|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
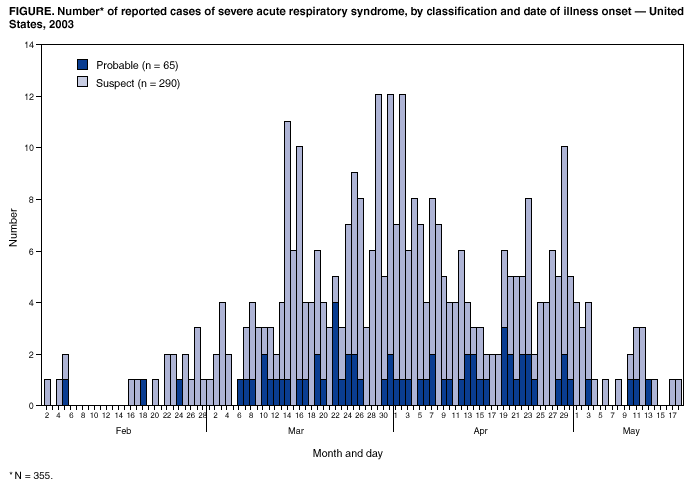
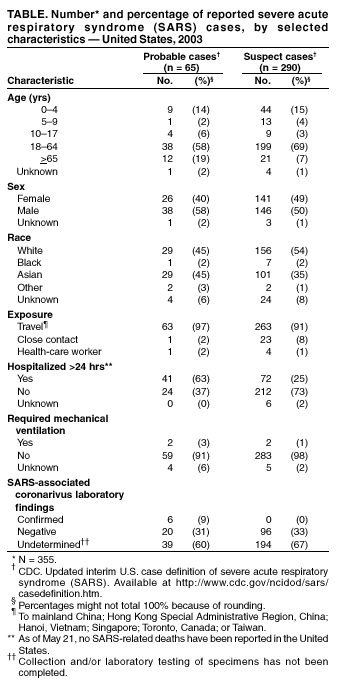
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Severe Acute Respiratory Syndrome --- United States, May 21, 2003CDC continues to work with state and local health departments, the World Health Organization (WHO), and other partners to investigate cases of severe acute respiratory syndrome (SARS). This report updates SARS cases reported worldwide and in the United States and highlights recent modifications to the U.S. SARS case definition that define criteria for exclusion of previously reported SARS cases and for reporting travel-associated cases of SARS. During November 1, 2002--May 21, 2003, a total of 7,956 SARS cases were reported to WHO from 28 countries, including the United States; 666 deaths (case-fatality proportion: 8.4%) have been reported (1). A total of 355 SARS cases identified in the United States have been reported from 40 states with 290 (82%) cases classified as suspect SARS and 65 (18%) classified as probable SARS (more severe illnesses characterized by the presence of pneumonia or acute respiratory distress syndrome) (Figure, Table) (2). One probable and nine suspect cases have been identified since the last update (3). Of the 65 probable SARS patients, 41 (63%) were hospitalized, and two (3%) required mechanical ventilation. No SARS-related deaths have been reported in the United States. Of 65 probable cases, 63 (97%) were attributed to international travel to areas with documented or suspected community transmission of SARS within the 10 days before illness onset; the remaining two (3%) probable cases occurred in a health-care worker who provided care to a SARS patient and a household contact of a SARS patient. Among the 63 probable SARS cases attributed to travel, 33 (52%) patients reported travel to mainland China; 19 (30%) to Hong Kong Special Administrative Region, China; six (10%) to Singapore; two (3%) to Hanoi, Vietnam; nine (14%) to Toronto, Canada; and one (2%) to Taiwan. Of the probable SARS patients, five (8%) had visited more than one area with SARS during the 10 days before illness onset. Laboratory testing to evaluate infection with the SARS-associated coronavirus (SARS-CoV) has been completed for 122 cases (26 probable and 96 suspect). Since the last update (3), the number of cases with laboratory-confirmed infection with SARS-CoV remains at six; all are probable SARS cases with no suspect SARS cases having laboratory evidence of infection with SARS-CoV. Negative findings (i.e., the absence of antibody to SARS-CoV in convalescent serum obtained >21 days after symptom onset) have been documented for 116 cases (96 suspect and 20 probable). The number of new cases reported in the United States has been decreasing in recent weeks. The epidemiologic profile of reported cases remains unchanged with most cases associated with international travel and few instances of secondary spread to family members or other contacts. However, vigilance is critical to ensure rapid recognition and appropriate management of persons with SARS The low specificity of the surveillance case definition captures many persons unlikely to have SARS. The CDC surveillance case definition has been revised to include interim criteria for excluding new or previously reported suspect or probable cases of SARS for whom an alternative diagnosis can fully explain the patient's illness (2). Factors that might be considered in assigning alternative diagnoses include the strength of the epidemiologic exposure criteria for SARS, the specificity of the diagnostic tests, and the compatibility of the clinical presentation and course of illness for the alternative diagnosis. The epidemiologic criteria for travel exposure also have been revised and now reflect updated information about the occurrence of community transmission in areas with SARS. Hanoi, Vietnam and Toronto, Canada are now considered areas with previous community transmission of SARS because >30 days have elapsed since the onset of symptoms for the last reported case (4). As a result, travel alerts for these cities were removed on May 15 and May 20, respectively. Persons reporting travel to these areas will meet the surveillance case definition if illness onset occurred within 10 days (i.e., one incubation period) after removal of the travel alert. These revisions to the case definition are for surveillance purposes only. Clinical judgment, rather than surveillance criteria, should continue to guide the management of patients and implementation of public health response measures when persons with an unknown respiratory illness are identified. As state and local health departments review and reclassify cases using these new criteria, case counts might change but the result will more accurately reflect the occurrence of SARS in the United States. Reported by: State and local health departments. SARS Investigative Team, CDC. References
Figure
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/22/2003 |
|||||||||
This page last reviewed 5/22/2003
|