 ShareCompartir
ShareCompartir

Monthy Case Studies - 2002
Case #91 - September, 2002
A 37-year-old man was admitted to the hospital for fever and an inflamed foot. He had spent the previous three months touring South America, southern and eastern Africa, and Kathmandu. Ten days before admission, he visited game reserves in Tanzania, where he reported multiple tsetse fly bites. Six days later, he developed pain in the left foot and high fever. The next day, he noted progressive swelling on the dorsum of the foot and he was evaluated at a clinic in Katmandu. A malaria smear was negative and he was prescribed cephalexin. He continued to have intermittent high fever (to 41°C [105.8°F]) and developed vomiting, headache, myalgia, and a diffuse rash. A repeat malaria smear was negative, but his white cell count was 4000 per mm3 with 10% band forms. He returned to the United States and was admitted to the hospital. A shallow ulceration was present on his left instep, encircled by bullae at the margin and surrounded by purple discoloration. The foot lesion was 5 cm in diameter. The following images show what was observed on a thin film made from EDTA blood. What is your diagnosis? Based on what criteria?
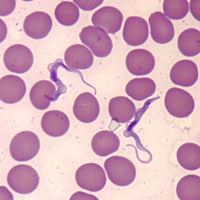
Figure B
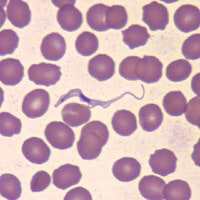
Figure C
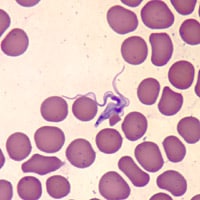
Figure D
Answer to Case #91
This was a case of African Sleeping Sickness (African trypanosomiasis) caused by Trypanosoma brucei rhodesiense. Please note that T. brucei rhodesiense cannot be distinguished from T. brucei gambiense morphologically; travel history helped play a part in a specific diagnosis. Note that the organisms are not C-shaped and do not have a large nucleus or kinetoplast as seen in T. cruzi.
More on: African Trypanosomiasis
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
