|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
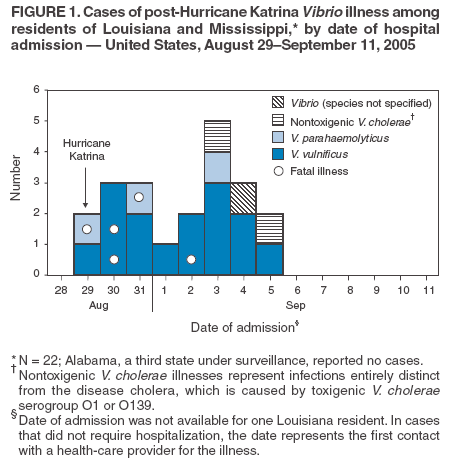
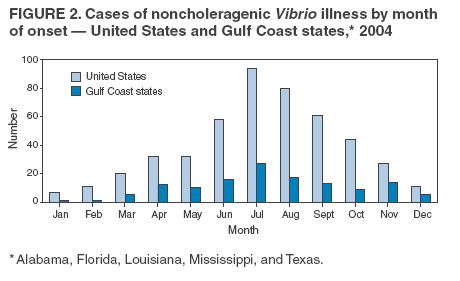
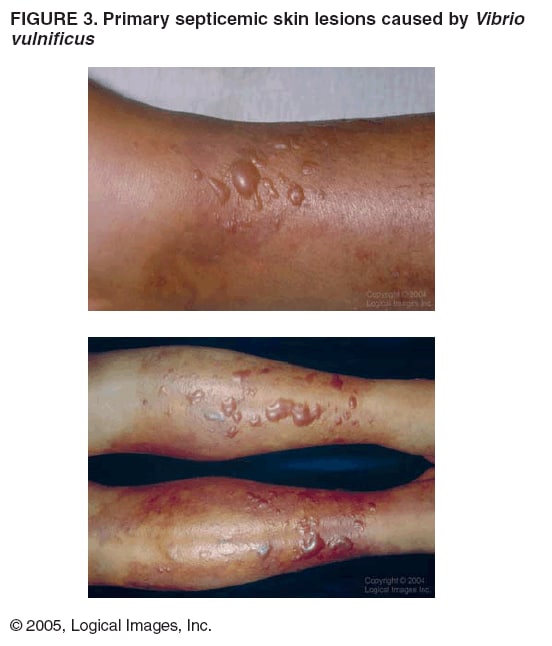
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Vibrio Illnesses After Hurricane Katrina --- Multiple States, August--September 2005On September 14, this report was posted as an MMWR Dispatch on the MMWR website (http://www.cdc.gov/mmwr). Hurricane Katrina made landfall on August 29, 2005, with major impact on the U.S. Gulf Coast. During August 29--September 11, surveillance identified 22 new cases of Vibrio illness with five deaths in persons who had resided in two states (Figure 1). These illnesses were caused by V. vulnificus, V. parahaemolyticus, and nontoxigenic V. cholerae. These organisms are acquired from the environment and are unlikely to cause outbreaks from person-to-person transmission. No cases of toxigenic V. cholerae serogroups O1 or O139, the causative agents of cholera, were identified. This report summarizes the investigation by state and local health departments and CDC, describes three illustrative cases, and provides background information on Vibrio illnesses. Results of the investigation underscore the need for heightened clinical awareness, appropriate culturing of specimens from patients, and empiric treatment of illnesses (particularly those associated with wound infections) caused by Vibrio species. No confirmed cases of illness have been identified with onset after September 5; additional Vibrio cases are under investigation. A case of post-hurricane Vibrio infection was defined as clinical illness in a person who had resided in a state struck by Hurricane Katrina (i.e., Alabama, Louisiana, or Mississippi) with illness onset and reporting during August 29--September 11, where Vibrio species was isolated from a wound, blood, or stool culture. Among cases, a wound-associated Vibrio case was defined as an illness that likely resulted from infection of a wound or abrasion acquired before or during immersion in floodwaters. Wound-Associated IllnessesEighteen wound-associated Vibrio cases were reported, in residents of Mississippi (seven) and Louisiana (five); in persons displaced from Louisiana to Texas (two), Arkansas (two), and Arizona (one); and in a person displaced from Mississippi to Florida (one). Speciation was performed in clinical laboratories for 17 of the wound-associated cases; 14 (82%) were V. vulnificus, and three (18%) were V. parahaemolyticus. Five (28%) patients with wound-associated Vibrio infections died; three deaths were associated with V. vulnificus infection, and two were associated with V. parahaemolyticus infection. Age of patients with wound-associated illnesses ranged from 31 to 89 years (median: 73 years). Fifteen (83%) were male. The majority of patients were hospitalized; admission dates ranged from August 29 to September 5. Not all patients were initially hospitalized because of their wounds. An underlying condition that might have increased risk for severe Vibrio illness was reported in 13 (72%) of the patients with wounds; these conditions included heart disease (seven patients), diabetes mellitus (four), renal disease (three), alcoholism (three), liver disease (two), peptic ulcer disease (one), immunodeficiency (one), and malignancy (one). Non-Wound--Associated IllnessesFour persons were reported with non-wound--associated Vibrio infections (two in Mississippi, one in Louisiana, and one displaced from Louisiana to Arizona). Information on the Vibrio species and clinical illness was available for two of these patients; the species were nontoxigenic V. cholerae isolated from patients with gastroenteritis. One of the infections occurred in a boy aged 2 months with diarrhea whose stool culture yielded both Salmonella group C2 and V. cholerae non-O1, non-O139. He was hospitalized for 2 days in Mississippi. The other V. cholerae non-O1, non-O139 isolate was from a stool specimen from an adult who was not hospitalized. No deaths were associated with the non-wound cases. Case ReportsTo illustrate the rapid onset and severity of Vibrio wound infections, brief descriptions of three of the cases are provided. Patient A. A man aged 60 years with a history of stroke, hypertension, and alcohol abuse arrived in Texas on August 31, after spending 3 days wading in the floodwaters of New Orleans, Louisiana. He was not housed at an evacuation center. On September 1, 2005, the man visited an emergency department with bilateral ankle wounds and diarrhea; he was treated and released. No details regarding treatment were available. Blood cultures subsequently yielded V. vulnificus. The patient was located and admitted to the hospital on September 2. He died the next day. Patient B. A man aged 61 years from Mississippi with human immunodeficiency virus infection, coronary artery disease, and hyperlipidemia was examined on August 29 and determined to have hypothermia and multiple second- and third-degree abrasions on his trunk. V. parahaemolyticus was isolated from his blood. Despite receiving antimicrobial therapy with levofloxacin, he died the next day. Patient C. A woman aged 49 years reported by her family to have hepatitis C was evacuated from New Orleans after a boat rescue. She visited an Arkansas hospital on September 4 with bullae, septic shock, and necrotizing fasciitis on her left leg, which was extensively debrided. V. vulnificus was isolated from her blood. As of September 12, she was being treated with ceftazidime and doxycycline and remained in critical condition. Reported by: D Engelthaler, MS, K Lewis, MD, S Anderson, MPH, Arizona Dept of Health Svcs. S Snow, MD, L Gladden, Arkansas Dept of Health. RM Hammond, PhD, RJ Hutchinson, Florida Dept of Health. R Ratard, MD, S Straif-Bourgeois, PhD, T Sokol, MPH, A Thomas, MPH, Louisiana Office of Public Health. L Mena, MD, J Parham, MD, School of Medicine, Univ of Mississippi Medical Center, Jackson; S Hand, M McNeill, MD, PhD, P Byers, MD, B Amy, MD, Mississippi Dept of Health. G Charns, Medical City Hospital of Dallas; J Rolling, A Friedman, J Romero, MPH, T Dorse, MD, J Carlo, MD, Dallas County Health and Human Svcs Dept; S Stonecipher, DVM, LK Gaul, PhD, T Betz, MD, Dept of State Health Svcs. RL Moolenar, MD, National Center for Environmental Health; JA Painter, DVM, MJ Kuehnert, MD, J Mott, PhD, DB Jernigan, MD, PA Yu, MPH, TA Clark, MD, National Center for Infectious Diseases; SK Greene, PhD, AM Schmitz, DVM, AC Cohn, MD, JL Liang, DVM, EIS officers, CDC. Editorial Note:After natural disasters such as Hurricane Katrina, the risk for illness related to infectious diseases is a public health concern. The findings in this report describe illnesses caused by Vibrio species, including wound infections resulting from post-hurricane exposure of wounds to flood waters. These findings underscore the need for prompt recognition and management of Vibrio wound infections by health-care providers. When the number of illnesses from infectious diseases increases after a natural disaster, they usually are caused by infectious agents normally present in the community or local environment (1). Nationwide, an average of 412 cases of noncholeragenic Vibrio* illnesses were reported each year during 2000--2004, including an average of 146 cases reported from the five Gulf Coast states (2). The most frequently reported Vibrio species are V. parahaemolyticus, V. vulnificus, and nontoxigenic V. cholerae. Vibrio illnesses in the United States are seasonal and peak during the summer (Figure 2). During 2000--2004, in the month of September, an average of 14 (range: 11--18) noncholeragenic Vibrio infections were reported from Gulf Coast states; an average of seven cases (range: 4--8) were wound-associated. Except for toxigenic V. cholerae O1 or O139, Vibrio illnesses are not nationally notifiable in the United States, and the actual number of noncholeragenic Vibrio illnesses is likely greater than the number reported. Cholera is a severe diarrheal illness caused by V. cholerae serogroups O1 or O139, which produce cholera toxin (i.e., toxigenic V. cholerae O1 or O139). A small endemic focus of toxigenic V. cholerae O1 exists in the Gulf of Mexico (3). During 2000--2004, a total of 16 cases of cholera were reported in the United States, and 13 (81%) of these infections were acquired during overseas travel or by consumption of imported seafood. Only three (19%) infections were acquired in the Gulf Coast states, all in the year 2000. Therefore, the risk for acquiring cholera associated with Hurricane Katrina is extremely low. Since 2000, at least seven noncholeragenic Vibrio species (V. vulnificus, V. parahaemolyticus, nontoxigenic V. cholerae, V. alginolyticus, V. fluvialis, V. mimicus, and V. hollisae) have been reported as causing illness each year in the United States. Although these organisms and those that cause cholera are grouped together under the genus Vibrio, they cause distinctly different illnesses. In the United States, noncholeragenic Vibrio usually are either foodborne, (e.g., resulting from eating raw or undercooked shellfish, particularly oysters, or other contaminated foods) or wound-associated (e.g., resulting from exposure to seawater or brackish waters where the organism naturally occurs). The incubation period for noncholeragenic Vibrio infection usually is 12--72 hours but can be as long as 1 week (2). Noncholeragenic Vibrio illnesses are not transmitted easily from person to person. Outbreaks, which are rare, usually are the result of consuming contaminated shellfish. The most frequently reported post-hurricane Vibrio illnesses were V. vulnificus and V. parahaemolyticus wound infections. These cases represent an increase over the normal reported incidence of Vibrio wound infections in Gulf Coast states and are consistent with exposure after hurricane landfall. Although precise exposure histories are not yet available for all patients, the infections caused by V. vulnificus likely resulted from wounds exposed to flood waters among persons with medical conditions that predisposed them to Vibrio infections. No evidence has been found of increased Vibrio gastrointestinal illness. V. vulnificus wound infections can begin as redness and swelling at the site of the wound and rapidly progress in patients at high risk to cause systemic illness, including sepsis. Whether acquired through wound infection or ingestion, V. vulnificus typically causes a severe and life-threatening illness characterized by fever and chills, decreased blood pressure (septic shock), and blood-tinged blistering skin lesions (hemorrhagic bullae) (Figure 3). Persons with chronic liver disease or immunocompromising conditions are particularly at risk for severe V. vulnificus infections (4,5). V. parahaemolyticus typically causes gastroenteritis after consumption of contaminated shellfish. Less frequently, V. parahaemolyticus causes wound infections that are generally less severe than V. vulnificus wound infections. However, in persons with liver disease or immunocompromising conditions, V. parahaemolyticus wound infections can lead to death. Nontoxigenic V. cholerae causes primarily gastroenteritis, but unlike toxigenic V. cholerae O1 or O139, nontoxigenic V. cholerae do not cause epidemics. Illness caused by this organism ranges in severity from mild diarrhea to severe watery diarrhea. Fever and bloody diarrhea are not typically observed. Immunocompromised persons and persons with liver disease can experience a more severe illness, including fever, chills, and septic shock. This organism has rarely been reported to cause wound infections. Vibrio infections are diagnosed by culture of wound, blood, or stool specimens. For stool specimens, a selective media of thiosulfate-citrate-bile salts-sucrose agar (TCBS) is recommended. If clinical suspicion of enteric Vibrio infection exists, the microbiology laboratory should be notified so that TCBS media will be used. Clinical laboratories should send all Vibrio isolates to state public health laboratories for confirmation. CDC continues to work with local and state public health officials to investigate post-Katrina Vibrio illnesses. Persons working in hurricane-damaged areas, especially in areas with standing brackish water, should wear boots and other protective gear to prevent wounds and to prevent exposure of broken skin to contaminated water. To prevent Vibrio infections, persons with open wounds or broken skin should avoid contact with brackish water or seawater, especially if they have preexisting liver disease or other immunocompromising conditions. Injury prevention is especially important for persons in these high-risk populations. Healthy persons are at much lower risk for Vibrio infection. In areas where flood waters have receded and surfaces are dry, Vibrio should not be a concern because the organism is killed rapidly by drying (6). To reduce the risk for Vibrio wound infection, persons should wash all wounds that have been exposed to sea or brackish waters with soap and clean water thoroughly as soon as possible and seek medical care for any wound that appears infected. Clinicians should be vigilant for Vibrio infection in hurricane evacuee populations, particularly in patients with infected wounds and especially if the patients are in a high-risk group. If V. vulnificus is suspected, antimicrobial therapy should be initiated immediately; prompt treatment can improve survival. Antimicrobials effective against Vibrio infections include doxycycline, third-generation cephalosporins (e.g., ceftazidime), fluoroquinolones, and aminoglycosides (7). Wound infections also should be treated with aggressive attention to the wound site; amputation of the infected limb is sometimes necessary. Additional information regarding management of V. vulnificus wound infections is available at http://www.bt.cdc.gov/disasters/hurricanes/Katrina/vibriofaq.asp . For Vibrio gastroenteritis that is mild and self-limited, treatment with oral rehydration usually is sufficient. Antimicrobial therapy might be helpful for patients with severe or prolonged diarrhea. Acknowledgments The findings in this report are based, in part, on contributions by C Bopp, MS, E Mintz, MD, J Sobel, MD, National Center for Infectious Diseases; W Arvelo, MD, N Gaffga, MD, MP Menon, MD, EIS officers, CDC. References
* All Vibrio species other than toxigenic V. cholerae O1 or O139.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/22/2005 |
|||||||||
|