|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
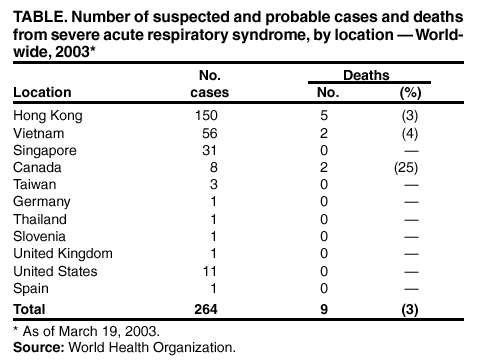
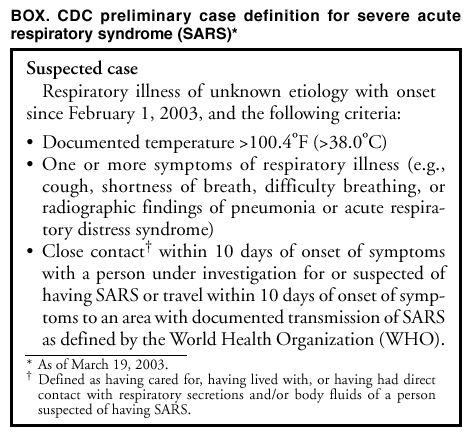
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Severe Acute Respiratory Syndrome ---Worldwide, 2003Please note: An erratum has been published for this article. To view the erratum, please click here. Since late February 2003, CDC has been supporting the World Health Organization (WHO) in the investigation of a multicountry outbreak of atypical pneumonia of unknown etiology. The illness is being referred to as severe acute respiratory syndrome (SARS). This report describes the scope of the outbreak, preliminary case definition, and interim infection control guidance for the United States. On February 11, the Chinese Ministry of Health notified WHO that 305 cases of acute respiratory syndrome of unknown etiology had occurred in six municipalities in Guangdong province in southern China during November 16, 2002--February 9, 2003. The disease was characterized by transmission to health-care workers and household contacts; five deaths were reported (1). On February 26, a man aged 47 years who had traveled in mainland China and Hong Kong became ill with a respiratory illness and was hospitalized shortly after arriving in Hanoi, Vietnam. Health-care providers at the hospital in Hanoi subsequently developed a similar illness. The patient died on March 13 after transfer to an isolation facility in Hong Kong. During late February, an outbreak of a similar respiratory illness was reported in Hong Kong among workers at another hospital; this cluster was linked to a patient who had traveled previously to southern China. On March 12, WHO issued a global alert about the outbreak and instituted worldwide surveillance. As of March 19, WHO has received reports of 264 patients from 11 countries with suspected and probable* SARS (Table). Areas with reported local transmission include Hong Kong and Guangdong province, China; Hanoi, Vietnam; and Singapore. More limited transmission has been reported in Taipei, Taiwan, and Toronto, Canada. The initial cases reported in Singapore, Taiwan, and Toronto were among persons who all had traveled to China. On March 15, after issuing a preliminary case definition for suspected cases (Box, CDC initiated enhanced domestic surveillance for SARS. CDC also issued a travel advisory suggesting that persons planning nonessential travel to Hong Kong, Guangdong, or Hanoi consider postponing their travel (http://www.cdc.gov/travel/other/acute_resp_syn_multi.htm). On March 16, CDC began advising passengers arriving on direct flights from these three locations to seek medical attention if they have symptoms of febrile respiratory illness. As of March 18, approximately 12,000 advisory notices had been distributed to airline passengers. In addition, surveillance is being heightened for suspected cases of SARS among arriving passengers. As of March 19, a total of 11 suspected cases of SARS in the United States are under investigation by CDC and state health authorities. Among patients reported worldwide as of March 19, the disease has been characterized by rapid onset of high fever, myalgia, chills, rigor, and sore throat, followed by shortness of breath, cough, and radiographic evidence of pneumonia. The incubation period has generally been 3--5 days (range: 2--7 days). Laboratory findings have included thrombocytopenia and leukopenia. Many patients have had respiratory distress or severe pneumonia requiring hospitalization, and several have required mechanical ventilation. Of the 264 suspected and probable cases reported by WHO, nine (3%) persons have died. In addition, secondary attack rates of >50% have been observed among health-care workers caring for patients with SARS in both Hong Kong and Hanoi. Additional clinical and epidemiologic details are available from WHO at http://www.who.int/wer/pdf/2003/wer7812.pdf. In the United States, initial diagnostic testing for persons with suspected SARS should include chest radiograph, pulse oximetry, blood cultures, sputum Gram stain and culture, and testing for viral respiratory pathogens, particularly influenza types A and B and respiratory syncytial virus. Clinicians should save any available clinical specimens (e.g., respiratory samples, blood, serum, tissue, and biopsies) for additional testing until diagnosis is confirmed. Instructions for specimen collection are available from CDC at http://www.cdc.gov/ncidod/sars/pdf/specimencollection-sars.pdf. Specimens should be forwarded to CDC by state health departments after consultation with the SARS State Support Team at the CDC Emergency Operations Center. Clinicians evaluating suspected cases should use standard precautions (e.g., hand hygiene) together with airborne (e.g., N-95 respirator) and contact (e.g., gowns and gloves) precautions (http://www.cdc.gov/ncidod/sars/infectioncontrol.htm). Until the mode of transmission has been defined more precisely, eye protection also should be worn for all patient contact. As more clinical and epidemiologic information becomes available, interim recommendations will be updated. Reported by: CDC SARS Investigative Team; AT Fleischauer, PhD, EIS Officer, CDC. Editorial Note:During 2000, approximately 83 million nonresident passengers arrived in China, 13 million in Hong Kong, and 2 million in Vietnam, and approximately 460,000 residents of China, Hong Kong, and Vietnam traveled to the United States (2). During January 1, 1997--March 18, 2003, an estimated 5% of ill tourists worldwide who sought post-travel care from one of 35 worldwide GeoSentinel travel clinics had pneumonia (International Society of Tropical Medicine, unpublished data, 2003). In the United States, approximately 500,000 persons with pneumonia require hospitalization each year; in approximately half of these cases, no etiologic agent is identified despite intensive investigation (3,4). On the basis of these data and the broad and necessarily nonspecific case definition, cases meeting the criteria for SARS are anticipated worldwide and in the United States. However, most of the anticipated cases are expected to be unrelated to the current outbreak. Electron microscopic identification of paramxyovirus-like particles has been reported from Germany and Hong Kong (5). This family of viruses includes measles, mumps, human parainfluenza viruses, and respiratory syncytial virus in addition to the recently identified henipaviruses and metapneumovirus. Additional testing is under way to confirm a definitive etiology. Identification of the causative agent should lead to specific diagnostic tests, simplify surveillance, and focus treatment guidelines and infection control guidance. Clinicians and public health officials who suspect cases of SARS are requested to report such cases to their state health departments. CDC requests that reports of suspect cases from state health departments, international airlines, cruise ships, or cargo carriers be directed to the SARS Investigative Team at the CDC Emergency Operations Center, telephone 770-488-7100. Additional information about SARS (e.g., infection control guidance and procedures for reporting suspected cases) is available at http://www.cdc.gov/ncidod/sars. Global case counts are available at http://www.who.int. References
* Suspected cases (Box with either a) radiographic evidence of pneumonia or respiratory distress syndrome or b) evidence of unexplained respiratory distress syndrome by autopsy are designated probable cases by the WHO case definition.
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/20/2003 |
|||||||||
This page last reviewed 3/20/2003
|