|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
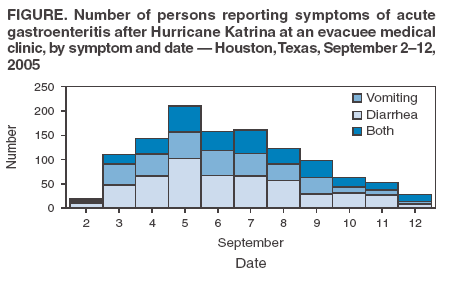
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Norovirus Outbreak Among Evacuees from Hurricane Katrina --- Houston, Texas, September 2005During the week after Hurricane Katrina struck the Gulf Coast on August 29, 2005, an estimated 240,000 persons, mostly from Louisiana, evacuated to Houston, Texas. On August 31, an estimated 24,000 evacuees were sheltered temporarily at facilities in Reliant Park, a sports and convention complex that includes Reliant Astrodome, Reliant Center, and Reliant Arena. All evacuees to these three facilities were provided with cots, bedding, food, water, and access to lavatories and showers. A medical facility was set up initially to provide emergency care to evacuees and subsequently to serve as a comprehensive outpatient clinic staffed largely by personnel from the Harris County Hospital District (HCHD), Baylor College of Medicine (BCM), and Texas Children's Hospital (TCH). On September 2, 2005, physicians and staff from Harris County Public Health and Environmental Services (HCPHES) noted a substantial number of adults and children with symptoms of acute gastroenteritis (defined as diarrhea and/or vomiting) at the medical clinic in Reliant Park. In collaboration with HCPHES, CDC and medical personnel of HCHD, BCM, and TCH conducted enhanced surveillance to improve identification of acute gastroenteritis, investigate the apparent outbreak, identify the infectious agent, and implement measures for its control. This report summarizes the preliminary epidemiologic data from this investigation and underscores the challenges to managing a large and rapidly spreading outbreak of norovirus in crowded evacuee settings. A simple checklist of symptoms was used by HCPHES to collect data on a triage intake form. Data were used as an index of medical problems and care delivered. This information was gathered and entered into a centralized database nightly by HCPHES staff members, and results were distributed to the surveillance team each morning. During September 2--12, 2005, approximately 6,500 of the estimated 24,000 evacuees visited the Reliant Park medical clinic, and 1,169 (18%) persons reported symptoms of acute gastroenteritis (Figure). Three fourths of the patients with acute gastroenteritis symptoms were adults (aged >18 years) residing in the three facilities housing evacuees at Reliant Park or in smaller shelters and hotels in Houston. The number of acute gastroenteritis cases peaked on September 5, when 211 persons reported acute gastroenteritis symptoms, and cases declined slowly thereafter. A total of 511 (44%) patients reporting acute gastroenteritis symptoms had diarrhea alone, 342 (29%) reported vomiting, and 316 (27%) reported both diarrhea and vomiting. During September 2--12, approximately 14% of adult visits to the medical clinic and 28% of pediatric visits were for acute gastroenteritis; on peak days, these figures reached 21% and 40%, respectively (other common reasons for visits were chronic diseases and medication refills). In addition, medical personnel, police officers, and volunteers who had direct contact with patients reported acute gastroenteritis symptoms, suggesting substantial secondary spread, presumably by person-to-person contact or fomite transmission. The number of hospitalizations was unknown; no deaths were reported. To determine the etiologic agent, stool samples (i.e., either rectal swabs or bulk stools) were sent to one of several laboratories of HCHD, BCM, and TCH for diagnosis of bacterial, parasitic, and viral enteropathogens. In stool samples from 44 patients tested by reverse transcription-polymerase chain reaction, norovirus was confirmed in 22 (50%) specimens; no other enteropathogen was identified. Sequencing to determine viral strains is being conducted but is not yet complete. At the onset of the outbreak, health authorities implemented extensive infection-control measures. Patients with acute gastroenteritis who were dehydrated were rehydrated in a separate observation area reserved for patients with suspected infectious illness and then transferred to an isolation area for at least 48 hours after vomiting and diarrhea had ended. In addition, alcohol-based gel hand sanitizers were distributed throughout the facilities and near lavatories, and a bank of portable sinks was installed inside the medical clinic. Medical staff, disaster relief personnel, volunteers, and evacuees were all alerted to the heightened need for using proper hand-washing techniques through medical staff meetings, posters, banners, and newsletters distributed to all evacuees. Despite these timely interventions, the outbreak continued for more than 1 week but declined before the evacuees vacated Reliant Park in late September. Reported by: H Palacio, MD, U Shah, MD, C Kilborn, MPH, D Martinez, MPH, V Page, MPH, Harris County Public Health and Environmental Svcs; T Gavagan, MD, K Mattox, MD, H DuPont, MD, MK Estes, PhD, R Feigin, MD, RL Atmar, MD, FH Neill, J Versalovic, MD, PhD, C Stager, PhD, D Musher, MD, Texas Children's Hospital, Baylor College of Medicine, and Harris County Hospital District, Houston, Texas. RI Glass, MD, PhD, Div of Viral and Rickettsial Disease, National Center for Infectious Diseases; M Faul, PhD, Div of Injury and Disability Outcomes and Programs, National Center for Injury Prevention and Control; M Davies, MD, North Carolina Dept of Health and Human Svcs; M Cortese, MD, Div of Epidemiology and Surveillance, National Immunization Program; E Lau, MD, EIS Officer, CDC. Editorial Note:The epidemiologic and laboratory findings in this report suggest that an outbreak of norovirus gastroenteritis might have affected approximately 1,000 evacuees and relief workers in three facilities at Reliant Park and in other Houston facilities that housed evacuees, including a convention center, smaller shelters, and hotels. The rapidly changing population of evacuees treated at the medical clinic complicated efforts to monitor the magnitude of the outbreak or the extent of disease among evacuees in Reliant Park. Nonetheless, on some days, nearly 21% of adults and 40% of children visiting the Reliant clinic had acute gastroenteritis, confirming the importance of this problem. Conditions that might have facilitated virus transmission included crowding, insufficient sanitation in lavatories, lack of an adequate number of hand-washing facilities, and delays in cleaning and decontaminating soiled areas and bedding. In addition, initial isolation procedures were difficult to maintain over time because family members already traumatized by displacement, grief, and personal loss were separated from each other because of illness. Noroviruses are the most common cause of outbreaks of acute gastroenteritis in the United States. Outbreaks not associated with contaminated food or water but spread through person-to-person contact or from fomites tend to occur in crowded settings, such as cruise ships, camps, shelters, and hospital wards (1--4). Persons infected with norovirus have an acute onset of vomiting and/or nonbloody diarrhea lasting 12--60 hours, with an incubation period of 24--48 hours (5). Certain persons do not become ill when infected, which might be associated with a genetic predisposition to infection conferred by blood group antigens (6). Once an outbreak begins, norovirus is highly contagious and easily transmitted via multiple routes because of its low infectious dose (i.e., <100 viral particles), its ability to persist in the environment, and its resistance to inactivation by multiple cleaning agents (5,7). Furthermore, diagnosis of norovirus through laboratory testing is not widely available, making confirmation of norovirus as the etiologic agent in these types of outbreaks difficult. Although the challenges to preventing and managing norovirus outbreaks in a disaster relief situation are considerable, certain lessons have been learned from this and other norovirus outbreaks. Early surveillance and identification of outbreaks of acute gastroenteritis with rapid detection of the causative agent are essential to implement timely, focused, and effective interventions. In particular, vigilance to hand-washing techniques; accessibility to soap and water within medical facilities, eating and food-preparation areas, lavatories, and showers; and containment and disinfection of soiled areas and bedding can all help decrease the spread of norovirus. These needs warrant special attention in planning and managing a disaster relief facility (8,9). When feasible, isolation of patients who are actively vomiting or continue to have diarrhea can be instituted, but care should be taken not to further distress traumatized evacuees. Norovirus should be suspected when outbreaks of acute gastroenteritis occur in a crowded setting, on the basis of its epidemiologic features (i.e., rapid spread and secondary transmission) and clinical presentation (e.g., high prevalence of vomiting). Persons with norovirus gastroenteritis should be treated promptly with rehydration, and measures to prevent secondary transmission (e.g., promoting proper hand-washing techniques and cleaning and disinfecting soiled surfaces) should be taken immediately; however, these measures give no absolute assurance against further spread of norovirus (5,10). The outbreak described in this report was identified early and managed aggressively. However, rapid, sensitive laboratory assays are still needed to detect norovirus and to provide a better understanding of the most effective intervention strategies in crowded evacuee environments. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/13/2005
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|