
|
|
Volume 1:
No. 3, July 2004
COMMENTARY
Prevention Health Care
Quality in America: Findings From the First National Healthcare Quality and
Disparities Reports
Ed Kelley, PhD, Ernie Moy, MD, MPH, Beth Kosiak, PhD, Dwight McNeill,
PhD, Chunliu Zhan, MD, PhD, Dan Stryer, MD, Carolyn Clancy, MD
Suggested citation for this article: Kelley E,
Moy E, Kosiak B, McNeill D, Zhan C, Stryer D, et al. Prevention health
care quality in America: findings from the first National Healthcare Quality
and Disparities Reports. Prev Chronic Dis [serial online] 2004
Jul [date cited]. Available from: URL: http://www.cdc.gov/pcd/issues/2004/
jul/04_0031.htm.
Introduction
The Agency for Healthcare Research and Quality (AHRQ) released in
December 2003 the first
National Healthcare Quality Report (NHQR) and National Healthcare
Disparities Report (NHDR) on behalf of the U.S. Department of Health and
Human Services (1,2). In this commentary, we
summarize the main findings of the reports on preventive care for both
primary prevention of disease and secondary prevention of increasing acuity
of existing disease and discuss the implications for quality measurement and
improvement efforts.
Federal partners within the U.S. health care system have recently focused
on increasing the use of preventive care services. Tommy G. Thompson,
Secretary of Health and Human Services, issued a challenge in April 2003 at the
launch of the Steps to a HealthierUS
national initiative:
"Approximately 95% of the $1.4 trillion that we spend as a nation on
health goes to direct medical services, while approximately 5% is allocated
to preventing disease and promoting health. This approach is equivalent to
waiting for your car to break down before you take it in for maintenance. By
changing the way we view our health, the Steps initiative helps move
us from a disease care system to a true health care system." (3)
Good quality preventive care holds the promise of greatly reducing the
nation’s health care costs and overall burden of disease. Numerous studies
and reports have examined the general quality of preventive care services in
the United States (4-7). Others have explored the performance of the U.S.
health care system in delivering specific preventive care services such as
immunizations (8,9), cancer screening (10-12), and cholesterol and blood
pressure screening (13-15).
The NHQR and NHDR provide the first national baseline views of the
quality of health care services and of differences in how at-risk groups in
America use the services. The reports provide one of the broadest
examinations to date of prevention health care quality for the nation and
among key priority populations, measuring quality of care across a range of
dimensions, including the degree to which care is safe, patient centered,
timely, and effectively delivered. They track more than 50 primary and
secondary prevention quality-of-care measures in five clinical areas,
including cancer, diabetes, heart disease, maternal and child health, and
respiratory disease.
Back to top
Findings of the NHQR and NHDR
Table 1 summarizes the major conclusions of the two reports: the promise
of high-quality health care is not a given, gaps in quality are particularly
acute for certain racial, ethnic, and socioeconomic groups, and improvement
is possible.
NHQR findings
In general, progress has been mixed at best in preventive care service
quality. For example, performance has deteriorated or not improved for three
quarters of the 21 prevention quality measures in which trend data are available.
Similarly, the reports track a set of measures assessing the rate of
hospital admissions for conditions that often can be managed in an
ambulatory care setting with proper primary and secondary preventive care.
Seven of the 10 preventable hospitalization measures with trend data have
either not improved or deteriorated. In addition, while hospital discharge
rates declined from 1997 to 2000 for uncontrolled
diabetes (by 30%) and for pediatric gastroenteritis (by 16%),
pediatric asthma discharge rates did not change in a statistically
significant way (18).
In some areas, however, prevention health care quality has improved. For
example, the incidence rate of new cases of cervical and colorectal cancers
detected at an advanced stage has been declining for decades. The percentage of institutionalized
adults (persons in long-term care or nursing homes) who have ever received
pneumococcal vaccination, while still low at 33% (1999), has improved from
25% (1997). More than 73% of children aged 19 to 35 months have all their
recommended vaccinations. And 83% of women obtain prenatal care in their
first trimester.
NHDR findings
Significant differences exist in the use of evidence-based preventive
services for certain populations, particularly people of lower socioeconomic
status (SES) and some minorities. For example:
- People of lower SES and some minorities are less likely to have
colorectal and breast cancer screening.
- People of lower SES and Hispanics are less likely to have blood
pressure and cholesterol screening in addition to counseling and treatment
for some cardiac risk factors.
- People of lower SES and blacks are less likely to have recommended
childhood immunizations before the age of four years.
- Children of lower SES and some minority children are less likely to
have dental care.
- Lower-SES, black, and Hispanic adults are less likely to have
recommended immunizations for influenza and pneumococcal disease.
Preventive care for specific diseases
NHQR and NHDR findings for cancer, diabetes, and heart disease are
presented below.
Cancer
Cancer screening allows for the detection of precancerous
abnormalities and the early detection of disease and, when followed by
appropriate treatment, can lead to a reduction in the likelihood of illness
and death. The reports track performance in cancer screening for breast,
colorectal, and cervical cancer (Figure). A majority of women 40 and older (70%) is screened with mammography for breast cancer, which
already meets the Healthy People 2010 objective, although this
clearly does not approach the theoretical limit of 100%. The rate of screening for
colorectal cancer (33% for fecal occult blood testing and 39% for flexible
sigmoidoscopy) is less than half that for cervical cancer
screening (81%) and has a long way to go to meet the Healthy People 2010
goal of 50%.
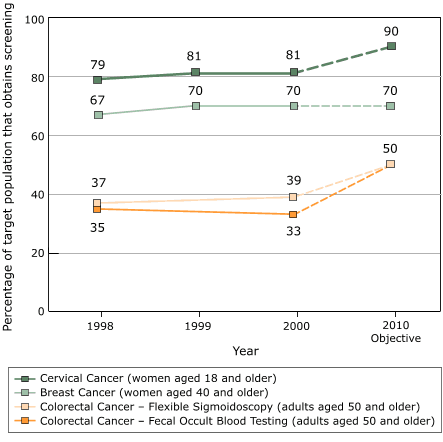
Figure. Cancer screening rates, 1998–2000,
National Healthcare Quality Report. Data not available for colorectal
screening rates for 1999. Data from National Health Interview
Survey, 2000 (19).
Diabetes
High quality of care for diabetes requires that
people with diabetes receive the tests, exams, and treatments that can help
them and their providers manage their condition. Table 2 shows variability
in the rate of delivery of services across the five process measures of
care, ranging from a low of 54.8% for influenza immunization to a high of
94.3% for a lipid profile test. Of particular note is that only 23% of
people with diabetes get all recommended secondary preventive services.
Heart disease
The reports track performance in screening for high
blood pressure and high cholesterol and in delivering smoking cessation
counseling.
Blood pressure screening. Ninety percent of Americans reported having
their blood pressure checked in the past two years. According to 1998 data
from the Centers for Disease Control and Prevention’s National
Health Interview Survey (NHIS), women (93%) and older adults (92%) are
more likely to be checked; Hispanics are screened at lower rates (84%)
(21).
Cholesterol screening. Cholesterol screening rates have
increased in the last two decades. According to 1998 NHIS data, 67% of
adults had their cholesterol checked within the previous five years and
more than 80% of adults aged 45 or older had their cholesterol checked
(21).
Counseling smokers to quit. In 2000, 62% of smokers who had a
routine office visit reported that their doctors had advised them to
quit. According to 2000 NHIS data, individuals who report poor to fair
health are more likely to be counseled to quit (75%) than those who
report good to excellent health (58%) (19). Furthermore, less than half (42%) of
acute myocardial infarction (AMI) patients who smoke are counseled to
quit while in the hospital. AMI patients who are counseled to quit
smoking while in the hospital are more likely than those counseled in
other settings to be abstinent from smoking a year later (20).
Back to top
Conclusions and
Implications
The NHQR and NHDR are two of the most comprehensive national assessments
of preventive care quality in the United States. They show that the U.S.
health care system is missing numerous opportunities to provide
evidence-based preventive care and that usage rates for a number of
preventive care services are not improving. Significant progress is needed
in areas such as colorectal cancer screening, delivery of the full
complement of diabetes secondary preventive services, and cessation
counseling for smokers, particularly when they are admitted to the hospital
for heart attacks.
The purpose of the reports, according to the Congressional mandate that
created them, is to document the state of health care quality for the
nation. The reports do not address the determinants of health care quality,
nor do they prescribe how quality of care could be improved or suggest a
national agenda for improving quality. Many public and private entities
address these important research, policy, and quality-improvement questions.
The reports contribute to the quality-improvement cycle by providing
national information on the state of health care quality, potential
benchmarks, and changes that have occurred over time to support a broad
community of concerned quality-improvement professionals. Information is
critical to helping this broad community understand how gaps and
opportunities apply to their own local needs and facilitate their move
from data to action. The reports offer more than 525 tables that provide
essential information for researchers to analyze the important questions
about why performance is the way it is. The reports can help policy makers
formulate an agenda for quality by creating understanding about the greatest
needs among a wide variety of concerns. Similarly, the reports can serve as
a scorecard on the collective performance of all those involved in quality
improvement.
In addition to tracking health care quality through the reports, the AHRQ
supports quality improvement for the nation by conducting research to
determine evidence-based prevention practices, translating research into
knowledge, and facilitating the use of knowledge toward the goal of
improving the quality of prevention services for all Americans.
Back to top
Author Information
The views expressed in this article are those of the authors and do not
necessarily reflect those of the Agency for Healthcare Research and Quality
or the U.S. Department of Health and Human Services.
Corresponding author: Ed Kelley, PhD, Director, National Healthcare
Quality Report, Agency for Healthcare Research and Quality, 540 Gaither Rd,
Suite 300, Rockville, MD 20850. Telephone: 301-427-1321. E-mail:
ekelley@ahrq.gov.
Author affiliations: Ernie Moy, MD, MPH, Beth Kosiak, PhD, Dwight McNeill,
PhD, Chunliu Zhan,
MD, PhD, Dan Stryer, MD, Carolyn Clancy, MD, Agency for Healthcare Research and Quality,
Rockville, Md.
Back to top
References
- U.S. Department of Health and Human Services. National healthcare
quality report. Rockville (MD): Agency for Healthcare Research and
Quality; 2003. Available from: URL: http://www.qualitytools.ahrq.gov/qualityreport/
download_report.aspx*.
- U.S. Department of Health and Human Services. National healthcare
disparities report. Rockville (MD): Agency for Healthcare Research and
Quality; 2003. Available from: URL: http://www.qualitytools.ahrq.gov/disparitiesreport/
documents/DisparitiesLtr.htm*.
- U.S. Department of Health and Human Services. Steps to a healthier
U.S. Washington (DC): Office of Public Health Promotion; 2001. Available
from: URL: http://www.healthierus.gov/steps/steps_brochure.pdf*.
- Chassin MR, Galvin RW.
The urgent need to improve health care quality.
Institute of Medicine National Roundtable on Health Care Quality. JAMA
1998;280 (11):1000-5.
- McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristotaro A, et al.
The quality of health care
delivered to adults in the United States. N Engl J Med
2003;348 (26):2635-45.
- Leatherman S, McCarthy D. Quality of health care in the United States:
a chartbook. New York (NY): The Commonwealth Fund; 2003 Apr. 164 p.
- Janes GR, Blackman DK, Bolen JC, Kamimoto LA, Rhodes L, Caplan LS,
et al.
Surveillance for use of preventive health-care services by older
adults, 1995-1997. MMWR Surveill Summ 1999 Dec
17;48 (8):51-88.
- Centers for Disease Control and Prevention.
National, state and urban
area vaccination coverage levels among children aged 19-35 months —
United States, January-December 1995. MMWR Morb Mortal Wkly
Rep 1997;46 (8):176-82.
- Kottke TE, Solberg LI, Brekke ML, Cabrera A, Marquez MA.
Delivery rates for
preventive services in 44 midwestern clinics. Mayo Clin Proc 1997;72 (7):515-23.
- Hawley ST, Vernon SW, Levin B, Vallejo B.
Prevalence of colorectal
cancer screening in a large medical organization. Cancer Epidemiol
Biomarkers Prev 2004 Feb;13 (2):314-9.
- Goel MS, Wee CC, McCarthy EP, Davis RB, Ngo-Metzger Q, Phillips RS.
Racial and ethnic disparities in cancer screening: the importance of
foreign birth as a barrier to care. J Gen Intern Med 2003
Dec;18 (12):1028-35.
- Janz NK, Wren PA, Schottenfeld D, Guire KE.
Colorectal cancer
screening attitudes and behavior: a population-based study. Prev Med
2003 Dec;37 (6 Pt 1):627-34.
-
State-specific cholesterol screening trends — United States, 1991-1999. MMWR Morb Mortal Wkly Rep 2000 Aug 25;49 (33):750-5.
- Lin T, Chen CH, Chou P. Impact of the high-risk and mass strategies on
hypertension control and stroke mortality in primary health care. J Hum Hypertens 2004 Feb;18 (2):97-105.
- Sheridan S, Pignone M, Donahue K.
Screening for high blood pressure: a
review of the evidence for the U.S. Preventive Services Task Force.
Am J Prev Med 2003 Aug;25 (2):151-8.
- Soumerai SB, McLaughlin TJ, Spiegelman D, Hertzmark E, Thibault G,
Goldman L.
Adverse outcomes of underuse of beta-blockers in elderly
survivors of acute myocardial infarction. JAMA 1997 Jan
8;277 (2):115-21.
- Ries LAG, Eisner MP, Kosary CL, Hankey BF, Miller BA, Clegg L,
et al, editors. SEER Cancer Statistics
Review, 1975-2000. Bethesda (MD): National Cancer Institute; 2003.
Available from: URL: http://seer.cancer.gov/csr/1975_2000/*.
- Centers for Disease Control and Prevention, National Center for Health
Statistics.
National Hospital Discharge Survey. Hyattsville (MD): The
Centers;1998-2000.
- Centers for Disease Control and Prevention, National Center for Health
Statistics. National Health Interview Survey. Hyattsville (MD): The
Centers;2000.
- Agency for Healthcare Research and Quality. Medical Expenditure Panel
Survey (MEPS). Rockville (MD): The Agency:2000.
- Centers for Disease Control and Prevention, National Center for Health
Statistics. National Health Interview Survey. Hyattsville (MD): The
Centers;1998.
Back to top
Tables
 Table 1. Table 1.
General Summary of Health Care in the United States, National Healthcare
Quality Report and National Healthcare Disparities Report, Agency for
Healthcare Research and Quality, 2003
High-quality health care is not a given in
the U.S. health care system.
- Thirty-seven of 57 areas with trend data
presented in the NHQR have either shown no improvement or have
deteriorated.
- Only 23% of individuals with hypertension have
it under control. Control of hypertension is essential to
continued successes in reducing mortality from heart disease,
stroke, and complications of diabetes.
- Half of the people with depression stop using
their medicines within the first month, far shorter than is
recommended by experts and scientific evidence.
- In terms of patient safety, about one in five
elderly Americans was prescribed medications that may have been
inappropriate for them and potentially harmful.
|
Gaps in health care quality are particularly
acute for certain racial, ethnic, and socioeconomic
groups.
- Blacks and Hispanics experience worse quality
of care for about half of the quality measures reported in the
NHQR and NHDR.
- Hispanics and Asians experience worse access to
care for about two thirds of access measures.
- Poor people experience worse care for about two
thirds of the quality and access measures.
|
Improvement in quality and disparities is
possible.
- Chosen as a national priority for improvement
by the Medicare QIO program, the use of beta blockers for heart
attack patients rose from 21% of eligible patients in the early
1990s (16) to 79%a. In addition, improvement on this
measure has been relatively universal. Fully 45 states are at or
above 70% on this measure.
- A majority of women older than 40 years (70.3%) is being screened by mammography for breast cancer, exceeding
the Healthy People 2010 objective.
- Black women have higher screening rates for
cervical cancer, perhaps related to significant investments in
community-based cancer screening and outreach programs for
cervical cancer. This data may help explain why death rates among
black women, although still more than twice those of white women, have
been decreasing at about twice the rate (17).
- Quality improvement efforts have resulted in
demonstrable reductions in black/white differences in hemodialysis. A targeted intervention within a quality
improvement culture may offer important lessons in disparity
reduction.
|
|
a This measure is the percentage of AMI
patients that are prescribed beta blockers at discharge.
Table 2.
Process Measures of Quality Care for Diabetes in Adults Aged 18 and Older,
United States, 2000a
| Measure |
Estimate |
SE |
|
Percent of adults age 18+ with diabetes who reported receiving influenza
immunization in past year |
54.8 |
2.2 |
|
Percent of adults age 18+ with diabetes who reported having a foot examination
in past year |
66.4 |
1.73 |
|
Percent of adults age 18+ with diabetes who reported having a retinal eye
examination in past year |
66.5 |
1.76 |
|
Percent of adults age 18+ with diabetes who reported having a hemoglobin A1c
measurement at least once in past year |
89.8 |
1.27 |
|
Percent of adults age 18+ with diabetes who reported receiving a lipid profile
in past two years |
94.3 |
0.87 |
| Percent of adults age 18+ with diabetes who reported having
all five major tests done in the past two years |
23.1 |
1.5 |
|
aData from Medical Expenditure Panel Survey,
2000 (20).
Back to top |
|
