|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
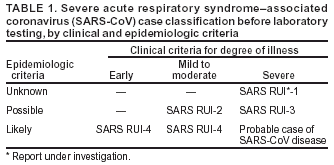
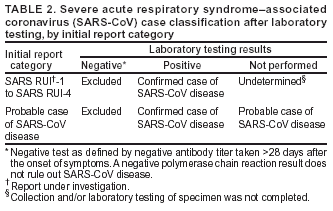
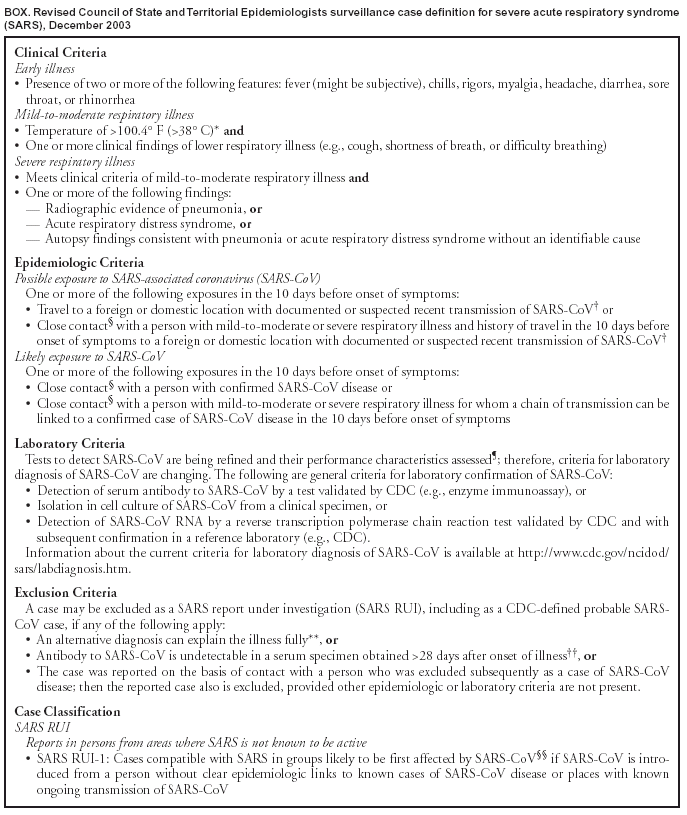
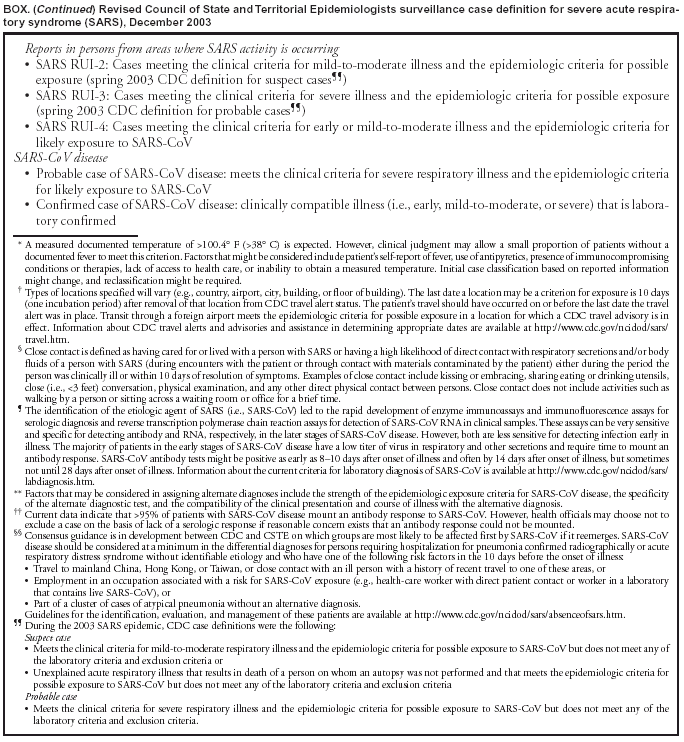
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Revised U.S. Surveillance Case Definition for Severe Acute Respiratory Syndrome (SARS) and Update on SARS Cases --- United States and Worldwide, December 2003During the 2003 epidemic of severe acute respiratory syndrome (SARS), CDC and the Council of State and Territorial Epidemiologists (CSTE) developed surveillance criteria to identify persons with SARS. The surveillance case definition changed throughout the epidemic as understanding of the clinical, laboratory, and transmission characteristics of SARS-associated coronavirus (SARS-CoV) increased (1--5). On June 26, CSTE adopted a position statement to add SARS-CoV disease to the National Notifiable Disease Surveillance System (NNDSS). The position statement included criteria for defining a SARS case for national reporting. On November 3, CSTE issued a new interim position statement* with a revised SARS case definition. This report summarizes the new U.S. surveillance case definition for SARS and updates reported cases of SARS worldwide and in the United States. Summary of Changes to Case DefinitionThe revised SARS case definition (Box) modifies the clinical, epidemiologic, laboratory, and case-exclusion criteria in the U.S. surveillance case definition used during the 2003 epidemic. In the clinical criteria, "early" illness replaces "asymptomatic" or "mild" illness. The epidemiologic criteria include the following new categories: 1) possible exposure to SARS-CoV and 2) likely exposure to SARS-CoV. Laboratory criteria for evidence of SARS-CoV infection reflect advances in testing technology. The case-exclusion criteria have been changed to allow for exclusion when a serum sample collected >28 days after onset of symptoms is negative for antibody to SARS-CoV. The revised case definition also classifies each SARS case as either a SARS report under investigation (SARS RUI) or SARS-CoV disease. SARS RUI is a sensitive, nonspecific case classification based solely on clinical or epidemiologic criteria and includes cases classified previously as probable or suspect. SARS-CoV disease is a more specific case classification based on selected clinical and epidemiologic criteria or laboratory confirmation. SARS RUIs might subsequently meet the definition for SARS-CoV disease based on results from laboratory testing (Tables 1 and 2). Update on SARS CasesDuring November 2002--July 2003, a total of 8,098 probable SARS cases were reported to the World Health Organization (WHO) from 29 countries, including 29 cases from the United States; 774 SARS-related deaths (case-fatality rate: 9.6%) were reported, none of which occurred in the United States (6). Eight U.S. cases had serologic evidence of SARS-CoV infection; these eight cases have been described previously (7--10). A total of 156 reported U.S. SARS cases from the 2003 epidemic remain under investigation, with 137 (88%) cases classified according to previous surveillance criteria as suspect SARS and 19 (12%) classified as probable SARS. Because convalescent serum specimens have not been obtained from the 19 probable and 137 suspect cases that remain under investigation, whether these persons had SARS-CoV disease is unknown. Reported by: SARS Team and Executive Committee, Council of State and Territorial Epidemiologists. SARS Investigative Team, CDC. Editorial Note:The revised surveillance case definition for SARS reflects an improved understanding of the clinical and laboratory characteristics of SARS-CoV. The revision differentiates patients with nonspecific clinical illness or less definitive epidemiologic associations (i.e., SARS RUIs) from those with laboratory-confirmed SARS-CoV infection or more definitive epidemiologic links (i.e., cases of SARS-CoV disease). Local and state health departments will monitor SARS RUIs to ensure implementation of prompt public health measures for preventing disease transmission if SARS-CoV is confirmed subsequently. Numerous SARS RUIs probably will be excluded as SARS cases as laboratory results become available during the course of illness. Surveillance data for cases meeting the SARS-CoV disease case definition will be reported to NNDSS and included in the weekly statistical summary of notifiable infectious diseases in the United States published in MMWR (Table 1. Summary of provisional cases of selected notifiable diseases, United States). Reporting of cases meeting previous SARS definitions ended in late July 2003. However, case numbers continue to change as new clinical information or results of additional laboratory testing on cases reported previously become available. Updated case counts reflecting these changes are available from CDC at http://www.cdc.gov/od/oc/media/sars/cases.htm. Efforts are under way to prepare for a possible reappearance of SARS-CoV. CDC, in collaboration with other federal partners, state and local health officials, professional organizations and societies, and representatives of the health-care industry, has developed a guidance document to help public health and health-care officials detect the reappearance of SARS-CoV in the United States quickly and implement a decisive and effective public health response. The document, "Public Health Guidance for Community-Level Preparedness and Response to Severe Acute Respiratory Syndrome (SARS)," is available at http://www.cdc.gov/ncidod/sars/sarsprepplan.htm. References
* The interim position statement must be ratified by the entire membership at the 2004 annual CSTE meeting. The statement is available from CSTE at http://www.cste.org/ps/2003pdfs/2003finalpdf/cstesarscasedefrevision2003-10-30.pdf.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 12/11/2003 |
|||||||||
This page last reviewed 12/11/2003
|