six WHO regions and includes 123 National Laboratories, 15 Regional Reference Laboratories, and seven Global Specialized Reference Laboratories. High-quality performance is ensured through a WHO-administered laboratory accreditation program that evaluates network laboratories for proper procedures, accuracy, and timeliness of reporting. Ninety-seven percent of network laboratories were fully accredited by WHO in 2004. Samples from nonaccredited laboratories are referred and tested in parallel in accredited laboratories to ensure that reliable virology results are available for program use. During January 2004--June 2005, the laboratory network tested 134,855 stool samples, an increase of 37% over the previously reported comparable 18-month period (1). Approximately 97% of samples had virus isolation results available within 28 days of receipt of samples in laboratories (program target: >80% within 28 days) (Table 1). For 83% of AFP cases with poliovirus isolates, the results of intratypic differentiation (ITD) tests confirmed either the wild or vaccine-like nature of isolates within 60 days of paralysis onset (program target: >80% within 60 days). However, this target was not achieved in all WHO regions during the 18-month period. Detection of WPV SerotypesIndigenous WPV type 2 circulation appears to have been eradicated and was last detected in western Uttar Pradesh, India, in October 1999 (Table 2) (4,5). Wild polioviruses were confirmed in 22 countries during January 2004--June 2005. Viruses of only serotype 1 were detected in 14 countries (Angola, Benin, Botswana, Burkina Faso, Central African Republic, Côte d'Ivoire, Egypt, Eritrea, Ethiopia, Guinea, Indonesia, Mali, Saudi Arabia, and Yemen). Polioviruses of both serotypes 1 and 3 were detected in Afghanistan, Cameroon, Chad, India, Niger, Nigeria, Pakistan, and Sudan. Detection of WPV GenotypesThe Global Polio Laboratory Network routinely generates VP1 sequences of 1) all WPVs and 2) all isolates that give inconclusive results on ITD tests. Sequences are analyzed to identify virus genotypes and investigate transmission links among viruses from diverse locations. Seven WPV genotypes were detected during January 2004--June 2005, including three type 1 genotypes (NEAF, WEAF-B, and SOAS) and four type 3 genotypes (WEAF-B, SOAS, CEAF, and EAAF). The NEAF genotype was detected only in Egypt. The SOAS genotypes were detected in Afghanistan, Angola (type 1 only), Pakistan, and India. The type 1 WEAF-B genotype was detected in 10 countries in west and central Africa as well as Botswana, Eritrea, Ethiopia, Indonesia, Saudi Arabia, Sudan, and Yemen. The type 3 WEAF-B genotype was detected in Cameroon, Niger, and Nigeria. In 2004, the type 3 EAAF and CEAF genotypes were detected in Sudan and Chad, having previously been detected during 1999 and 1996, respectively. Indigenous WPVs were detected in Afghanistan, Egypt, India, Pakistan, Niger, and Nigeria in 2004 and 2005. Indigenous type 3 viruses were detected in Chad and Sudan in 2004, although these were isolated from only 2% and 9%, respectively, of all reported cases from those countries (the remainder were from reestablished transmission of imported type 1 viruses). The type 1 virus detected in Angola in 2005 was an importation from northern India. Type 1 viruses in countries of east, west, and central Africa, Botswana, Indonesia, Saudi Arabia, and Yemen were linked, often through intermediate countries, to indigenous viruses of northern Nigeria. Detection of Vaccine VirusesVaccine viruses isolated from stool specimens or environmental samples are characterized as Sabin-like (SL) vaccine viruses or as VDPVs; during January 2004--June 2005, a total of 6,577 of 6,594 (99.7%) vaccine viruses were SL (Table 3). AFP cases with isolation of SL vaccine viruses are evaluated through detailed epidemiologic investigation and by National Expert Review Committees for the possibility of vaccine-associated paralytic poliomyelitis. VDPVs are defined as viruses with >1% sequence difference compared with Sabin vaccine virus of the same serotype. VDPVs are further categorized as 1) circulating VDPVs (cVDPVs) when evidence exists of person-to-person transmission, 2) immunodeficiency-associated VDPVs (iVDPVs) when isolated from immunodeficient persons (usually without secondary spread), and 3) ambiguous VDPVs (aVDPVs) when insufficient evidence exists of circulation or connection to an immunodeficient patient or the virus is from a source (e.g., environmental sample) that is not from a specific patient. Circulating VDPVs have been detected previously in Egypt, Hispaniola, the Philippines, and Madagascar (6--9). Type 1 cVDPV outbreaks were detected in 2004 in China, where isolates were obtained from two AFP patients and three contacts from Guizhou Province, and in 2005 in Indonesia, where two cases with paralysis onset before June 30 were confirmed and an additional 10 cases with later onset have been confirmed through ongoing investigations. Type 2 VDPVs were also isolated from single AFP cases in Lao People's Democratic Republic in 2004 and in Hong Kong and Saudi Arabia in 2005. Type 2 VDPV and type 3 cVDPV outbreaks are being investigated in Madagascar; type 3 cVDPVs have been confirmed in one AFP case and eight contacts in Madagascar in 2005. VDPVs from non-AFP sources also have been reported by network laboratories. Type 2 VDPVs are detected most frequently and have been isolated intermittently from sewage waters in Slovakia (during October 2003--February 2005), Egypt (from a single sewage sample in 2005), and Israel (intermittently during 2004--2005) (10). Follow-up investigations in Slovakia and Israel have not revealed paralytic cases nor identified the source of the VDPVs. A type 2 VDPV was isolated from a healthy child as part of a stool-specimen survey in Japan in 2004. Type 3 VDPVs were isolated in 2005 in Japan from a paralyzed adult and from a child vaccinated in the same household. The VDPVs from Slovakia and Israel are highly divergent from Sabin 2 (i.e., >10% VP1 differences), whereas the VDPVs from Egypt and Japan are much less divergent (i.e., <2% VP1 differences from the parental Sabin strain), consistent with less than 2 years of replication. Reported by: Immunization, Vaccines and Biologicals Dept, WHO, Geneva, Switzerland. Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Global Immunization Div, National Immunization Program, CDC. Editorial Note:The Global Polio Laboratory Network provides support to the PEI by 1) monitoring the extent of WPV circulation in endemic areas, 2) identifying reservoir communities sustaining WPV endemicity, 3) identifying the source of imported WPVs, 4) monitoring for the presence of WPVs and VDPVs in the environment, 5) identifying gaps in AFP surveillance from the extent of genetic divergence among the most closely related isolate pairs, and 6) characterizing VDPVs and investigating the factors contributing to their emergence. During 2004--2005, the number of countries with circulating WPVs increased because of the eastward spread of WPV type 1 from Nigeria to Cameroon, the Central African Republic, Chad, Sudan, Saudi Arabia, Yemen, Ethiopia, Eritrea, and Indonesia, and the importation of WPV type 1 from India (Uttar Pradesh) to Angola. In 2005, the number of cases caused by reestablished transmission of imported viruses exceeded for the first time the number of cases in remaining countries where WPVs are endemic. The larger outbreaks associated with this spread and intensified surveillance activities have increased the workload within the laboratory network. PEI responded to this challenge by providing increased logistical support and redistributing the workload, increasing the number of laboratories that perform both virus isolation and ITD in the same facility. Network laboratories with the most increased workloads have responded by implementing double work shifts and 7-day work weeks, streamlining procedures, and incorporating new rapid technologies (e.g., diagnostic polymerase chain reaction and hybridization in key National Laboratories and implementation of genomic sequencing in key Regional Reference Laboratories). Prominent in their effective responses to the increasing workloads are the National Laboratories in Nigeria (Ibadan and Maiduguri), Sudan, Oman, Indonesia (Bandung), and India (Lucknow); the Regional Reference Laboratories in South Africa, Pakistan, and Egypt; and the Global Specialized Reference Laboratory in India (Mumbai). Other network laboratories have continued to improve their performance. Studies in network laboratories in Madagascar and France, Slovakia and Finland, Indonesia and India, China, Egypt, Japan, Israel, and the United Kingdom have detected VDPVs. Of greatest concern are the detection of two independent cVDPV outbreaks (one type 2 and the other type 3) in Madagascar and the outbreak of type 1 cVDPV in Indonesia. The recent detections of type 3 VDPVs represent the first reports of VDPVs from this serotype in more than 30 years. Nonetheless, despite intensive surveillance, the incidence of VDPVs is currently much lower than that of WPVs. The genetic and antigenic characterization of the recent VDPV isolates will contribute to the refinement of laboratory methods for the detection of VDPVs. In this final stage of the PEI, the time between onset of an AFP case, identification of an association with poliovirus, and implementation of an effective immunization response must be as short as possible. A high priority for the laboratory network in coming months will be evaluating technologies and procedures that have the potential to substantially reduce the time for poliovirus identification. Maintenance and necessary enhancement of network performance will require continued commitment and support from WHO and its partners.† References
* At least 2 stool samples are collected, 1--2 days apart and within 14 days of paralysis onset. † Major contributors to the PEI include Rotary International, Department for International Development of the United Kingdom, U.S. Agency for International Development (USAID), European Commission, Canadian International Development Agency, World Bank, Bill and Melinda Gates Foundation, United Nations Foundation, Sanofi-Pasteur, International Federation of Pharmaceutical Manufacturers and Associations, national governments of Australia, Denmark, France, Germany, Italy, Japan, the Netherlands, Norway, the Russian Federation, and Sweden, and CDC.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/29/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|