Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
The Effectiveness of Universal School-Based Programs for
the Prevention of Violent and Aggressive Behavior
A Report on Recommendations of the Task Force on Community
Preventive Services*
Prepared by
Robert Hahn, PhD1
Dawna Fuqua-Whitley, MA1
Holly Wethington, PhD1
Jessica Lowy, MPH1
Akiva Liberman, PhD2
Alex Crosby, MD3
Mindy Fullilove, MD4
Robert Johnson, MD5
Eve Moscicki, ScD6
LeShawndra Price, PhD6
Susan R. Snyder, PhD1
Farris Tuma, ScD6
Stella Cory, MD1
Glenda Stone, PhD1
Kaushik Mukhopadhaya, PhD1
Sajal Chattopadhyay, PhD1
Linda Dahlberg, PhD2
1Division of Health Communication and Marketing, National Center for Health Marketing, CDC
2National Institute of Justice, Washington, District of Columbia
3Division of Violence Prevention, National Center for Injury Prevention and Control, CDC
4Columbia University, New York, New York, and Task Force on Community Preventive Services
5New Jersey Medical School, Department of Pediatrics, Newark, New Jersey, and Task Force on Community Preventive Services
6National Institute of Mental Health, Bethesda, Maryland
The material in this report originated in the National Center for Health Marketing, Jay M. Bernhardt, PhD, Director; and the Division of
Health Communication and Marketing, Cynthia E. Baur, PhD, Director.
Corresponding preparer: Robert A. Hahn, PhD, National Center for Health Marketing, 1600 Clifton Road, MS E-69, Atlanta, GA 30333.
Telephone: 404-498-0958; Fax: 404-498-0989; E-mail:
rah1@cdc.gov.
Summary
Universal school-based programs to reduce or prevent violent behavior are delivered to all children in classrooms in
a grade or in a school. Similarly, programs targeted to schools in high-risk areas (defined by low socioeconomic status or
high crime rates) are delivered to all children in a grade or school in those high-risk areas. During 2004--2006, the Task
Force on Community Preventive Services (Task Force) conducted a systematic review of published scientific evidence
concerning the effectiveness of these programs. The results of this review provide strong evidence that universal school-based
programs decrease rates of violence and aggressive behavior among school-aged children. Program effects were demonstrated at
all grade levels. An independent meta-analysis of school-based programs confirmed and supplemented these findings. On
the basis of strong evidence of effectiveness, the Task Force recommends the use of universal school-based programs to prevent
or reduce violent behavior.
Background
Youth violence is a substantial public health problem in the United States. In a representative national
survey conducted in 2003, U.S. adults reported approximately 1.56 million incidents of victimization by
perpetrators estimated to be aged 12--20 years, representing a rate of approximately 4.2 incidents per 100 persons in this age
group
(1,2). Two thirds of reports by victims concerned "simple assaults" (i.e.,
attacks without a weapon and not resulting in an injury requiring >2 days of hospitalization). The remaining victimizations were "serious violent crimes" (i.e.,
rape, sexual assault, robbery, or aggravated assault). Because survey
respondents were crime victims, murder was not
included. Since the 1980s, youths aged 10--17 years, who constitute <12% of the U.S. population, have been involved
as offenders in approximately 25% of serious violent victimizations
(3). Homicide and suicide are the fourth and
fifth leading causes of death respectively among children aged 5--14 years and the second and third leading causes of
death among persons aged 15--24 years (4).
Risk factors for youth violence include low socioeconomic status (SES), poor parental supervision, harsh and
erratic discipline, and delinquent peers (3). Delinquent youths commonly have additional problems
(5), including drug abuse, difficulties at school, and mental health problems (as indicated by being in the top 10% of the distribution
of externalizing and internalizing symptoms in the Child Behavior Checklist)
(6). These youths are threats not only because of the direct harm they cause but also because of the role they might play in the socialization of
other potential delinquents (7).
The prevention of youth violence and aggression is of value in itself and also because early violent and
aggressive behavior is a precursor of later problem behaviors
(8). Researchers categorize risk factors for early childhood
delinquency, including violent behavior, as individual, family, peer, school, neighborhood, and media. Factors in all categories
are thought to contribute to the development of early and chronic violent behavior, and all are thought to
provide opportunities for intervention to reduce the development of these behaviors
(9).
The most serious forms of violent crime (i.e., rape, sexual assault, robbery, aggravated assault, and homicide)
rarely occur in schools (10). During July 1992--June 2000, an annual average of 29 homicides and five suicides
occurred throughout U.S. schools, representing <1% of the homicides among youths aged 5--19 years and <0.5% of
suicides among youths away from schools during the same period
(10). However, a disproportionate amount of nonfatal
crime occurred in school facilities or on the way to or from school. Although rates of violent crime declined during
1993--2003, in 2003, approximately 740,000 violent crimes were committed at schools against adolescents aged 12--18
years (rate: 1.3 per 100 persons) (10). Of these crimes, approximately 150,000 (20.3%) were classified as "serious."
The Task Force review assessed the effectiveness of universal school-based programs in reducing or preventing
violent and aggressive behavior among children and adolescents. These programs teach all students in a school or school
grade about the problem of violence and its prevention or about one or more of the following topics or skills intended
to reduce aggressive or violent behavior: emotional self-awareness, emotional control, and self-esteem; positive
social skills; social problem solving; conflict resolution; and team work.
As used in this report, "universal" means that programs are administered to all children in classrooms regardless
of individual risk, not only to those who already have manifested violent or aggressive behavior or risk factors for
these behaviors. Although meriting separate review because youths who manifest violence or aggressive behavior at young
ages are at greater risk for later violence, programs that target youths who already have manifested problems of violence or
are considered at high risk for violence were not evaluated in this review.
Universal programs might be targeted by grade or school in high-risk areas (defined by residents' low SES,
commonly indicated by the proportion of school children receiving subsidized lunches, or high crime rates, as noted by
study authors describing the school community). Programs
are delivered to all children in those settings. Programs
also might be implemented in special schools (e.g., schools for children with specific disabilities). Prekindergarten,
kindergarten, elementary, middle, and junior and senior high school settings were included in this review.
Universal school-based programs are founded on multiple theoretical approaches
(11,12). Theories of behavior change vary in their focus on individuals; interpersonal
relations; the physical and social environment, including social
norms; and combinations of these. Certain programs focus on providing information about the problem of violence
and approaches to avoiding violence, on the assumptions that providing this information to students will lead to
its application and subsequently to reduced violence and that information is necessary, if not sufficient, to change
behavior. For example, the Violence Prevention Curriculum for Adolescents
(13) is designed to teach students about the causes
of violence; knowledge of violence resistance skills is taught through discussion. Other programs
(14) assume that self-concept and self-esteem derive from positive
action and its rewards, so if children's behavior can be made more
positive and sociable, they will develop better attitudes toward themselves and then continue to make positive choices. In
the
Second Step program (15), teaching and discussion are accompanied by role playing,
modeling, skill practice, feedback, and reinforcement.
Certain programs (e.g., Responding in Peaceful and
Positive Ways [16] and Students for Peace
[17]) cite social learning theory
(18) as the foundation for their intervention design. Other programs are founded on the theory that they will
be most effective if they modify the broader environment of the child. In the elementary school PeaceBuilders program,
in addition to the classroom curriculum, the entire school is involved, both outside and inside the classroom, together
with parents and the community; in the school setting, conditions that provoke
aggressive behavior are mitigated, and the following of simple positive behavioral rules, such as "praise people" and "right wrongs," is encouraged and
rewarded (19). The Safe Dates Program includes a 10-session classroom curriculum, a theatrical production performed
by students, a poster contest, community services for adolescents in abusive relationships (e.g., support groups
and materials for parents), and training for community service providers
(20). School antiviolence programs often
are associated with manuals, which facilitate reliable implementation; manuals often are available commercially.
Introduction
The independent, nonfederal Task Force on Community Preventive Services leads work on the Guide to
Community Preventive Services, a resource that includes multiple systematic reviews, each focusing on a preventive health
topic. Work on the Community Guide is supported by the U.S. Department of Health and Human Services (DHHS)
in collaboration with public and private partners. Although CDC provides staff support to the Task Force for
development of the Community Guide, the recommendations presented in this report were developed by the Task Force and are
not necessarily the recommendations of DHHS or CDC.
Community Guide findings are prepared and released as each is completed. Reports of systematic reviews
have already been published on improving coverage with universally recommended and targeted vaccines, tobacco
use prevention and reduction, reducing
motor-vehicle--occupant injury, increasing physical activity, diabetes
management, improving oral health, skin cancer prevention, other aspects of violence prevention, and the effects of the
social environment on health. A compilation of Community Guide systematic reviews has been published in book form
(22). Additional information regarding the Task Force and the Community Guide and a list of published articles are
available on the Internet at http://www.thecommunityguide.org.
The interventions reviewed might be useful in reaching certain objectives specified in
Healthy People 2010 (23), which outlines the disease prevention and health promotion agenda for the United States. These objectives identify
certain important preventable threats to health and focus the efforts of public health systems, legislators, and law
enforcement officials on addressing those threats. Universal school-based programs and their proposed effects on
violence-related outcomes are relevant to multiple
Healthy People 2010 objectives regarding injury and violence
prevention (Table 1).
Methods
Community Guide systematic reviews summarize evidence on the effectiveness of interventions in improving
selected health-related outcomes. Positive or negative
effects of the intervention other than those assessed for the purpose
of determining effectiveness (including positive or negative health and nonhealth outcomes) also are considered
(24,25). When an intervention is shown to be effective in changing a selected outcome, information also is included on
the applicability of evidence (i.e., the extent to which available effectiveness data might apply to diverse
population segments and settings), the economic impact of the intervention, and barriers to implementation.
As with other Community Guide reviews, the process used to conduct a systematic review of the evidence and
to develop conclusions involved 1) forming a systematic
review development team, 2) developing a conceptual
approach to organizing, grouping, and selecting interventions, 3) selecting interventions to evaluate, 4) searching for and
retrieving evidence regarding each intervention, 5) assessing the quality of and abstracting information from each study,
6) assessing the quality of and drawing conclusions about the body of evidence on effectiveness, and 7)
translating the evidence on effectiveness into recommendations.
The present review was produced by the systematic
review development team (the team) and a multidisciplinary
team of specialists and consultants representing various perspectives on violence. This review included studies that
assessed directly measured violent outcomes, specifically self- or other-reported or observed aggression or violence,
including violent crime. The review also included studies that examined any of five proxies for violent outcomes that include
not only clearly violent behavior but also behavior that is not clearly violent:
measures of conduct disorder (the psychiatric condition, in which the rights of others or major societal norms
or rules are violated) (26);
measures of externalizing behavior (i.e., rule-breaking behaviors and conduct problems, including physical
and verbal aggression, defiance, lying, stealing, truancy, delinquency, physical cruelty, and criminal acts)
(27);
measures of acting out (i.e., aggressive, impulsive, or disruptive class behaviors) or conduct
problems (includes talking in class, stealing, fighting, lying, not following directions, teasing, and breaking things);
measures of delinquency (which might include violent behavior and behavior not regarded as violent); and
school records of suspensions or disciplinary referrals.
The purpose of this review was to assess the effectiveness of school-based programs in reducing or preventing
violent behavior. Thus, studies of school-based programs were included only if they assessed violent outcomes or proxies
for violent outcomes and if the reduction of violent or
aggressive behavior was an objective of the program
(although it need not have been the only or principal
objective). The effects on other outcomes were not systematically assessed, but
are reported if they were addressed in the studies reviewed.
Electronic searches for literature on universal school-based programs were conducted during June--July 2002
and updated in December 2004. Databases searched included MEDLINE, EMBASE, Education Resources
Information Center (ERIC), Applied Social Sciences Index and Abstracts, National Technical Information Service (NTIS),
PsycINFO, Sociological Abstracts, National Criminal Justice Reference Service (NCHRS), and Cumulative Index to Nursing
and Allied Health Literature (CINAHL).†
The team also reviewed the references listed in retrieved articles, and specialists on the systematic review
development team and elsewhere were consulted. Studies reported in journal papers, governmental reports, books, and book
chapters were eligible for review.
Articles published before December 2004 were considered for inclusion in the systematic review if they evaluated
a universal school-based program, assessed at least one of the violent outcomes specified previously, were conducted
in countries with high-income
economies,§ and compared persons exposed to the intervention with persons who had
not been exposed or who had been less exposed. Studies with a sample size <20 students were excluded
because results from such studies were not considered
reliable. While searching for evidence on violent outcomes, the team also
sought information about effects on other outcomes not related to violence (e.g., changes in school performance and
drug abuse).
Each study that met the initial inclusion criteria became a candidate for the review and was read by two reviewers
who used standardized criteria (available at
http://www.thecommunityguide.org/methods/abstractionform.pdf)
to assess the suitability of the study design and threats to validity
(24,25). Disagreements between the reviewers were reconciled
by consensus of the development team members. The team's classification of the designs of studies
reviewed is in accord with standards of the Community Guide review process and sometimes differs from the classification used in the
original studies. Studies with the greatest design suitability are those in which data on exposed and control populations
are collected prospectively. Studies with moderate design suitability are those in which data are collected retrospectively
or that have multiple pre- or postmeasurements but no concurrent comparison population. Studies with least
suitable designs are those with no separate comparison population and only a single pre- and postmeasurement in
the intervention population. On the basis of the number of threats to validity, studies were
assigned a number of penalties and characterized as having good, fair, or limited execution for the purposes of this
review (24). Studies with good or fair quality of execution and any level of design suitability (greatest, moderate, or least) were included in the body
of evidence.
Baselines and relative percentage change were calculated using the following formulas:
For studies with before-and-after measurements and concurrent comparison groups:
Effect size = (Ipost /
Ipre)/(Cpost /
Cpre) -- 1
where: Ipost = last reported outcome rate in the intervention group after the intervention,
Ipre = reported outcome rate in the intervention group before the
intervention, Cpost = last reported outcome rate in the comparison
group after the intervention, and Cpre = reported outcome rate in the comparison group before the intervention.
For studies with post measurements only and concurrent comparison groups:
Effect size = (Ipost -
Cpost) / Cpost
For studies with before-and-after measurements but no concurrent comparison:
Effect size = (Ipost -
Ipre) / Ipre
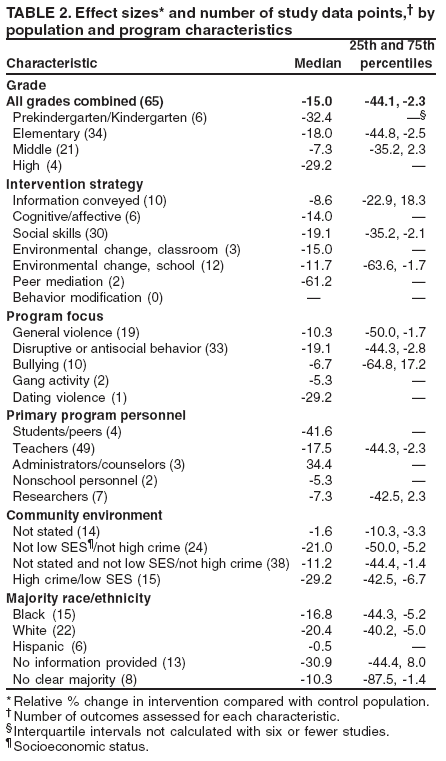
To report effect sizes from multiple studies, the team used the median and, if seven or more effect sizes existed,
the lower quartile, Q1 (the 25th percentile), and the upper quartile,
Q3 (the 75th percentile). Q1
and Q3 provide information on the range of the middle 50% of the study effect sizes and therefore can be interpreted as reflecting
the range of typical effects.
The strength of the body of evidence was summarized on the basis of the number of available studies, the strength
of their design and execution, and the size and consistency of reported effects
(24). When the number of studies and their design and execution quality were sufficient by Community Guide standards to draw a conclusion on effectiveness,
the results were summarized statistically and graphically.
If an intervention was determined to be effective, evidence was assessed regarding its applicability in diverse
settings, populations, and circumstances, noting whether it had been applied specifically in different conditions (e.g., to
white and minority populations or to younger and older children). The goal of this assessment was to determine the
conditions under which the intervention was effective and thus the known limits of its application.
As noted, this review did not systematically assess the effects of a violence prevention intervention on other
outcomes (e.g., drug abuse, school achievement, truancy, or psychological adjustment). However, some of the benefits of
the intervention mentioned in reviewed studies are noted. The potential harms of school-based violence prevention
programs also are noted if these harms were mentioned in the effectiveness literature or were judged by the team to be
of importance.
Barriers to implementation are summarized only if an intervention was demonstrated to be effective.
Similarly, economic evaluations of interventions were conducted only when evidence of effectiveness was identified. Methods
used in Community Guide economic evaluations have been
described previously (28,29).
Systematic reviews in the Community Guide identify existing information on which to base public health
decisions about implementing interventions. An additional benefit of these reviews is identification of areas in which
information is lacking or of poor quality. To summarize these research gaps, the team identifies remaining research
questions for each intervention evaluated.
Results
The team identified 53 studies
(14,15,20,30--79) of universal school-based programs that met the criteria to
be included in the review. Of these, seven (32,41,45,49,50,
52,64) were of greatest design suitability and good
execution, 32 (15,20,30,31,34--40,43,46--48,51,53--56,59,
60,63,65,66,70,71,74,75,77--79) were of greatest design
suitability and fair execution, five
(14,33,44,68,76) were of moderate design suitability and fair execution, one
(42) was of least suitable design and good execution, and eight
(57,58,61,62,67,69,72,73) were of least suitable design and
fair execution. This intervention was well-suited for an experimental design, in certain cases using randomization of
classes, grades, or schools to the antiviolence program or to a control condition. The comparison population often received
no intervention rather than an alternative intervention. Study sample sizes varied widely (range: 21--39,168
students;
median: 563). Follow-up time from the conclusion of the intervention to the final assessment ranged from none
(i.e., assessment was conducted immediately after the end of the intervention) to 6 years (median: 6 months).
Characteristics of school programs differed by school level. In lower grades, programs focus on disruptive and
antisocial behavior. At higher grade levels, the focus shifts to general violence and specific forms of violence (e.g., bullying
and dating violence). The intervention strategy shifts from a cognitive affective approach designed to modify behavior
by changing the cognitive and affective mechanisms linked with such behavior to greater use of social skills training.
With increasing grade level, interventions might focus less on the teacher as the primary program implementer than on
other personnel (e.g., student peers or members of the team conducting the research study). Because this review assessed
only universal programs, the classroom was the principal setting of these programs at all grade levels. No clear trends
in frequency and duration of programs were apparent by school level.
Comparison of program characteristics and populations served at different school levels indicated
substantial heterogeneity by level and intercorrelation among characteristics. For this reason, bivariate analysis of program effects
by program characteristics might suggest incorrectly a causal association of these characteristics with effect size
differences when the associations actually are confounded by other associations. Recognizing the potential for other
program characteristics to confound apparent associations, the team provided bivariate associations of program characteristics
with effect sizes.
For all grades combined, the median effect was a 15.0% relative reduction in violent behavior among students
who received the program (interquartile interval [IQI]: -44.1%, -2.3%). The effects of school programs were identified at
all school levels, from a 7.3% relative reduction in violent behavior (i.e., an effect size of -7.3%) among middle
school students who received the program (15 study data points; IQI: -35.2%, 2.3%) to a median effect size of -32.4%
in prekindergarten and kindergarten programs (six study data points; percentiles not calculated). In elementary
school programs, the median reduction of violent behavior was 18.0% (34 study data points; IQI: -44.8%, 2.5%).
Among high school students, the median reduction in violent
behavior was 29.2% (four study data points; percentiles
not calculated) (Table 2). The team next explored associations between various program characteristics and effect size
to develop hypotheses that might explain the heterogeneity of program effects. Because of the intercorrelation of
program characteristics noted previously, this bivariate presentation should be regarded as simply reporting empirical
associations rather than the assessment of causal explanations for effect variability.
All school antiviolence program strategies (e.g., informational, cognitive/affective, and social skills building)
were associated with a reduction in violent behavior. All program foci (e.g., disruptive or antisocial behavior, bullying,
or dating violence) similarly were associated with reduced violent behavior. With the exception of programs
administered by school administrators or counselors, a reduction in violent behavior was reported in programs administered by
all personnel, including students and peers; however, certain effect sizes were based on a small number of study data points.
The team compared the effects of programs delivered in school environments defined by the presence of lower SES
or high rates of crime or both with environments that did not have these characteristics. For 14 studies,
these characteristics were not described. In environments with lower SES or high crime rates or both, effectiveness
was consistent with overall study results (15 studies; median: -29.2%; IQI: -42.5%, -6.7%). These programs appeared to
be similarly effective in settings in which lower SES or high crime rates or both were noted to be absent (24
studies; median: -21.0%; IQI: -50.0%, -5.2%). Nonreporting of class and crime characteristics in certain studies might
have occurred because these characteristics were not remarkable (i.e., in neighborhoods that have low crime and higher
SES). If results from these studies are combined with those for which crime is specified as low and/or SES as higher,
the combination is associated with a relative reduction of 11.2%
(38 studies; IQI: -44.4%, -1.4%), which is still
consistent in direction with overall study results.
Finally, the team explored the effects of universal school programs by predominant race and ethnicity of the
study school population. In schools in which the population was >50% black, the median reduction in violent behavior
was 16.8% (11 studies; IQI: -44.3%, -5.2%), compared with 20.4% in schools in which the population was >50%
white (22 studies; IQI: -40.2%, -5.0%) and 0.5% in schools in which the population was >50% Hispanic (six
studies; percentiles not calculated). Given the limited number of studies, the last estimate might not be reliable. To
determine whether the magnitude of the reduction in violent behavior diminished with longer intervals following the end of
the
intervention, the team assessed the association between
length of follow-up time and effect size (data not
presented). Longer follow-up was associated with smaller effect size.
Universal school-based programs were determined to be effective at all school levels and across different
populations. The reviewed studies assessed the effects of programs in communities characterized by the presence of lower SES or
high rates of crime or both, compared with communities characterized by the absence of both of these factors.
Other benefits of universal school-based programs have been noted, with supporting evidence for some of these
effects (15,46,49). Improvements were reported for social behavior more broadly, including reductions in drug
abuse, inappropriate sexual behavior, delinquency, and property crime. Substantial improvements in school attendance
and achievement also were reported
(54,80,81).
The majority of economic studies identified in this
review reported the costs of programs, but only one
study reported economic summary measures based on both costs and benefits. Cost estimates ranged from $15--$45
per student for the PATHS program (30,82) to <$200 per
student for the PeaceBuilders program (81). The only study
that estimated both costs and benefits (83) was based on the Seattle Social Development Project
(31). This study was rated as good according to the Community Guide's quality assessment criteria for economic studies. The average effect size
for this program, which focused on elementary schools in a high-crime urban area, was a relative decrease of 13% in
basic crime outcomes. The total benefits per project participant, including cost savings to taxpayers because of
reduced expenses for the criminal justice system and reduced personal and property losses for crime victims, were estimated to
be $14,426 in 2003 dollars. Net savings per participant amounted to $9,837. In terms of cost-benefit ratio, this
program indicated a benefit of $3.14 for every dollar
invested in the program. Although the effect size found in the study is
near the median effect size of other school programs, this program is more comprehensive, more intensive, and of
longer duration than many programs, in addition to being more costly. Thus, the cost benefit of other programs might
differ from that determined for the Seattle Social Development Project.
Schools and their curricula are subject to multiple
requirements and demands. Because schools might not
recognize the need for instruction in the reduction of violence and aggression, introducing effective programs into school
curricula and schedules might be difficult. The need for teacher training for these programs also might make acceptance
and implementation difficult. However, the benefits of many programs for traditional academic outcomes such as
attendance and school performance might enhance the
interest of school policy makers, administrators, and
teachers in these programs.
In summary, study results consistently indicated that universal school-based programs were associated
with decreased violence. Beneficial results were found across all school levels examined. On the basis of the limited amount
of available economic data, universal school-based programs also appear to be cost-effective.
Discussion
The findings of this review were compared with a
recently updated meta-analysis (84) with a similar approach
to intervention definition and outcomes assessed, although certain differences existed in the literature and methods
used. Expanded versions of both reviews, including a
detailed exploration of similarities and differences, have been
published (85). The meta-analysis indicated that the associations reported in the present review were not greatly
confounded. School-based programs for the prevention of violence are effective for all school levels, and
different intervention strategies are all effective. Programs have other effects beyond those on violent or aggressive
behavior, including reduced truancy and improvements in school achievement, "problem behavior," activity levels,
attention problems, social skills, and internalizing problems (e.g., anxiety and depression).
Although this review established the effectiveness of universal school-based programs for the prevention of violent
and aggressive behavior, important research issues remain. These include determining 1) whether the characteristics of
the programs, or perhaps of the settings in which they are implemented, differentiate those programs that are more
effective from those that are less effective; 2) whether school programs are equally effective and cost effective for high- and
low-risk children, and in high- and low-risk environments; and 3) how to address cultural and social differences in
diverse populations to improve program implementation effectiveness.
Use of the Recommendation in States and Communities
U.S. schools provide a critical opportunity for changing societal behavior because almost the entire population
is engaged in this institution for many years, starting at an early and formative period. With approximately 71
million children in primary and secondary schools in 2003 and an overall high school graduation rate of 85%
(86), this opportunity is difficult to overestimate. The potential benefits of improved school function alone are notable.
The broader and longer term benefits in terms of reduced
delinquency and antisocial behavior are yet more
substantial. Universal school-based violence prevention programs represent an important means of reducing violent
and aggressive behavior in the United States. The findings of this review suggest that universal school-based
violence prevention programs can be effective in communities with
diverse ethnic compositions and in communities
whose residents are predominantly of lower SES or that have
relatively high rates of crime.
References
Maguire K, Pastore AL. Sourcebook of criminal justice statistics 2003. Washington, DC: US Department of Justice, Bureau of Justice Statistics,
US Government Printing Office; 2005.
US Census Bureau. Monthly postcensal resident population, by single year of age, sex, race, and Hispanic origin
(1/1/2003--6/1/2003). Washington, DC: US Census Bureau; 2006.
Snyder HN, Sickmund M. Juvenile offenders and victims: 1999
national report. Washington, DC: Office of Juvenile Justice
and Delinquency Prevention; 1999.
CDC. Health, United States, 2005. Hyattsville, MD: US Department of Health and Human Services, CDC, National Center for Health
Statistics; 2005.
Wasserman G, Keenan K, Tremblay R, et al. Child delinquency bulletin series: risk and protective factors of child delinquency. Washington,
DC: US Department of Justice, Office of Juvenile Justice and Delinquency Prevention, Office of Justice Programs; 2003.
Achenbach TM, Edelbrock C. Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Burlington, VT: University of
Vermont, Department of Psychiatry; 1983.
Patterson G, Dishion T, Yoerger K. Adolescent growth in new forms of problem behavior: macro and micro peer dynamics. Prev Sci 2000; 1:3--13.
US Department of Health and Human Services. Youth violence: a report of the Surgeon General. Washington, DC: US Department of Health
and Human Services; 2001.
Loeber R, Farrington DP, Petechuk D. Child delinquency: early intervention and prevention. Washington, DC: US Office of Juvenile Justice
and Delinquency Prevention: Child Delinquency Bulletin Series; 2003.
DeVoe J, Peter K, Noonan M, Snyder T, Baum K. Indicators of school crime and safety: 2005 (NCES 2006-001/NCJ 210697). Washington
DC: US Government Printing Office; 2005.
Goleman D. Emotional intelligence. New York, NY: Bantam Books; 1994.
Glanz K, Rimer B, Lewis F, eds. Health behavior and health education: theory, research, and practice. 3rd ed. San Francisco, CA: Jossey-Bass,
Inc.; 2002.
Prothro-Stith D. Violence prevention curriculum for adolescents. Newton, MA: Education Development Center; 1987.
Flay BR, Allred C. Long-term effects of the Positive Action Program. Am J Health Behav 2003;27(Suppl 1):S6--S21.
Grossman DC, Neckerman HJ, Koepsell TD, et al. Effectiveness of a violence prevention curriculum among children in elementary school:
a randomized controlled trial. JAMA 1997;277:1605--11.
Meyer A, Farrell A, Northup W, Kung E, Plybon L. Promoting nonviolence in early adolescence: responding in peaceful and positive ways.
New York, NY: Kluwer Academic Publishers; 2000.
Kelder SH, Orpinas P, McAlister A, Frankowski R, Parcel GS, Friday J. The Students for Peace Project: a comprehensive
violence-prevention program for middle school students. Am J Prev Med 1996;12:22--30.
Bandura A. Social learning theory. Englewood Cliffs, NJ: Prentice Hall; 1977.
Embry D, Flannery DJ, Vazsonyi AT, Powell KE, Atha H. PeaceBuilders: a theoretically driven, school-based model for early violence
prevention. Am J Prev Med 1996;12(Suppl 5):91--100.
Foshee VA, Bauman KE, Greene WF, Koch GG, Linder GF, MacDougall JE. The Safe Dates Program: 1-year follow-up results. Am J Public
Health 2000;90:1619--22.
Truman BI, Smith-Akin CK, Hinman AR, et al. Developing the Guide to Community Preventive Services---overview and rationale. Am J Prev
Med 2000;18(Suppl 1):18--26.
Task Force on Community Preventive Services. The guide to community preventive services. What works to promote health? New York,
NY: Oxford University Press; 2005.
US Department of Health and Human Services. Healthy people 2010. 2nd ed. With understanding and improving health and objectives
for improving health (2 vols.). Washington, DC: US Department of Health and Human Services; 2000.
Briss PA, Zaza S, Pappaioanou M, et al. Developing an evidence-based guide to community preventive services: methods. Am J Prev
Med 2000;18(Suppl 1):35--43.
Zaza S, Wright-de Aguero L, Briss PA, et al. Data collection instrument and procedure for systematic reviews in the Guide to
Community Preventive Services. Am J Prev Med 2000;18(Suppl 1):44--74.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-IV-TR. 4th ed. Washington, DC:
American Psychiatric Association; 2000.
Hann DM, Borek N, eds. Taking stock of risk factors for child/youth externalizing behavior problems. Bethesda, MD: US Department of
Health and Human Services, Public Health Service, National Institute of Mental Health/National Institute of Health; 2001.
Carande-Kulis VG, Maciosek MV, Briss PA, et al. Methods for systematic reviews of economic evaluations for the Guide to Community
Preventive Services. Am J Prev Med 2000;18(Suppl 1):75--91.
Greenberg MT, Kusche C. Preventive intervention for school-aged deaf children: the PATHS curriculum. J Deaf Stud Deaf Educ 1998;3:49--63.
Hawkins JD, Catalano RF, Kosterman R, Abbott R, Hill KG. Preventing adolescent health-risk behaviors by strengthening protection
during childhood. Arch Pediatr Adolesc Med 1999;153:226--34.
Ialongo N, Werthamer L, Kellam SG. Proximal impact of two first-grade preventive interventions on the early risk behaviors for later
substance abuse, depression and antisocial behavior. Am J Community Psychol 1999;27:599--641.
Olweus D. Bully/victim problems in school: facts and intervention. Eur J Psychol Educ 1997;12:495--510.
Reid JB, Eddy JM, Fetrow RA, Stoolmiller M. Description and immediate impacts of a preventive intervention for conduct problems. Am
J Community Psychol 1999;27:483--517.
Shure MB, Spivack G. Interpersonal problem-solving in young children: a cognitive approach to prevention. Am J Community
Psychol 1982;10:341--55.
Aber JL, Jones SM, Brown JL, Chaudry N, Samples F. Resolving conflict creatively: evaluating the developmental effects of a school-based
violence prevention program in neighborhood and classroom context. Dev Psychopathol 1998;10:187--213.
Alsaker FD, Valkanover S. Early diagnosis and prevention of victimization in kindergarten. In: Juvonen J, Graham S, eds. Peer harassment in
school: the plight of the vulnerable and victimized. New York, NY: The Guilford Press; 2001:175--95.
Battistich V, Schaps E, Watson M, Solomon D, Lewis C. Effects of the Child Development Project on students' drug use and other
problem behaviors. J Prim Prev 2000;21:75--99.
Bosworth K, Espelage D, DuBay T, Daytner G, Karageorge K. Preliminary evaluation of a multimedia violence prevention program for
adolescents. Am J Health Behav 2000;24:268--80.
Boulton MJ, Flemington I. The effects of a short video intervention on secondary school pupils' involvement in definitions of and attitudes
towards bullying. Sch Psychol Int 1996;17:331--45.
Conduct Problems Prevention Research Group. Evaluation of the first 3 years of the Fast Track prevention trial with children at high risk
for adolescent conduct problems. J Abnormal Child Psychol 2002;30:19--35.
DuRant RH. Comparison of two violence prevention curricula for middle school adolescents. J Adolesc Health 1996;19:111--7.
DuRant RH, Barkin S, Krowchuck DP. Evaluation of a peaceful conflict resolution and violence prevention curriculum for sixth-grade students.
J Adoles Health 2001;28:386--93.
Elias MJ, Gara MA, Schuyler T, Branden-Muller LR, Sayette MA. The promotion of social competence: longitudinal study of a preventive
school-based program. Am J Orthopsychiatry 1991;61:409--17.
Esbensen FA, Osgood DW, Taylor TJ, Peterson D, Freng A. How great is G. R. E. A. T.? Results from a longitudinal quasi-experimental
design. Criminol Public Policy 2001;1:87--118.
Farrell AD, Meyer AL. The effectiveness of a school-based curriculum for reducing violence among urban sixth-grade students. Am J Public
Health 1997;87:979--84.
Farrell AD, Meyer AL, White KS. Evaluation of Responding in Peaceful and Positive Ways (RIPP): a school-based prevention program for
reducing violence among urban adolescents. J Clin Child Psychol 2001;30:451--63.
Farrell AD, Valois RF, Meyer AL. Evaluation of the RIPP-6 violence prevention program at a rural middle school. Am J Health Ed
2002;33:167--72.
Farrell AD, Valois RF, Meyer AL, Tidwell RP. Impact of the RIPP violence prevention program on rural middle school students. J Prim
Prev 2003;24:143--67.
Flay BR, Graumlich S, Segawa E, Burns JL, Holliday MY. Effects of 2 prevention programs on high-risk behaviors among African-American youth:
a randomized trial. Arch Pediatr Adolesc Med 2004;158: 377--84.
Sandy SV, Boardman SK. The Peaceful Kids Conflict Resolution Program. Int J Conflict Manag 2000;11:337--57.
Sawyer MG, MacMullin C, Graetz B, Said JA, Clark JJ, Baghurst P. Social skills training for primary school children: a one-year follow-up study.
J Paediatr Child Health 1997;33:378--83.
Flannery DJ, Liau AK, Powell KE, et al. Initial behavior outcomes for the PeaceBuilders universal school-based violence prevention program.
Dev Psychol 2003;39:292--308.
Flay BR, Allred CG, Ordway N. Effects of the Positive Action Program on achievement and discipline: two matched-control comparisons. Prev
Sci 2001;2:71--89.
Gesten EL, Rains MH, Rapkin BD, et al. Training children in social problem-solving competencies: a first and second look. Am J
Community Psychol 1982;10:95--115.
Hindley P, Reed H. Promoting alternative thinking strategies (PATHS): mental health promotion with deaf children in school. In: Decker S,
Kirby S, Greenwood A, et al., eds. Taking children seriously: applications of counseling and therapy in education. London, UK: Cassell
Publishers; 1999:113--30.
Johnson DW, Johnson RT, Dudley BS. Effects of peer mediation training on elementary school students. Mediation Q 1992;10:89--99.
Johnson DW, Johnson RT, Dudley BS, Ward M, et al. The impact of peer mediation training on the management of school and home
conflicts. Am Educ Res J 1995;32:829--44.
Kenney DJ, Watson TS. Reducing fear in the schools: managing
conflict through student problem solving. Educ Urban Soc 1996;28:436--55.
Lynch KB, Geller SR, Schmidt MG. Multi-year evaluation of the effectiveness of a resilience-based prevention program for young children. J
Prim Prev 2004;24:335--53.
McMahon SD, Washburn JJ. Violence prevention: an evaluation of program effects with urban African-American students. J Prim Prev
2003;24:43--62.
McMahon SD, Washburn J, Felix ED, Yakin J, Childrey G. Violence prevention: program effects on urban preschool and kindergarten
children. Appl Prev Psychol 2000;9:271--81.
Nelson G, Carson P. Evaluation of a social problem-solving skills program for third- and fourth-grade students. Am J Community Psychol 1988;16:79--99.
O'Donnell L, Stueve A, Doval AS, et al. Violence prevention and young adolescents' participation in community youth service. J Adolesc
Health 1999;24:28--37.
Orpinas P, Parcel GS, McAlister A, Frankowski R. Violence prevention in middle schools: a pilot evaluation. J Adolesc Health 1995;17:360--71.
Orpinas P, Kelder S, Frankowski R, Murray N, Zhang Q, McAlister A. Outcome evaluation of a multi-component violence-prevention program
for middle schools: the Students for Peace project. Health Educ Res 2000;15:45--58.
Orpinas P, Horne A. School bullying: changing the problem by changing the school. Sch Psychol Rev 2003;32:431--44.
Pepler DJ, Craig WM, Ziegler S, Charach A. An evaluation of an anti-bullying intervention in Toronto schools. Can J Commun Ment
Health 1994;13:95--110.
Palumbo DJ, Ferguson JL. Evaluating Gang Resistance Education and Training (GREAT): is the impact the same at that of Drug Abuse
Resistance Education (DARE)? Eval Rev 1995;19:597--619.
Renfro J, Huebner R, Ritchey B. School violence prevention: the effects of a university and high school partnership. J Sch Violence 2003;2:81--99.
Rickel AU, Eshelman AK, Loigman GA. Social problem solving training: a follow-up study of cognitive and behavioral effects. J Abnorm
Child Psychol 1983;11:15--28.
Roland E. Bullying: a developing tradition of research and management. In: Tattum D, ed. Understanding and managing bullying.
Oxford, UK: Heinemann Education; 1993:15--30.
Roush G, Hall E. Teaching peaceful conflict resolution. Mediation Q 1993;11:185--91.
Shapiro J, Burgoon JD, Welker CJ, Clough JB. Evaluation of The Peacemakers Program: school-based violence prevention for students in
grades four through eight. Psychol Sch 2002;39:87--100.
Stevens V, De Bourdeaudhuij I, Van Oost P. Bullying in Flemish schools: an evaluation of anti-bullying intervention in primary and
secondary schools. Brit J Educ Psychol 2000;70:195--210.
Taylor CA, Liang B, Tracy AJ, Williams LM, Seigle P. Gender differences in middle school adjustment, physical fighting, and social skills:
evaluation of a social competency program. J Prim Prev 2002;23: 261--73.
Weissberg RP, Gesten EL, Carnrike CL, et al. Social problem-solving skills training: a competence building intervention with 2nd--4th
grade children. Am J Community Psychol 1981;9:411--24.
Whitney I, Rivers I, Smith P, et al. The Sheffield project: methodology and findings. In: Smith P, Sharp S, eds. School bullying: insights
and perspectives. London, UK: Routledge; 1994:20--56.
Winer JI, Hilpert PL, Gesten EL, Cowen EL, Schubin WE. The evaluation of a kindergarten social problem solving program. J Prim
Prev 1982;2:205--16.
Conduct Problems Prevention Research Group. Initial impact of the fast track prevention trial for conduct problems: II. Classroom effects.
J Consult Clin Psychol 1999;67:648--57.
Vazsonyi A, Belliston L, Flannery D. Evaluation of a school-based, universal violence prevention program: low-, medium-, and high-risk
children. Youth Violence and Juvenile Justice 2004;2:185--206.
Greenberg MT, Kusche C, Mihalic SF. Blueprints for violence prevention, Book Ten: Promoting Alternative Thinking Strategies (PATHS).
Boulder, CO: Center for the Study and Prevention of Violence; 1998.
Aos S, Lieb R, Mayfield J, et al. Benefits and costs of prevention and early intervention programs for youth. Olympia, WA: Washington
State Institute for Public Policy; 2004. Available at
http://www.wsipp.wa.gov/rptfiles/04-07-3901.pdf.
Wilson S, Lipsey M. Update of a meta-analysis of school-based intervention programs. Am J Prev Med. 2007;33(Suppl):S130--S143.
Hahn R, Fuqua-Whitley D, Wethington H, et al. and the Task Force on Community Preventive Services. Effectiveness of universal
school-based programs to prevent violent and aggressive behavior: a systematic review. Am J Prev Med 2007;33(Suppl):S114--S129.
US Census Bureau. Statistical abstract of the United States.
Washington, DC: US Census Bureau; 2001.
* Points of view expressed are those of the contributors and the Task Force on Community Preventive Services and do not necessarily reflect those of CDC,
the National Institutes of Health, the National Institute of Justice, the U.S. Department of Justice, or the U.S. Department of Health and Human Services.
Author affiliations reflect author's location while this research was being conducted.
§ High-income economiesas defined by the World Bank are Andorra, Antigua & Barbuda, Aruba, Australia, Austria, The Bahamas, Bahrain, Barbados,
Belgium, Bermuda, Brunei, Canada, Cayman Islands, Channel Islands, Cyprus, Denmark, Faeroe Islands, Finland, France, French Polynesia, Germany,
Greece, Greenland, Guam, Hong Kong (China), Iceland, Ireland, Isle of Man, Israel, Italy, Japan, Republic of Korea, Kuwait, Liechtenstein, Luxembourg,
Macao (China), Malta, Monaco, Netherlands, Netherlands Antilles, New Caledonia, New Zealand, Norway, Portugal, Puerto Rico, Qatar, San Marino,
Singapore, Slovenia, Spain, Sweden, Switzerland, Taiwan (China), United Arab Emirates, United Kingdom, United States, and U.S. Virgin Islands.
Task Force on Community Preventive Services*
June 1, 2007
Chair: Jonathan E. Fielding, MD, Los Angeles County Department of Health Services, Los Angeles, California.
Vice-chair: Barbara K. Rimer, DrPH; School of Public Health, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina.
Members: Ana Abraido-Lanza, PhD, Mailman School of Public Health, Columbia University, New York, New York; Ned Calonge, MD,
Colorado Department of Public Health and University of Colorado Health Sciences Center, Denver, Colorado; John Clymer, Partnership for
Prevention, Washington, District of Columbia; Kay Dickersin, PhD, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland;
Karen Glanz, PhD, Rollins School of Public Health, Emory University, Atlanta, Georgia; Ron Goetzel, PhD, Cornell University Institute for Health
and Productivity Studies, Thomson Medstat, Washington, District of Columbia; Robert L. Johnson, MD, New Jersey Medical School, University
of Medicine and Dentistry of New Jersey, Newark, New Jersey; Nicolaas P. Pronk, PhD, HealthPartners Research Foundation, Minneapolis,
Minnesota; Gilbert Ramirez, DrPH, Charles R. Drew University, Los Angeles, California; Dennis L. Richling, MD, Matria Healthcare, Chicago, Illinois;
and Steven M. Teutsch, MD, Merck & Company, Inc., West Point, Pennsylvania.
Consultants: Robert S. Lawrence, MD, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, Maryland; J. Michael
McGinnis, MD, Institute of Medicine of the National Academies, Washington, District of Columbia.
* The following persons also served on the Task Force while the recommendations were being developed: Mindy Thompson Fullilove, MD, New York State
Psychiatric Institute and Columbia University, New York, New York; Alan R. Hinman, MD, Task Force for Child Survival and Development, Atlanta, Georgia; George J.
Isham, MD, HealthPartners, Minneapolis, Minnesota; Garland H. Land, MPH, Center for Health Information Management and Epidemiology, Missouri Department
of Health, Jefferson City, Missouri; Patricia Dolan Mullen, DrPH, University of Texas--Houston School of Public Health, Houston, Texas; Patricia A. Nolan,
MD, Rhode Island Department of Health, Providence, Rhode Island; and Alonzo L. Plough, PhD, Public Health-Seattle and King County, Seattle, Washington. Lloyd
F. Novick, MD, East Carolina University, Greenville, North Carolina, also was a consultant to the Task Force during that time.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.