|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
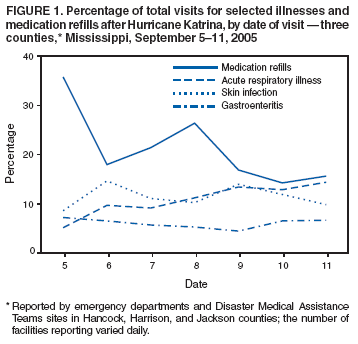
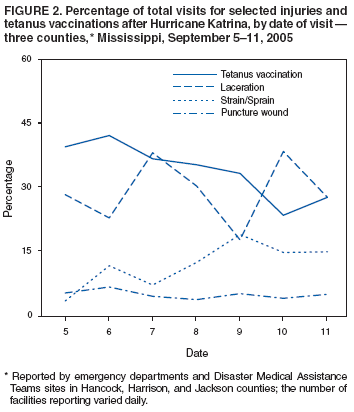
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Surveillance for Illness and Injury After Hurricane Katrina --- Three Counties, Mississippi, September 5--October 11, 2005Hurricane Katrina made landfall on the U.S. Gulf Coast on August 29, 2005, resulting in massive destruction from wind damage and storm surge. In Mississippi, the storm surge was an estimated 27 feet high at the Hancock County Emergency Operations Center and extended inland for 6--12 miles, causing extensive flooding in Biloxi and Gulfport and rendering approximately 80% of buildings in Waveland uninhabitable (1). The devastation was greatest in the coastal counties of Hancock, Harrison, and Jackson, where public infrastructure (e.g., electric power, communications networks, roads, sanitation systems, and water treatment plants) was severely disrupted. Multiple hospitals, health clinics, and public health facilities were either destroyed or nonfunctioning immediately after the hurricane. The Mississippi Department of Health (MDH) asked CDC to help conduct active surveillance at hospital emergency departments (EDs), federal Disaster Medical Assistance Team (DMAT)* operation sites, and outpatient health-care facilities in Hancock, Harrison, and Jackson counties. On September 4, a team of 17 CDC staff members was deployed to Mississippi to work with MDH and an Epi Strike Team from the Florida Department of Health to provide surveillance for injury and illness (2). This report describes those surveillance activities and their findings, which determined that no major outbreaks of infectious illnesses or clusters of preventable major injuries occurred after the hurricane. However, daily reports to MDH provided reassurance regarding outbreaks and data to help direct public health activities in the affected region. Data were collected from a total of 15 EDs, DMATs, and outpatient health-care facilities in two phases, using two different systems. The number of facilities reporting varied daily; a maximum of 15 total facilities, including eight DMATs, were included in the reporting. During September 5--11, individual patient data were collected from each facility and entered into a database. Data collection was limited to the following variables that were consistently available: medical record number, sex, age, illness/injury diagnostic category, severity, disposition, and comments. Data were collected from patient ED records, paper logs of ED/DMAT visits, or electronic records of visits to the one facility equipped with electronic medical record-keeping. For each patient visit, an injury or illness diagnostic category for reason of visit was assigned by a reviewing epidemiologist, using both chief-complaint data and discharge diagnoses from the patient record and diagnostic categories from a standard injury and illness surveillance form designed by CDC. Data were forwarded to MDH in Jackson to create daily reports on illness and injury trends for MDH staff, reporting facilities, and CDC in Atlanta. By September 10, DMAT operations had begun to scale down, shifting health-care services to operating EDs. As patient volumes declined and no major outbreaks of infectious disease were identified, the surveillance team simplified its system. On September 12, the team began collecting aggregate data by using a tally-based system that focused on 16 categories of syndromes† selected from illnesses and injuries most commonly observed during the first surveillance phase and conditions considered to be of greatest public health importance on the basis of severity, communicability, and preventability. Hospitals and DMATs faxed or e-mailed a daily tally sheet to MDH, where it was analyzed and reported back to the sites and CDC. Operation of this tally-based system was transferred to MDH on September 24 and continued until mid-October, when baseline surveillance activities were resumed gradually. During September 5--11, active surveillance data from 11,424 patient visits were reported daily from up to 15 facilities, an average of 1,632 visits per day. For the 10,999 visits with patient information available, 5,614 (51.0%) patients were female. At one facility, which included both an ED and a DMAT on site and where complete electronic patient records were recorded by the surveillance system, 2,235 patient visits were recorded during the 1-week period. This total was 83.6% greater than the number of visits to the same ED (1,217) during the 1-week period before the hurricane. Of the 10,047 patient visits for which disposition information was available, 376 (3.7%) patients were admitted, and five (0.05%) died. Of the 11,424 visits for which the reason for visit was known, 6,550 (57.3%) were for illness (including 1,394 for medication refills only), and 4,391 (38.4%) were for injury (including 1,324 for tetanus vaccination with no further injury description). Trends in the most common types of illnesses (i.e., gastrointestinal, acute respiratory, and skin infection/rash illness) were stable. Among illness visits, medication refills accounted for a decreasing proportion of visits during the 1-week period (Figure 1). Among injury visits, the proportion of visits for lacerations decreased and strains/sprains increased during the 1-week period (Figure 2). Five nonfatal post-hurricane carbon monoxide (CO) poisonings were detected by this surveillance system. During the period after active surveillance, September 12--October 11, a total of 27,135 visits were reported from EDs, DMATs, and outpatient clinics, an average of 904 per day; 1,196 (4.4%) patients were children aged <5 years. Facility reporting varied, with seven to 13 facilities reporting daily. Among visits during this period, the greatest proportion, 5,907 (21.8%), were for injuries. Major injuries accounted for 497 (8.4%) of the total injuries; minor injuries accounted for 5,410 (91.6%). The most common illnesses were skin/wound infections (1,858 [6.8%]), followed by 1,769 (6.5%) upper respiratory infections, 1,212 (4.5%) rashes and insect stings/bites, and 761 (2.8%) lower respiratory infections. Among gastrointestinal conditions, nausea/vomiting was the most common syndrome (743 [2.7%]), followed by watery diarrhea (288 [1.1%]), and bloody diarrhea (16 [0.1%]). A total of 675 (2.5%) visits were for mental health concerns; 43 suicide attempts were reported. In addition, 13,655 (50.3%) were categorized as other illness. Although visits for particular conditions varied daily, no trends or outbreaks were noted. Reported by: KM McNeill, MD, PhD, P Byers, MD, T Kittle, MPH, S Hand, J Parham, MD, L Mena, MD, Mississippi Dept of Health. C Blackmore, DVM, PhD, A Rowan DrPH, JM Kintz, MPH, D George, Epi Strike Team, Florida Dept of Health. RL Moolenaar, MD, R Shults, PhD, J Montgomery, PhD, C Shepard, MD, C Wright, M Kuehnert, MD, L Newman, MD, T Doyle, MPH, G Mootrey, DO, R Burger, J Bertulfo, MPH, G Koops, MPH, Director's Emergency Operations Center; E Stern, MD, M Breiding, PhD, L Burwell, MD, K Cain, MD, D Chang, MD, A Cohn, MD, T Finkbeiner, MD, S Jain, MD, H Jordan, MD, J Liang, DVM, E Melius, MPH, C Rao, ScD, F Soud, PhD, K Uhde, PhD, D Van Sickle, PhD, EIS officers, CDC. Editorial Note:In the immediate aftermath of Hurricane Katrina, visits to hospital EDs in the three southernmost counties of Mississippi likely increased; at the one facility with available pre-hurricane data, visits increased approximately twofold. This burden on a damaged health-care infrastructure was partially shifted to DMATs, which were able to fill the role of certain facilities rendered inoperable by the storm. The most common health-care visits to EDs and DMATs in the immediate post-hurricane period were for minor injuries, primarily puncture wounds, lacerations, strains, and sprains. Among initial noninjury visits, acute respiratory illness, gastroenteritis, and skin infections were among the most common diagnoses. Many persons visited health-care facilities for tetanus vaccination, and records did not always indicate whether associated injuries were present. A large proportion of persons also sought medication refills without other reported illnesses. Pre-hurricane preparations might reduce the post-hurricane burden on health-care systems by 1) improving tetanus booster vaccination coverage, 2) communicating to residents that tetanus vaccination is not required after disasters, and 3) encouraging residents to maintain emergency travel medical kits with supplies of critical medications. The surveillance team conducted follow-up on cases of reported infection with Vibrio spp. and clusters of respiratory and diarrheal illness (3). Similar to reports from Louisiana after Katrina (4) and from Florida after Hurricane Andrew (5), no community-associated outbreaks of infectious disease were reported in Mississippi after Katrina. Unlike Alabama and Louisiana, Mississippi had few cases of post-hurricane CO poisoning (6). The strengths of the surveillance systems described in this report included their capability to obtain large amounts of data from all major hospital EDs and DMATs in the region, despite the challenges of operating in a setting in which telephone communication, electricity, and gasoline were not always available. In addition, the physical presence of a surveillance team in health-care facilities permitted dialogue with clinical providers regarding the surveillance activity, without adding to the already burdened health-care system. The findings in this report are subject to at least three limitations. First, accurate pre- and post-hurricane population data were not available to calculate illness rates and allow for comparisons to place the findings into context. Second, diagnostic categories might have been miscoded because chief-complaint and discharge-diagnosis codes might have differed and classification might have varied by reviewer and condition (7,8). Finally, data on patient characteristics (e.g., recovery worker, resident, or shelter evacuee) were rarely collected in ED and DMAT records, limiting the ability to identify groups at higher risk. The Mississippi surveillance system, especially during the first week, was labor intensive, relying on teams of epidemiologists to travel throughout the region to collect and manually enter data. For monitoring illness and injury in a post-disaster setting, surveillance practices should allow for simple, direct electronic data entry of key syndromes of public health concern. When possible, data-collection guidelines and forms should be distributed to EDs and DMATS before the storm to ensure rapid initiation of post-storm data collection. Calculation of historical proportional morbidities for syndromes of public health concern before a disaster will enable local health departments and health-care facilities to provide useful background for post-disaster comparison. Surveillance results should be linked to educational resources, risk-communication messages, and recommendations of effective interventions. Finally, surveillance-system infrastructure should be self-contained at the site of the disaster with technological capabilities to collect data, transmit results, and deliver feedback to the affected region (9). Whether individual-level or aggregate surveillance methods are more effective for detecting outbreaks requires further evaluation (2). Both methods allayed concerns regarding infectious disease outbreaks in Mississippi; however, aggregate surveillance was less labor intensive. Acknowledgments This report is based, in part, on data provided by members of the Florida Epi Strike Team and health-care professionals in Hancock, Harrison, and Jackson counties. References
* Creation of DMATs is fostered by the U.S. Department of Homeland Security through the National Disaster Medical System. A DMAT is a group of medical professionals or paraprofessionals, supported by logistic and administrative staff, who can provide medical care during a disaster or other event. Each team has a sponsoring organization, such as a major medical center, public health or safety agency, or nonprofit, public, or private organization. The DMAT sponsor organizes the team, recruits members, arranges training, and coordinates deployment of the team. DMAT members are paid while serving as part-time federal employees. † Major injuries (e.g., amputations, fractures, or closed head and spinal cord injuries), minor injuries (e.g., strains, sprains, bruises, lacerations, contusions, or puncture wounds), three gastrointestinal syndromes (nausea/vomiting, bloody diarrhea, or watery diarrhea), three respiratory illnesses (upper respiratory infections, lower respiratory infections, or asthma), two skin conditions (rash or skin/wound infection), two mental health problems (attempted suicide or mental health condition), two environmentally induced illnesses (carbon monoxide poisoning or insect stings/bites), suspected meningo-encephalitis, and other illness visits (including for medication refills, cardiovascular disease, renal disease, chronic obstructive pulmonary disease, diabetes, headache, other chronic diseases, generalized pain, abdominal pain, or unspecified).
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 3/9/2006 |
|||||||||
|