 ShareCompartir
ShareCompartir

Monthy Case Studies - 2000
Case #49 - December, 2000
A 10-week-old infant was admitted to a hospital in North Carolina with a recurring fever on September 8, 2000. The baby's parents were from the Democratic Republic of Congo (DRC), but had resided in the United States since 1995. The baby's mother took chloroquine before leaving the DRC. She had traveled to France for a month in 1998. A missionary friend of the family, who had been working in the DRC, visited the family in North Carolina during August 2000. The friend was not ill during his stay. The baby's father reportedly saw and killed a few mosquitoes during the friend's stay. Blood was drawn from the baby on September 9, 2000 and thin blood smears were made and stained with Giemsa (Figures A, B, C, and D). Blood was drawn from the baby's mother on September 10, 2000 and thin blood smears were made and stained with Giemsa (Figures E, F, and G). What is your diagnosis for both the baby and mother? What other tests might be indicated to confirm your diagnosis and/or is there a need for an epidemiological investigation?
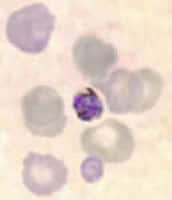
Figure A
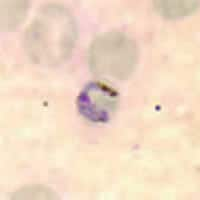
Figure B
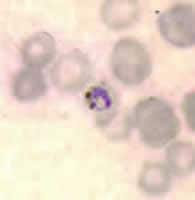
Figure C
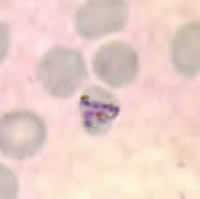
Figure D
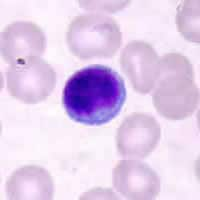
Figure E
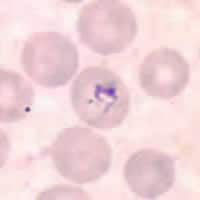
Figure F
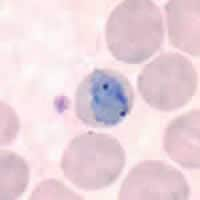
Figure G
Answer to Case #49
This was a case of malaria caused by Plasmodium malariae. Diagnostic features observed on the baby's blood smear were:
- a somewhat oval gametocyte with diffuse pigment (Figure A).
- a developing trophozoite with coarse pigment and a large chromatin mass (Figure B).
- a developing trophozoite with coarse pigment and a large chromatin mass (Figure C). The parasite was a basket-form typically seen in infections with P. malariae with large chromatin mass.
- infected red blood cells smaller than uninfected red blood cells.
Images taken from the mother's smear showed no parasites. Figure E showed a lymphocyte. Figure F showed an artifact somewhat resembling a ring-stage parasite superimposed on a red blood cell. Notice that there is lack of pigment and a red nucleus in this object. Figure G showed an artifact that could be mistaken for a band-form parasite superimposed on a red blood cell. Again, notice the color of the object.
In addition to examining Giemsa stained blood films, both serology and PCR were performed on specimens from the mother. The results were:
- Serology was positive for P. malariae and P. falciparum (both 1:16,384). Results were also positive for P. ovale and P. vivax (both 1:1024).
- PCR was negative.
Malaria due to either mosquito transmission or recrudescence during pregnancy may result in congenital malaria, where Plasmodium organisms are transmitted via the umbilical cord to the fetus. As early as 48 hours after giving birth, the mother's parasitemia may decline to undetectable levels by slide examination and PCR. In patients from endemic areas, serology is not useful for diagnosing current infection with Plasmodium since antibodies may persist for years after treatment. Positive titers indicate infection at some unknown time and the titer level cannot be used to determine the infecting species of a current infection. Because the child had no risk factors for malaria, such as travel to endemic areas or blood transfusions, and the mother was seropositive, the findings are consistent with congenital malaria. Unfortunately, the visiting friend was not available to be tested for malaria. If he had been tested and was positive for P. malariae, the possibility of locally transmitted malaria could also be considered.
More on: Malaria
Images presented in the monthly case studies are from specimens submitted for diagnosis or archiving. On rare occasions, clinical histories given may be partly fictitious.
