
|
|
Volume
2:
No. 3, July 2005
ORIGINAL RESEARCH
Evaluation of Salud Para Su Corazón (Health for Your Heart) — National Council of La Raza Promotora
Outreach Program
Héctor Balcázar, PhD, Matilde Alvarado, RN, MSN, Mary Luna Hollen, PhD, RD, Yanira Gonzalez-Cruz, MPH, Verónica Pedregón
Suggested citation for this article: Balcázar H, Alvarado M, Hollen ML, Gonzalez-Cruz Y, Pedregón V. Evaluation of Salud Para Su Corazón (Health for Your Heart) — National Council of La Raza Promotora outreach program. Prev Chronic Dis [serial online] 2005 Jul
[date cited]. Available from: URL: http://www.cdc.gov/pcd/issues/2005/
jul/04_0130.htm. PEER REVIEWED
Abstract
Introduction
In 2001, the National Heart, Lung, and Blood Institute partnered with the National Council of La Raza
to conduct a pilot test of its community-based outreach program Salud Para Su Corazón (Health for Your Heart),
which aims to reduce the burden of morbidity and mortality associated with cardiovascular disease among Latinos.
Methods
The effectiveness of promotores de salud (community health workers) in improving heart-healthy behaviors among Latino families participating in the pilot program at seven sites was evaluated. Data on the characteristics of the promotores in the Salud Para Su Corazón program were compiled. Promotores collected data on family risk factors, health habits, referrals and screenings, information
sharing, and program satisfaction from 223 participating Latino families (320 individual family members) through questionnaires.
Paired t tests and chi-square tests were used to measure pretest–posttest differences among program participants.
Results
Results demonstrated the effectiveness of the promotora
model in improving heart-healthy behaviors, promoting community referrals and screenings, enhancing information sharing beyond families, and satisfying participants’ expectations of the program. The main outcome of interest was the change in heart-healthy behaviors among families.
Conclusion
The community outreach model worked well in the seven pilot programs because of the successes of the
promotores and the support of the community-based organizations. Successes stemmed in part from the train-the-trainer approach. Promotoria, as implemented in this program, has the potential to be integrated with a medical model of patient care for primary, secondary, and
tertiary prevention.
Back to top
Introduction
Recent epidemiological studies have demonstrated that Latinos may not be as protected from mortality events associated with cardiovascular disease (CVD) as postulated in earlier studies (1). Compared
with non-Hispanic whites, Mexican Americans, who represent the largest percentage of the U.S. Hispanic population, experience equal or greater rates of CVD mortality (2,3). This disparity is
paralleled by the increased prevalence of associated risk factors (e.g., obesity, diabetes, lack of physical activity) for CVD in this and other Hispanic populations (4). The response to combat CVD and its risk factors among Hispanics necessitates the development of culturally competent programs that include community outreach strategies that target underserved and underinsured Hispanic
populations. The Salud Para Su Corazón (SPSC)
(Health for Your Heart) program is one example of a community-based outreach strategy that aims to reduce CVD risk factors and ultimately reduce the burden of mortality associated with CVD among Latinos.
SPSC was developed in 1994 by the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH) as a community-based health promotion model for heart health among Latinos (5-9). The integration of the
promotora de salud (community health worker) model distinguishes SPSC from other heart health programs. The use of community health workers has proven
to be a cost-effective intervention strategy for expanding health access and health care services to underserved and underinsured minority communities, including Latino
communities (10).
In 2001, the NHLBI partnered with the National Council of La Raza (NCLR), the
nation's largest Hispanic grassroots organization, to establish a national pilot dissemination of SPSC programs. The partnership sought to test the
promotora model for promoting heart health and reducing CVD risk factors within seven Latino communities across the country.
Promotores de salud and community-based organizations (CBOs) teamed up to
deliver the culturally competent SPSC health promotion intervention.
The SPSC–NCLR initiative to test the
promotora outreach model had three components: 1) a planning and development phase, 2) an implementation phase, and 3) an evaluation phase. The description of the planning and development phase has been published elsewhere (11). The objectives of the implementation and evaluation phases for the SPSC–NCLR initiative were to 1)
monitor changes in heart health knowledge, attitudes, and skills of promotores; 2) track the delivery of program curriculum and educational sessions by promotores to Latino families; 3) deliver a series of community-educational activities; 4) assess perceptions of CBOs associated with the
promotora model to build community capacity; and 5) evaluate changes in heart-healthy
behaviors reported by Latino family participants. This article describes the SPSC–NCLR pilot dissemination approach, focusing on the implementation and evaluation phases of the initiative, and describes the effectiveness of promotores to improve heart-healthy behaviors among participant Latino families.
Back to top
Methods
The SPSC–NCLR
pilot dissemination approach
The theoretical framework guiding the SPSC–NCLR initiative integrated two major elements: community outreach processes and participatory research methods. This integrated approach guided the development, implementation, and evaluation of the train-the-trainer
promotora model.
Development of the promotora model
The development phase of the SPSC-NCLR initiative consisted of a needs assessment survey of CBOs, which was used for selecting the seven participating sites. These participating sites were CBOs that had promotores working for them. The
Table provides the names and locations of the CBOs. A detailed description of the
development of this model is described elsewhere (11).
Implementation of the promotora model
The implementation phase at each site consisted of 1)
promotora training activities, 2) activities to recruit participant Latino families, and 3) a 6-month intervention delivered by promotores.
Promotora training. A series of well-defined and structured
promotora training activities was conducted and supervised by the SPSC–NCLR team for all seven sites. The activities involved the development of participatory process and capacity building to support the adequate delivery of the interventions (11).
Recruitment of Latino families. Recruitment was primarily the responsibility of the promotores. They recruited families using advertisements developed by their own CBOs, and they enrolled participants from community centers, health centers, schools, and other community and neighborhood sites.
Promotores
approached individual family members and invited them to participate in the
program. All family members were invited to participate in the program; however,
the mother was the most likely participant (91% of the time).
Intervention. The intervention implemented at all seven sites included a series of educational sessions from the
NHLBI heart-health curriculum called Your Heart, Your Life.
Promotores delivered seven of eight curriculum lessons in 2-hour sessions within a 2- to 3-month period
for the first part of a 6-month intervention. The eighth lesson on diabetes was optional. Sessions occurred either several times a week, once a week,
or every other week.
Promotores used a variety of educational materials including workbooks,
fotonovela stories,
easy-to-read booklets, and videos. The intervention also included home-visit or telephone follow-up contacts to reinforce the educational activities learned in the program. More detailed information about this family heart-health education program using Your Heart, Your Life has been reported in a recent article (11). Additional activities under the contracts for the CBOs and their
promotores included referrals to health care providers for health screenings of blood pressure, blood cholesterol, blood glucose, and measures of weight and waist circumference.
The SPSC–NCLR program reached 223 Latino families served by 33 promotores at seven locations across the United States. The majority of the families served by the program resided in California, Illinois, New Mexico, and Texas and were of Mexican origin. Latino families of Central and South American origin were also represented in the communities of Chicago, Ill; Escondido, Calif; and
Providence, RI.
Evaluation of the promotora model
The evaluation framework focused on the content of the program, how it was implemented, and its results. To evaluate the extent to which the SPSC-NCLR
program effected change in awareness, knowledge, and behavior, data were collected
using an evaluation tool called ¡Cuéntamelo!
(Tell me about it!) at three levels: 1) the CBOs, 2) the trained promotores,
and 3) the participating families. Designed to guide and assess program implementation, ¡Cuéntamelo! captures process and outcome data with several instruments. Data sources include
questionnaires completed by promotores, families, and CBOs as well as interviews. A full description of the instruments comprising ¡Cuéntamelo!
(11) as well as evaluation data provided by participating CBOs (12) are
published elsewhere.
This evaluation consisted of analyzing data collected from 33 promotores and 223 families (including
a total of 320 individual family members) across all seven Latino communities. The evaluation focused on the characteristics of the promotores participating in the pilot program; the impact of the intervention on improving heart-healthy behaviors among family participants; the levels of referrals
and screenings resulting from the program; the extent to which family participants shared their newly gained knowledge with others; and degree of participant satisfaction with the program.
Data analysis
Questionnaires were designed to facilitate data entry into a computer database using Epi Info 2002 (Centers for Disease Control and Prevention, Atlanta, Ga). The SPSS statistical
software program (SPSS Inc, Chicago, Ill) was used to do a variety of analyses,
which included calculating frequencies of responses to each question, computing averages and scores, and comparing responses across families and
promotores. Paired t tests and chi-square
tests were used to test for pre–post differences in family habits. Average improvement scores based on pre–post tests and their 95% confidence intervals were also calculated. Data analysis is presented for all sites combined based on several factors: 1) 91% of participants were
women; 2) the mean age of
participants for each site ranged from 30 to 51 years; 3) data on country of origin
were not available for subgroup analysis; and 4) sample size was limited for some sites.
The main outcome variable of interest was the change in heart-healthy behaviors among family contact persons. A pre–post research design without a control group was used because the outreach programs were pilot programs and because of financial and logistic limitations. Families participating in the Your Heart, Your Life educational sessions completed a survey on practices of
heart-healthy behaviors both before and after the sessions. The average time
between the completion of the curriculum and the posttest was 3 months. A 35-item self-report
4-point scale for assessing family habits (0 = never, 3 = always) was used to assess heart-healthy behaviors.
The family habits scale included many items that assessed the frequency with which families engaged in a variety of heart-healthy practices, such as exercise and eating a low-sodium diet.
Two groups of physical activity questions were asked. For the question “What
does the family do to be more active?,” the possible responses included such
activities as walking, dancing, riding a stationary bike, working in the garden,
aerobic dancing, or playing soccer. The second group of physical activity
questions focused on such activities as getting off a bus one or two stops early
and walking and using stairs instead of elevators. Families
could choose to answer “never,” “sometimes,” “usually,” or “always.” Responses were converted for each of the items representing a desirable behavior to a 0–3-point scale with “never” equaling 0 and “always” equaling 3, assuming there were equal distances between responses. Subscores were calculated by adding responses to
individual items on the same topic. An overall score using responses to all items was also computed. For ease of interpretation, scores were converted to a 0–100-point scale in which a high score reflected a higher frequency of always practicing a desirable behavior. Content validity and reliability of these subscales have been reported elsewhere (11,13)
and shown to have good reliability (Cronbach a > 0.60) (13).
Back to top
Results
Promotores
A total of 33 promotores delivered the intervention. The average number of families per promotor(a)
was seven, with a range of 2 to 13 families per promotor(a).
The Table presents the number of promotores working with participant families, the total number of families, and the mean number of families per promotor(a) at each site.
Most promotores were women aged 20 to 67; the average age was 41. About 65% of the promotores were born outside the United States. Of the 33 promotores, 5% reported having attended only primary school or less, 18% reported having some high school education, 28% reported having a high school diploma or GED, 30% reported having some college or technical school
education, and 18%
reported being college graduates. Overall, most promotores reported being bilingual. As would be expected, the preferred language varied depending on whether the promotores were born in the United States; a greater proportion preferred English or English and Spanish if they were born in the United States. Most promotores (78%) had worked as lay health educators before
participating in the SPSC-NCLR program, with experience ranging from 6 months to 20 years.
Improving heart health of families
The location for conducting family education sessions varied slightly depending on the topic; the most common locations were family homes (35%) and community centers (32%). Other locations (e.g., church, school) were also used for about 27% of the family education sessions.
Fewer than 5% of the family education sessions were conducted in health centers. The surveyed families received an average
of about seven educational sessions out of the possible eight. Almost all families (89%) were given information on at least seven topics, including diabetes.
Promotores asked the main respondent for the family, usually the mother, to provide the estimated number of individuals in the family at risk for CVD. Among the main respondents for the 223 families, 57% reported that no one in their family was at risk for CVD; 42% reported that they had at least one family member at risk.
Figure 1 shows CVD risks reported by individual family members. When promotores asked individual family members to report on a list of risk factors, 80% of the 320 individuals surveyed had at least one risk for heart disease. The mean number of risks per family member surveyed, excluding those who reported having no risks, was three. The overall mean number of risks, including the
individuals who reported having no risks, was two. The two most common risks factors for CVD among all individuals surveyed were being overweight (50%) and a lack of physical activity (45%). Only 9% of the respondents reported that they smoked, a low percentage compared
with other factors.
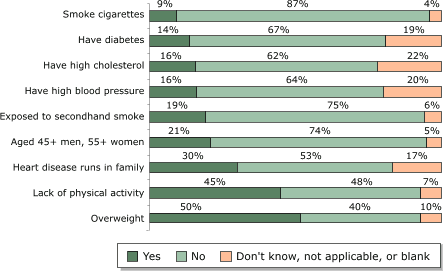
Figure 1.
Heart disease risks reported by individual family members (n = 320) participating in the Salud Para Su Corazón outreach program. Data collected by promotores using questionnaires, 2001.
[A tabular version of this chart is also
available.]
Changes in pretest and posttest scores for the families’ practices of heart-healthy behaviors are presented in Figure 2. Families showed improvement in heart-healthy behaviors. Paired t tests of the increases in average overall scores and for each topic were statistically significant (P < .001). For the 190 families that completed both surveys, the average pretest
overall score was 41% and the average posttest overall score was 59%, representing an average improvement in the total score of 18% (95%
confidence interval [CI], 16%–21%).
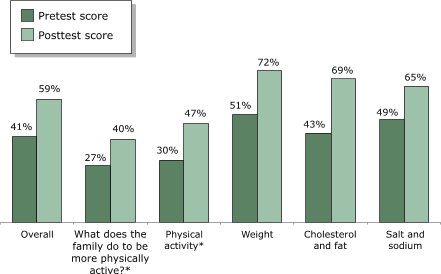
Figure 2.
Average scores, by topic, for heart-healthy habits among families (n = 190) participating in both the pretest and posttest as part of the Salud Para Su Corazón
outreach program. Score percentages calculated based on maximum score of 100.
Asterisk (*) indicates that data refer only to mother. P < .001 for paired t tests on all topics. Data collected by
promotores using questionnaires, 2001. [A
tabular version of this chart is also
available.]
The greatest improvement was observed for the items on practices related to cholesterol and fat, with an average pretest score of 43% and an average posttest score of 69%, an improvement of 26% (95% CI, 23%–30%). On topics such as “What is the family doing to be more physically active?” an average improvement of 13% was found (95% CI, 9%–16%). An improvement of
17% (95% CI, 14%–21%) was found for the physical activity topic. An average improvement of 21% (95% CI, 18%–24%) was found in practices related to weight reduction and control. Improvements were also observed on items related to salt and sodium consumption.
Figure 3 describes the distribution of responses across the four possible response categories. Chi-square tests of changes in the distribution were statistically significant (P < .001), even though this test does not correct for a potential underestimation of the effect due to the correlation between pretest and posttest scores for individual respondents.
Figure 3.
Distribution of responses on family heart-healthy habits among families (n = 190) participating in both the pretest and posttest as part of the Salud Para Su Corazón outreach program. Asterisk
(*) indicates that data refer only to mother. Data collected by promotores using questionnaires, 2001.
Percentages do not add to 100% because of rounding. [A tabular
version of this chart is also
available.]
Community referrals and screenings
Of the 223 families surveyed, promotores referred 74% to health care providers for blood pressure screening and 81% for blood cholesterol screening. They also weighed and measured the waist circumferences of family members for 77% of the families. Among the 101 families that received the educational session on diabetes, 70% were referred for a blood glucose check. According to the data
collected by promotores through the group education
questionnaires, promotores referred participants
in 89% of the 56 classes taught on cholesterol for blood cholesterol screening and
referred participants in 86% of the 37 classes taught on diabetes for blood
glucose screening. Promotores also measured the weight and waist circumferences in 34% of the 32
classes taught on maintaining a healthy weight. No data were collected for blood pressure screenings.
Based on the promotores interviews conducted in 2003, five of the seven sites reported that more than 90% of the participants referred for screening in 2001 were actually screened,
and one of the sites reported that 100% of the participants referred were screened. Another site reported that it did not have this information. To ensure that the participants would be screened after
taking the class, some of the promotores opted for providing transportation to a clinic after the class, while others decided to bring a nurse to the session to do the screening. In other locations, promotores kept track of the percentage of participants who were screened by asking them for the screening results during follow-up visits. In still other locations,
promotores arranged
for free screening of class participants in an effort to increase the number of people getting screened for the different heart risk factors. The interaction between
promotora and screening activities on reducing CVD risk factors was not explored because of limitations in data collection.
Reaching beyond families
According to the data collected from 223 families, SPSC–NCLR reached other people beyond the original participant families.
Responses to
questions on information sharing revealed that family respondents were
likely to share information they learned about heart-healthy behaviors
with friends in their neighborhood, friends in other cities, friends in
their country of birth, relatives in their country of birth, or people at
work. The results showed that family respondents were just as likely to
share information about one topic as another, with the exception of smoking
(Figure 4). Fewer than 33% of families shared information with friends in other cities, friends in their country of birth, relatives in their country of birth, or people at work. The lower proportion of families that shared information about smoking, compared
with
other topics, may reflect the fact that most respondents reported being nonsmokers.
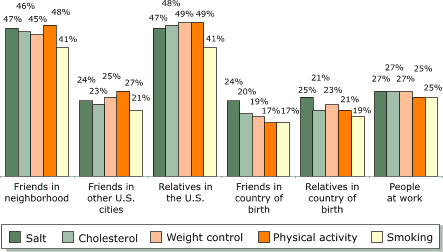
Figure 4.
Audiences with whom families participating in Salud Para Su Corazón outreach program (n = 223) shared educational information received, by topic. Data collected by promotores using questionnaires, 2001.
[A tabular version of this chart is also
available.]
Participants’ evaluations of SPSC–NCLR programs
Family participants expressed a very high level of satisfaction with the program. Overall, of the 207 families
participating in the survey on satisfaction, 96% were very satisfied with the program. Accordingly, the level of satisfaction with specific aspects of the program was also very high (Figure 5).
For example, the majority of the families surveyed (95%) rated the information they received through the program
(instruction and guidance) as very important,
including information on cholesterol and fat, blood pressure, weight control and serving information, physical activity,
smoking, and salt and sodium.
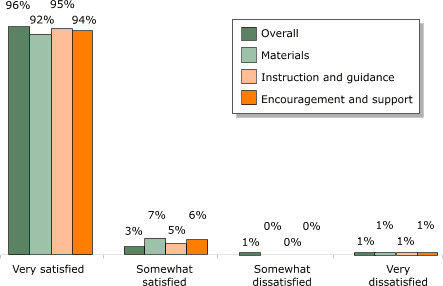
Figure 5. Percentages of families satisfied with guidance provided by the Salud Para Su Corazón outreach program (n = 207). Data collected by promotores using questionnaires, 2001.
[A tabular version of this chart is also
available.]
Back to top
DiscussionSuccesses
The community outreach model worked well in the seven pilot programs because of the successes of the promotores de salud and the support of the CBOs
(12). With their skills, commitment, and enthusiasm, the training program and health education curriculum proved effective, translating into success for the SPSC-NCLR initiative. Overall, the results of the evaluation show that the
initiative resulted in significant accomplishments at all three levels: promotores, families, and CBOs
(12).
The successes realized in promoting heart health stems in part from the train-the-trainer approach. It nurtured the competency of the promotores to ensure success of the intervention. The train-the-trainer approach empowered promotores in their work by broadening their range of instructional approaches and heart-health knowledge. Based on self-reports by promotores and
families, after completing the SPSC training, promotores were able to obtain the knowledge and skills necessary to recruit community members to participate in the program, to pass on the knowledge they had gained, and to support community members in accomplishing lifestyle changes that promoted better heart health.
Promotores also expanded awareness of the project in the
community, solicited additional funding, developed public service announcements related to the teaching materials,
or did all of these. Despite facing a number of challenges, including limited funding and the need to prove the value of their work and that of the SPSC-NCLR program to some health care professionals, they successfully established partnerships with a variety of local organizations and programs, including
clinics and health care providers, churches, schools, radio stations, health professional associations, restaurants, and pharmaceutical companies.
Promotoria, as implemented in the SPSC-NCLR program, has the potential to be integrated with a medical model of patient care for primary, secondary, and tertiary prevention. Using the ¡Cuéntamelo! evaluation tools, promotores successfully identified risks for heart disease at the levels of both families and individuals, referring individuals for screening and
providing community members with the knowledge and skills that they needed to improve their heart health. The capacity of promotores to function as health educators and advocates has important implications for health promotion and disease prevention, given recent evidence that physicians spend less than 10 minutes
per patient delivering educational messages (15).
The ability of promotores to effect behavioral change is evident among the families they served. Evidence suggests families participating in the SPSC-NCLR program made positive changes in heart-healthy behaviors. Families showed an improvement of 18% on self-reported heart-healthy behaviors. It seems that promotores succeeded at improving heart-health awareness and creating a
cultural environment for learning heart-health information to promote changes in lifestyle behaviors among family members. Changes in heart-health behaviors have been consistently observed for similar
promotora educational programs, adding credibility to the
promotora approach (16,17).
According to the CBO survey (11,12), these local organizations supported the SPSC-NCLR program for two main reasons:
the program supported the organization’s mission of enhancing health education and prevention in Latino communities, and
the program facilitated partnerships and provided access to additional human and financial resources. Furthermore, the adaptability of the SPSC-NCLR program
facilitated its implementation at all seven sites. Even though all the sites applied the same SPSC-NCLR program training and materials (including the ¡Cuéntamelo! tools), each site adapted some aspects of the program based upon their needs, the resources available, and the characteristics of the community. For example, some sites focused on conducting group education sessions; others focused on home visits for family education. Thus, SPSC-NCLR appears to be a flexible and adaptable program for use in a variety of settings and with different types of Latino communities (5,13,17,18).
Recommendations
Four recommendations are identified to improve the implementation and evaluation of the SPSC-NCLR program. First, it might be useful to explore how to facilitate health screening and follow-up care for individuals whom promotores identify as being at risk for heart disease. The second recommendation follows from the
difficulties reported by promotores in using videos as educational materials.
These difficulties resulted from a
lack of video equipment on site. It
might be useful instead to use sociodramas based on the video scripts as supplemental educational tools or to replace the video entirely. The use of the videos could also be tested for its effectiveness in promoting awareness and changing behavior.
Third, a distance-training and continuing-education module of
promotora training can be considered, using a Web-based curriculum. It would be
interesting to examine whether this form of training is effective; it might have implications for international use. Finally, a formal evaluation of the SPSC-NCLR program requires a quasiexperimental design or a clinical trial with pretest and posttest comparisons. It should involve evaluation of a series of sociodemographic and acculturation indicators, in addition to biological parameters, including
changes in blood pressure, blood cholesterol, and body mass index. Finally, a formal evaluation should include more distal or secondary outcomes such as screening rates, sales of low-fat foods, and similar aspects in the community at large to indicate whether heart-healthy behaviors are becoming a community norm.
Back to top
Acknowledgments
Funding for this research was provided by Metropolitan Life Foundation.
Back to top
Author Information
Corresponding Author: Héctor Balcázar, PhD, University of Texas Health Science Center at Houston, School of Public Health, El Paso Regional Campus, 1100 N Stanton St, Suite 100, El Paso, TX 79902. Telephone: 915-747-8507. E-mail: Hector.G.Balcazar@.uth.tmc.edu.
Author Affiliations: Matilde Alvarado, RN, MSN, National Heart, Lung, and Blood Institute, National Institutes of Health,
Bethesda, Md; Mary Luna Hollen, PhD, RD, University of North Texas Health Science Center at Fort Worth, School of Public Health, Department of Social & Behavioral Sciences, Fort Worth, Tex; Yanira Gonzalez-Cruz, MPH, National Hispanic Council on Aging,
Washington, DC; Verónica
Pedregón, University of Texas Health Science Center at Houston, School of Public Health, El Paso Regional Campus, El Paso, Tex.
Back to top
References
- Rainwater DL, Mitchell BD, Comuzzie AG, VandeBerg JL, Stern MP, MacCluer JW.
Association among 5-year changes in weight, physical activity, and cardiovascular disease risk factors in Mexican Americans. Am J Epidemiol 2000 Nov 15;152(10):974-82.
- Stern MP, Wei M.
Do Mexican Americans really have low rates of cardiovascular disease? Prev Med 1999 Dec;29(6 Pt 2):S90-5.
- Pandey DK, Labarthe DR, Goff DC, Chan W, Nichaman MZ.
Community-wide coronary heart disease mortality in Mexican Americans equals or exceeds that in non-Hispanic whites: The Corpus Christi Heart Project. Am J Med 2001 Feb 1;110(2):81-7.
- Perez-Stable E, Juarbe T, Moreno-John C. Cardiovascular. In: Aguirre-Molina M, Molina C, Zambrana R, editors. Health issues in the Latino community. San Francisco: Jossey-Bass; 2001. p. 245-76.
- Alcalay R, Alvarado M, Balcázar H, Newman A, Huerta E.
Salud para su Corazón: a community-based Latino cardiovascular disease prevention and outreach model. J Community Health 1999 Oct;24(5):359-79.
- Alcalay R, Alvarado M, Balcázar H, Newman E, Ortiz G. Evaluation of a community-based Latino heart disease prevention program in metropolitan Washington, DC. Int Q Community Health Educ 1999-2000;19(3):191-204.
- Balcázar H, Alvarado M, Alcalay R, Huerta E, Ortiz G. Salud para su Corazón:
a model program to promote cardiovascular health in Latinos. Med Interam 1999;18(1):18-23.
- Balcázar H, Alvarado M, Alcalay R, Schindeldecker M, Newman E, Huerta E, et al. Salud para su Corazón:
evaluating cardiovascular health outreach activities in the Latino community. Medicine of the Americas 2001 Jan/Feb;2(1):4-11.
- National Heart, Lung, and Blood Institute. Latino community cardiovascular disease prevention and outreach initiative. Bethesda
(MD): Public Health Service, National Institutes of Health; 1996.
- Ro MJ, Treadwell H, Northridge M, editors. Community health workers and
community voices: promoting good health [policy brief on the Internet].
Washington (DC): Community Voices; 2003 Oct [cited 2004 Nov 15]. Available from:
URL: http://www.communityvoices.org*.
- Balcázar H, Alvarado M, Luna Hollen M, Gonzalez-Cruz Y, Hughes O, Vasquez E, et al. Salud para su Corazón-NCLR:
a comprehensive promotora outreach program to promote heart-healthy behaviors among Hispanics. Health Promot Pract.
Forthcoming.
- National Heart, Lung, and Blood Institute. Salud para su Corazon
National Dissemination: Evaluation of the implementation of Salud para su
Corazon by lay health educators in seven Latino communities, 2001.
Bethesda (MD): Public Health Service, National Institutes of Health; Sept
2003.
- Medina AY. Does a community health worker program work among Latino communities? [Master in public health thesis]. Fort Worth (TX): University of North Texas Health Science Center at Forth Worth; 2003.
- Tabachnick BG, Fidell LS. Using multivariate statistics. 3rd edition. New York: HarperCollins College Publishers; 1996.
- Russell NK, Roter DL.
Health promotion counseling of chronic-disease patients during primary care visits. Am J Public Health 1993 Jul;83(7):979-82.
- Medina AY, Balcázar H, Luna Hollen M, Nkoma E, Soto Mas F. Community health workers educating Hispanic communities on heart-healthy living.
Forthcoming.
- Balcázar H, Luna Hollen M. Salud para su Corazón of North Texas.
Bethesda (MD): National Institutes of Health, National Heart, Lung, and
Blood Institute; 2004.
- Beam BA. Cardiovascular disease risk factor education in the Hispanic population [Master of science in nursing thesis]. San Diego (CA): San Diego State University; 2003.
Back to top
|
|
