|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
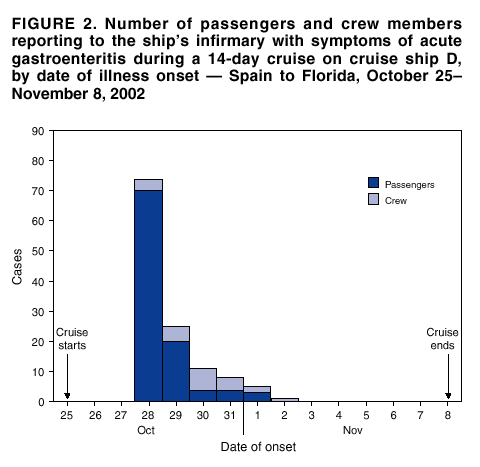
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreaks of Gastroenteritis Associated with Noroviruses on Cruise Ships --- United States, 2002During January 1--December 2, 2002, CDC's Vessel Sanitation Program (VSP), which conducts surveillance for acute gastroenteritis (AGE) on cruise ships with foreign itineraries sailing into U.S. ports (1), received reports of 21 outbreaks of AGE* on 17 cruise ships. Of the 21 outbreaks, nine were confirmed by laboratory analysis of stool specimens from affected persons to be associated with noroviruses, three were attributable to bacterial agents, and nine were of unknown etiology. Seven outbreaks were reported in 2001, and of these, four were confirmed to be associated with norovirus (CDC, unpublished data, 2002). This report describes five of the norovirus outbreaks that occurred during July 1--December 2, 2002, on cruise ships. OutbreaksCruise Ship A. On July 18, cruise ship A, owned by cruise line A, embarked 1,318 passengers and 564 crew members for a 7-day cruise from Vancouver to Alaska. On July 19, five passengers reported to the ship's infirmary with symptoms of AGE (Figure 1). By July 25, a total of 167 (13%) passengers and nine (2%) crew members had reported illness. Among the 176 patients, the predominant symptoms were vomiting (76%) and diarrhea (73%). Five of 10 stool specimens from ill passengers were positive for norovirus by reverse transcriptase polymerase chain reaction (RT-PCR). On July 25, when passengers disembarked, the ship was disinfected in accordance with CDC recommendations, and the same day, a new group of passengers embarked for another 7-day cruise. During the cruise, 189 (14%) of 1,336 passengers and 30 (5.3%) of 571 crew members had AGE with diarrhea (91%) and vomiting (85%) (Figure 1). An environmental health inspection conducted by CDC revealed no sanitary deficiencies. Cruise line A cancelled a subsequent cruise and voluntarily took the ship out of service for 1 week for aggressive cleaning and sanitizing. No outbreaks were reported on subsequent cruises. Cruise Ship B. On October 1, cruise ship B, also owned by cruise line A, embarked 1,281 passengers and 598 crew members for a 21-day cruise from Washington to Florida. By October 16, a total of 101 (8%) passengers and 14 (2%) crew members reported to the infirmary with AGE symptoms. On October 18, CDC investigators boarded the ship to conduct an epidemiologic and environmental investigation. Of 972 surveyed passengers, 399 (41%) met the case definition for AGE. Investigators found no association between illness and water, specific meals served on the ship, or with offshore excursions. Stool specimens from 12 of 13 patients tested positive for norovirus. Characterization of the strain by sequence analysis of RT-PCR products matched those from cruise ship A. Despite implementation of control measures that included disinfection of the vessel and quarantine of ill passengers and crew members, a total of 264 passengers and 41 crew members reported illness on three subsequent 10-day cruises. Cruise line A voluntarily withdrew cruise ship B from service for 10 days for aggressive cleaning and sanitizing. No outbreaks were reported on subsequent voyages. Cruise Ship C. On September 28, cruise ship C, owned by cruise line B, embarked 1,984 passengers and 941 crew members for a 7-day round-trip cruise from Florida to the Caribbean. Several passengers had AGE within 24 hours of embarkation, and by October 1, a total of 70 (4%) passengers and two (0.2%) crew members reported illness. On October 3, CDC investigators boarded the ship to conduct an epidemiologic and environmental investigation. Questionnaires completed by 1,879 (95%) passengers and 860 (91%) crew members identified 356 (19%) passengers and 13 (1.5%) crew members who met the AGE case definition. The epidemiologic investigation suggested a point source of infection, followed by cases associated with person-to-person transmission. The investigation identified an association between illness among passengers and lunch served at embarkation (odds ratio=2.4; 95% confidence interval=1.1--5.2; p value=0.02). Four of 11 stool specimens from patients were positive for norovirus by RT-PCR. Characterization of the strain by sequence analysis of RT-PCR products matched those from an outbreak on the same ship that occurred 3 weeks previously but was not identical to the outbreak strain on cruise ships A and B. CDC recommended reinforcing sanitation practices and excluding ill foodhandlers from the work place. Cruise ship C continued service, and no new cases were reported on subsequent cruises. Cruise Ship D. On October 25, cruise ship D, owned by cruise line C, embarked 2,882 passengers and 944 crew members in Spain for a 14-day cruise to Florida. On October 28, a total of 70 (2.5%) passengers reported to the infirmary with AGE; the number of ill passengers declined rapidly during the following days (Figure 2). By November 2, a total of 106 (5%) passengers and 25 (3%) crew members had reported illness. Stool specimens from four of six patients tested positive for norovirus by RT-PCR. Characterization of the strain by sequence analysis of RT-PCR products identified a strain distinct from the other cruise-ship outbreaks. With passengers aboard, control measures included quarantine of ill crew members until symptom-free for 72 hours, disinfection of the ship, and reinforcement of sanitation practices. No new outbreaks were reported on subsequent cruises. Cruise Ship E. On November 16, cruise ship E, owned by cruise line D, embarked 2,318 passengers and 988 crew members for a 7-day cruise from Florida to the Caribbean. By November 20, a total of 28 (1%) passengers and seven (1%) crew members had reported to the ship's infirmary with AGE. By disembarkation on November 23, a total of 260 (12%) passengers and 17 (2%) crew members had reported illness. On November 23, CDC investigators boarded the ship and collected questionnaires that had been distributed to all passengers before disembarkation. A total of 1,280 (55%) passengers returned a questionnaire; of these, 492 (21%) met the case definition for AGE. Seven of 12 specimens from patients were positive for norovirus by RT-PCR. Characterization of the strain by sequence analysis of RT-PCR products identified a perfect match with those products from the outbreaks on cruise ships A and B. Despite implementation of disinfection and sanitation measures, the outbreak continued on the subsequent cruise. On November 30, cruise line D removed the ship from service for 1 week for aggressive cleaning and sanitizing. Reported by: EH Cramer, MD, D Forney, Vessel Sanitation Program; AL Dannenberg, MD, Div of Emergency and Environmental Health Svcs, National Center for Environmental Health; MA Widdowson, VetMB, JS Bresee, MD, S Monroe, PhD, RS Beard, H White, MS, S Bulens, MPH, Div of Viral and Rickettsial Diseases; E Mintz, MD, C Stover, MPH, Div of Bacterial Diseases, National Center of Infectious Diseases; E Isakbaeva, MD, J Mullins, DVM, J Wright, DVM, V Hsu, MD, W Chege, MD, J Varma, MD, EIS officers, CDC. Editorial Note:Cruise-ship outbreaks demonstrate how easily noroviruses can be transmitted from person to person in a closed environment, resulting in large outbreaks (2--4). The continuation of these outbreaks on consecutive cruises with new passengers and the resurgence of outbreaks caused by the same virus strains during previous cruises on the same ship, or even on different ships of the same company, suggests that environmental contamination and infected crew members can serve as reservoirs of infection for passengers. The increase in reported norovirus outbreaks on cruise ships in 2002 might reflect an actual increase in norovirus outbreaks or it might be attributable to improved surveillance with an electronic reporting format implemented January 1, 2001, and increased application of sensitive molecular assays. The surveillance system captures cases of illness reported to the ship's infirmary or to designated staff on board the ship. Other cases of AGE among passengers and crew members are not reported. In 2002, CDC has confirmed 26 land-based outbreaks of AGE attributable to norovirus; three were caused by strains closely related to the strain detected from cruise ships A, B, and E. Although several land-based outbreaks are linked to norovirus strains with unique sequence types, strains with identical sequence types are identified commonly in outbreaks with no obvious epidemiologic link. Further genetic characterization of common outbreak strains associated with epidemiologic data might help establish possible links among these outbreaks. Noroviruses (i.e., Norwalk-like viruses or NLV) are members of the family Caliciviridae and are well-recognized etiologic agents of nonbacterial AGE (5). Noroviruses cause approximately 23 million cases of AGE each year and are the leading cause of outbreaks of gastroenteritis (5,6). Illness caused by norovirus infection lasts 12--60 hours and is characterized by sudden onset of nausea, vomiting, and watery diarrhea (7); the incubation period is 12--48 hours. The virus is transmitted by hands contaminated through the fecal-oral route, directly from person to person, through contaminated food or water, or by contact with contaminated surfaces or fomites (8). Aerosolized vomitus also has been implicated as a transmission mode (9). Because of high infectivity and persistence in the environment, transmission of noroviruses is difficult to control through routine sanitary measures (3,4,9). Although norovirus causes a self-limited AGE, elderly passengers, children, and those with severe underlying medical conditions might be at increased risk for complications because of volume depletion and electrolyte disturbances. Hospitalization of adults with norovirus who are otherwise healthy is rare. Neither specific antiviral treatment nor a vaccine has been developed for noroviruses. In addition to emphasizing basic food and water sanitation measures, control efforts should include thorough and prompt disinfection of ships during cruises, and isolation of ill crew members and, if possible, passengers for 72 hours after clinical recovery. Suitable disinfectants include freshly prepared chlorine solutions at concentrations of >1,000 ppm, phenol-based compounds, and accelerated hydrogenperoxide products (10). Cruise ships also should promote frequent, rigorous hand washing with soap and water by passengers and crew members. Rapid implementation of control measures at the first sign of a suspected AGE outbreak is critical in preventing additional cases. When routine disinfection measures are unsuccessful at interrupting the spread of virus during an outbreak, more extensive disinfection and a period of time without passengers aboard a ship might facilitate elimination of the virus. CDC encourages local and state health departments to test for noroviruses when investigating outbreaks of suspected viral AGE. For assistance in testing for noroviruses and for strain characterization, local and state health departments should contact CDC's Viral Gastroenteritis Section, telephone 404-639-3577 or by e-mail: CaliciNet@cdc.gov. References
* An outbreak of AGE was defined as one in which >3% of passengers or crew members report illness (defined as three or more episodes of loose stools in a 24-hour period or as vomiting with one additional symptom such as abdominal cramps, headache, myalgia, or fever). The evaluation of an outbreak might consist of environmental, epidemiologic, and laboratory investigative components, including an epidemic survey distributed to passengers and crew members, environmental sampling, and collection of stool specimens from patients.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/12/2002 |
|||||||||
This page last reviewed 12/12/2002
|