|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
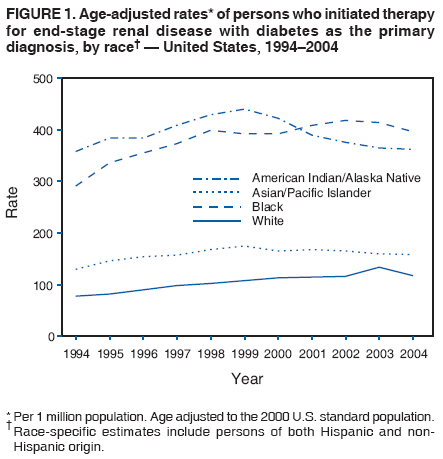
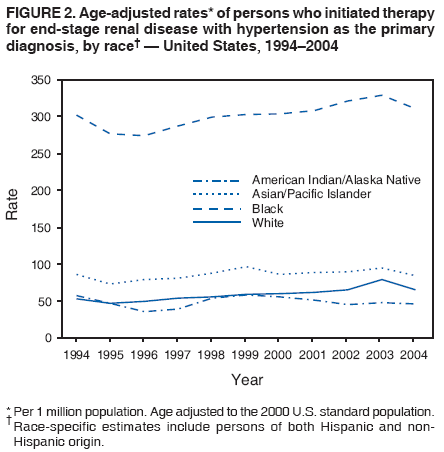
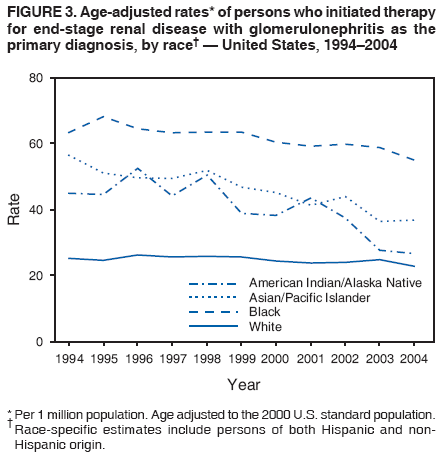
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Racial Differences in Trends of End-Stage Renal Disease, by Primary Diagnosis --- United States, 1994--2004The leading cause of end-stage renal disease (ESRD) (i.e., kidney failure requiring dialysis or transplantation) in the United States is diabetes, followed by hypertension and glomerulonephritis (1). These three conditions accounted for approximately 80% of new cases of ESRD treated during 2004 (1). This report presents an analysis of data from the United States Renal Data System (USRDS) to examine trends in the primary diagnosis of ESRD in the United States. The findings of that analysis indicated that, during 1994--2004, ESRD incidence attributed to glomerulonephritis decreased among all races analyzed. During 1999--2004, ESRD incidence attributed to diabetes or hypertension also decreased for American Indians/Alaska Natives (AI/ANs) and Asians/Pacific Islanders (A/PIs) but not for whites or blacks.* Continued interventions, such as those addressing blood-glucose and blood-pressure control (2,3), are needed to reduce the prevalence of these risk factors for kidney failure (4) and to improve care among persons with these conditions. USRDS, with administrative oversight by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health (NIH), collects, analyzes, and distributes information from clinical and claims data reports to the Centers for Medicare and Medicaid Services (CMS) regarding patients being treated for ESRD. Through the ESRD entitlement program, Medicare reimburses most of the total cost of ESRD treatment in the United States (1). USRDS collects demographic and clinical data, including the date patients were first treated and the primary diagnosis, on all ESRD patients and includes data for approximately 93% of persons with ESRD in the United States (1). Primary diagnosis (i.e., primary cause of renal failure) is taken from the CMS Medical Evidence Report, which is completed by the renal-care provider for each new ESRD patient and is based on the physician's assessment of the patient. The 1994--2004 USRDS data were used to determine the number of persons in the United States who began treatment (i.e., dialysis or kidney transplantation) for ESRD with diabetes, hypertension, or glomerulonephritis listed as the primary diagnosis. Incidence rates were calculated using race-specific population estimates from the U.S. census and were age adjusted based on the 2000 U.S. standard population. The total number of persons who began treatment for ESRD increased from 68,757 in 1994 to 102,356 in 2004. Of the new cases reported in 1994, a total of 26,848 (39%) had diabetes listed as the primary cause of renal failure, 21,270 (31%) had hypertension, and 8,213 (12%) had glomerulonephritis. In 2004, a total of 44,953 (44%) of the new cases were attributed to diabetes, 27,910 (27%) to hypertension, and 8,352 (8%) to glomerulonephritis. Overall, ESRD incidence increased from 261.3 per million population in 1994 to 348.6 in 2004. During 1994--2004, age-adjusted ESRD incidence with diabetes listed as the primary diagnosis was higher among blacks and AI/ANs than among whites and A/PIs (Figure 1). During this time, age-adjusted ESRD incidence among whites increased from 77.6 to 117.1 per million population. However, among blacks, incidence increased from 291.0 to 399.1 per million population during 1994--1998 and then leveled off during 1999--2004. Among AI/ANs, age-adjusted ESRD incidence increased from 358.6 per million population in 1994 to a peak of 440.4 in 1999; by 2004, incidence had decreased to 362.4 per million. Similarly, among A/PIs, incidence increased from 130.1 to 175.1 per million population during 1994--1999 and subsequently decreased to 158.8 in 2004. During 1994--2004, ESRD incidence with hypertension listed as the primary diagnosis was at least three times higher among blacks than among the other three racial populations (Figure 2). During 1994--2004, age-adjusted ESRD incidence increased from 53.4 to 65.6 per million population among whites, but increased less among blacks, from 302.2 to 310.7. Incidence among A/PIs decreased slightly, from 86.0 to 84.2 per million population. Although no clear trends among AI/ANs were detected before 1999, incidence of hypertension-related ESRD decreased from 58.1 to 45.8 per million population during 1999--2004. ESRD incidence with glomerulonephritis listed as the primary diagnosis also was highest among blacks compared with other racial populations (Figure 3). During 1994--2004, age-adjusted ESRD incidence decreased for all races: from 63.5 to 55.0 per million population among blacks, from 56.7 to 36.8 among A/PIs, from 45.1 to 26.7 among AI/ANs, and from 25.2 to 22.8 among whites. Reported by: D Gilbertson, PhD, Chronic Disease Research Group, United States Renal Data System Coordinating Center, Minneapolis, Minnesota. NR Burrows, MPH, J Wang, D Rolka, MS, LS Geiss, MA, DE Williams, MD, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:ESRD is a costly and disabling condition associated with a high mortality rate. Among patients aged >65 years who were receiving dialysis, overall mortality rates in 2004 were seven times greater than among persons in the general Medicare population (1). Risk factors for ESRD include diabetes and hypertension (4). The findings in this report indicate some encouraging trends in ESRD incidence rates. Among all racial populations, ESRD incidence attributable to glomerulonephritis declined during 1994--2004. Among AI/ANs, the incidence of ESRD attributable to diabetes, hypertension, or glomerulonephritis decreased during 1999--2004. Moreover, the decline in diabetes-related ESRD incidence among AI/ANs, despite the increasing diabetes prevalence in this population (5), suggests that diabetes management has improved and the prevalence of other risk factors has decreased. Among A/PIs, ESRD incidence attributable to diabetes and glomerulonephritis also declined during 1999--2004. Reasons for these trends cannot be determined from surveillance data but might include a reduction in the prevalence of risk factors for kidney failure (6,7) as a result of early detection or better treatment with new pharmacologic agents, such as angiotensin-converting enzyme inhibitors and angiotensin-receptor blockers. Both of these agents have been determined to be renoprotective, independent of their ability to reduce blood pressure (8). Continued awareness and interventions (e.g., blood-glucose and blood-pressure control [2,3]) to reduce the prevalence of these risk factors and improve care among persons with diabetes or hypertension are needed to sustain and improve trends in ESRD incidence. Additional strategies are needed to decrease ESRD incidence attributable to diabetes or hypertension among blacks and whites because ESRD incidence in these populations did not decrease during 1999--2004 as it did among AI/ANs and A/PIs. The findings in this report are subject to at least four limitations. First, data were collected for persons whose ESRD treatment was reported to CMS; persons who died from ESRD before receiving treatment, persons who refused treatment, and persons whose treatment was not reported to CMS were not included. Second, primary diagnosis was taken from the CMS Medical Evidence Report and was based on the physician's assessment of the patient, which might have affected trends, especially if patients had comorbid conditions. Furthermore, primary diagnosis might be influenced by the physician's awareness of prevalent conditions in certain populations, such as diabetes among AI/ANs (6) or hypertension among blacks (9). Third, racial misclassification in USRDS data might have affected the magnitude of the rates in specific populations, although trends would not be affected if the bias remained constant over time. Finally, ESRD incidence among Hispanics was not analyzed because USRDS racial categories do not include ethnicity; however, during 1997--2002, age-adjusted ESRD incidence attributable to diabetes among Hispanics did not change (10). CDC provides resources and technical assistance to diabetes-control programs in all 50 states, eight territories, and the District of Columbia (DC) for 1) educating persons about diabetes, 2) improving and monitoring the quality of diabetes care, and 3) promoting early detection of diabetes complications. CDC also funds health departments in 32 states and DC to develop effective strategies for reducing the effects of heart disease and stroke and their risk factors, such as high blood pressure. The National Diabetes Education Program (NDEP) campaign, Be Smart About Your Heart: Control the ABCs of Diabetes, addresses risk factors for ESRD among persons with diabetes, such as poorly controlled hyperglycemia, hypertension, and hyperlipidemia (http://www.ndep.nih.gov/campaigns/besmart/besmart_index.htm). NDEP is sponsored by CDC and NIH and aims to educate the public about controlling diabetes and preventing its complications. In March 2006, NDEP launched the first Survey of Public Attitudes, Knowledge, and Practices Related to Diabetes, and the survey findings indicated that most people with diabetes report that they are taking steps to manage their disease; 81% check their own blood-glucose levels, 61% keep records of their blood-glucose test results, and 61% have had their hemoglobin A1c levels tested one or more times in the past year (http://www.ndep.nih.gov/new/nltr/2007/programupdatewinter2007.pdf). Another NIH-sponsored program, the National Kidney Disease Education Program (http://www.nkdep.nih.gov), aims to raise public awareness about kidney disease, the importance of testing for kidney disease among those at risk, and the availability of treatment to prevent or slow kidney failure. In addition, the National Kidney Foundation offers the Kidney Early Evaluation Program (http://www.kidney.org/news/keep/index.cfm), a free health-screening program for persons at increased risk for kidney disease. CDC will continue to work with public and private partners to reduce rates of diabetes and other risk factors for kidney failure and improve care of persons with these conditions. Continued surveillance of ESRD using USRDS data will help public health officials monitor and assess progress in reducing ESRD and its risk factors. In addition, CDC is collaborating with partners at Johns Hopkins University and the University of Michigan to develop a national surveillance system for kidney disease. References
* USRDS categories do not include ethnicity (Hispanic or non-Hispanic origin); thus, race-specific estimates include persons of both Hispanic and non-Hispanic origin.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/22/2007 |
|||||||||
|