Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
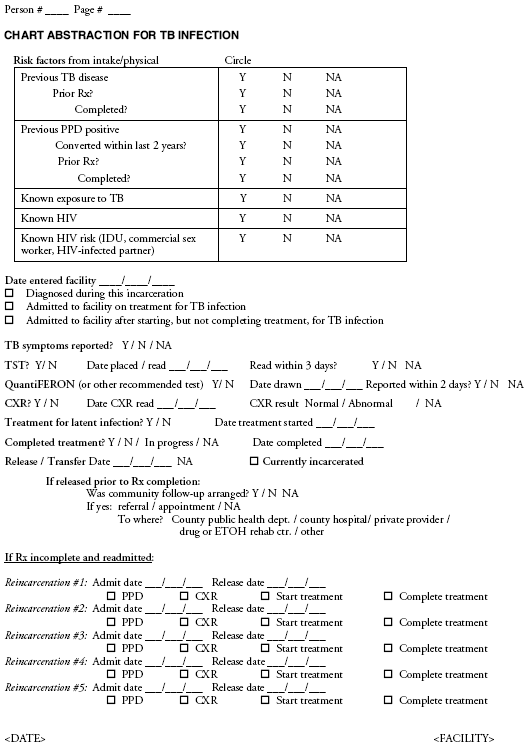
Appendix B
Examples of Data Collection Tools
Glossary
Acid-fast bacilli (AFB). A laboratory test that involves microscopic examination of a stained smear (typically of sputum)
to determine if mycobacteria are present. A presumptive diagnosis of pulmonary tuberculosis (TB) can be made with a
positive AFB sputum smear result; however, approximately 50% of the patients with pulmonary TB disease have negative
AFB sputum-smear results. The diagnosis of TB disease typically is not confirmed until
Mycobacterium tuberculosis is identified in culture. A positive nucleic acid amplification (NAA) test is useful as a confirmatory test.
Aerosol. Dispersions of particles in a gaseous medium (e.g., air). Droplet nuclei are examples of particles that are
expelled by a person with an infectious disease (e.g., by coughing, sneezing, or singing). For
M. tuberculosis, the droplet nuclei are approximately 1--5
µm. Because of their small size, the droplet nuclei can remain suspended in the air for substantial
periods and can transmit M. tuberculosis to other persons.
Adherence. Following instructions regarding a treatment regimen (adherence to treatment).
Administrative controls. Managerial measures that reduce the risk for exposure to persons who might have TB
disease. Examples include coordinating efforts with the state or local health department, conducting a TB risk assessment of
the setting, developing and instituting a written TB infection-control plan to ensure prompt detection, airborne
infection isolation, treating persons with suspected or confirmed TB disease, and screening and evaluating persons who are at risk
for TB disease or who might be exposed to M.
tuberculosis.
Air change rate. Ratio of the airflow in volume units per hour to the volume of the space under consideration in
identical volume units, typically expressed in air changes per hour (ACH).
Air change rate (equivalent). Ratio of the volumetric air loss rate associated with an environmental control or
combination of controls (e.g., an air cleaner or ultraviolet germicidal irradiation [UVGI] system) divided by the volume of the room
in which the control has been applied. The equivalent air change rate is useful for describing the rate at which bioaerosols
are removed by means other than ventilation.
Air change rate (mechanical). Ratio of the airflow to the space volume per unit time, typically expressed in ACH.
Air changes per hour (ACH). Air change rate expressed as the number of air exchange units per hour.
Airborne infection isolation room (AII room). Formerly called a negative pressure isolation room, an AII room is a
single-occupancy patient-care room used to isolate persons with suspected or confirmed infectious TB disease. Environmental
factors are controlled in AII rooms to minimize the transmission of infectious agents that typically are spread from person to
person by droplet nuclei associated with coughing or aerosolization of contaminated fluids. An AII room should have these all
three of these characteristics: 1) negative pressure, so air flows under the door gap into the room; 2) an air flow rate of 6--12
ACH; and 3) direct exhaust of air from the room to the outside of the building or recirculation of air through a high
efficiency particulate air (HEPA) filter.
Anergy. Condition in which a person has a diminished ability to react to antigens because of a medical condition
or situation resulting in immunosuppression. Persons who have such immunosuppression are considered to be
anergic. Traditionally, anergy is identified through a tuberculin skin test (TST). Anergy skin testing has poor predictive value and
is not routinely recommended.
Apical. Relating to or located at the tip (an apex).
Asymptomatic. Neither causing nor exhibiting signs or symptoms of disease.
Bacille Calmette-Guérin (BCG). An attenuated strain of
Mycobacterium bovis that is used in multiple countries
worldwide as a TB vaccine, named after the French scientists Calmette and Guérin. BCG has limited efficacy in preventing disease and
is rarely used in the United States. The vaccine is effective in preventing disseminated and meningeal TB disease in infants
and young children and is appropriately used in multiple countries in which TB disease is endemic.
Boosting. A phenomenon in which some persons who receive a TST many years after acquiring latent TB infection
(LTBI) have a negative result to an initial TST followed by a positive result to a subsequent TST. The second (i.e., positive) result
is caused by a boosted immune response of the prior sensitivity rather than by a new infection. Two-step testing is used
to distinguish new infections from boosted reactions in TB infection control screening programs that utilize TST for
detecting M. tuberculosis (see Two-step skin testing). Because
QuantiFERON®-TB Gold (QFT-G) test is an in vitro method, it is
not complicated by boosting.
Bronchoscopy. Procedure for examining the respiratory tract that requires inserting an instrument (bronchoscope),
either flexible or rigid, through the mouth or nose and into the respiratory tree. Bronchoscopy can be used to obtain
diagnostic specimens and creates a risk for transmission for exposed health-care professionals when performed on a patient
with pulmonary or laryngeal TB disease.
Cavity. The radiographic appearance of a hole in the lung parenchyma, typically not involving the pleural space,
resulting from the destruction of pulmonary tissue by an interaction of
M. tuberculosis infection and the host response seen in
TB disease (or other pulmonary infections). TB patients with cavitary disease indicated by a chest radiograph typically are
more infectious than TB patients without cavitary disease.
Chest x-ray. See Radiography.
Close contact. A person who has shared the same air space in a household or other enclosed environment for a
prolonged period (i.e., days or weeks, not minutes or hours) with a person with suspected or confirmed TB disease.
Contact. A person who has shared the same air space with a person in whom infectious TB disease has been
diagnosed. Although sputum-smear results, the grade of the sputum-smear result if positive, and sputum culture results all influence
the likelihood of infectiousness, other factors (e.g., exposure time, environmental conditions, and site of disease) also contribute
to infectiousness.
Contact investigation. The process of finding, notifying, screening, and treating persons who might have LTBI or
TB disease as a result of recent contact with a person diagnosed with TB disease. This process is undertaken promptly after a
TB source patient is identified.
Contagious. Refers to a disease that can be transmitted from one living being to another through direct contact
(e.g., measles) or indirect contact (e.g., TB or cholera). The agent responsible for the contagious character of a disease is described
as being infectious; the most common infectious agents are microorganisms (e.g.,
M. tuberculosis) or macroorganisms (e.g., parasitic worms).
Conversion. See TST conversion.
Conversion rate. The percentage of a population with a converted test result (TST or QFT-G) for
M. tuberculosis within a specified time. This is calculated by dividing the number of conversions among eligible persons in the setting in a
specified period (numerator) by the number of persons who received tests in the setting over the same period (denominator),
multiplied by 100.
Culture. Microorganisms obtained from sputum or samples of other body fluids that are grown in the laboratory to
detect and identify infection. This test typically takes 2--4 days when used to detect the majority of bacteria, although cultures
for mycobacteria typically must grow for 2--4 weeks.
Directly observed therapy (DOT). Adherence-enhancing strategy in which a trained health-care professional or
other specially trained person watches a patient swallow each dose of medication and records the dates that the medication
was taken. DOT is the standard of care for all patients with TB disease and should be used for all doses during the course
of treatment for TB disease and for LTBI whenever feasible. All patients on intermittent (i.e., once- or twice-weekly)
treatment for TB disease or LTBI should receive DOT. Plans for DOT should be coordinated with the state or local health
department. Rates of relapse and development of drug-resistance are decreased when DOT is used.
Disposable respirator. A respirator designed to be used and then discarded; also known as a filtering-facepiece
respirator. Respirators should be discarded after excessive resistance, physical damage, or hygiene considerations.
Droplet nuclei. Microscopic particles produced when a person coughs, sneezes, shouts, or sings. These particles can
remain suspended in the air for prolonged periods of time and can be carried on normal air currents throughout the room and
to adjacent spaces or areas receiving exhaust air.
Drug-susceptibility test. Laboratory test that determines whether the
M. tuberculosis bacteria cultured from a
patient's isolate are susceptible or resistant to various first-line or second-line anti-TB drugs.
Enabler. An item or service that helps to remove barriers for willing (but unable) patients to adhere to anti-TB therapy
(e.g., transportation, bus tokens, stable housing, driver's license, and service programs).
Environmental control measures. Physical or mechanical measures (as opposed to administrative control measures) used
to reduce the risk for transmission of M.
tuberculosis. Examples include ventilation, filtration, ultraviolet lamps,
airborne infection isolation rooms, and local exhaust ventilation devices.
Epidemiologic cluster. A series of cases that can be closely grouped by time or place.
Erythema. Abnormal redness of the skin. Erythema might develop around a TST site, but it should not be read as part
of the TST result.
Exposure. The condition of being subjected to something (e.g., an infectious agent) that could have a harmful
effect. A person exposed to M. tuberculosis does not necessarily become infected (See Transmission).
Exposure period. The period when the following two events overlap: 1) the time the contact shares the same air space
with the TB source patient and 2) the infectious period of the source patient.
Extrapulmonary TB. Disease in any part of the body other than the lungs (e.g., the kidneys, spine, or lymph nodes.)
The presence of extrapulmonary disease does not exclude pulmonary TB disease.
False-positive TST or QFT-G result. A TST or QFT-G result that is interpreted as positive for a particular purpose
(i.e., infection control surveillance or medical and diagnostic evaluation) in a person who is not actually infected
with M. tuberculosis. For the TST, this is more likely to occur in persons who have been vaccinated with BCG or who are
infected with nontuberculous mycobacteria (NTM).
Heating, ventilation, air conditioning
(HVAC). Mechanical systems that provide (either collectively or
individually) heating, ventilating, or air conditioning for comfort within or associated with a building.
High-efficiency particulate air (HEPA) filter. A filter that is certified to remove >99.97% of particles 0.3
µm in size, including M.
tuberculosis--containing droplet nuclei; the filter can be either portable or stationary. Use of HEPA filters
in building ventilation systems requires expertise in installation and maintenance.
Hemoptysis. The expectoration or coughing up of blood or blood-tinged sputum. Hemoptysis is one of the symptoms
of pulmonary TB disease, and it can also occur in other pulmonary conditions (e.g., lung cancer).
Immunosuppression and immunocompromising
conditions. A condition in which the immune system is
not functioning normally. The term "immunocompromised" has come to be defined as the broader term, and the
term "immunosuppression" is now used when referring to states that were induced by medical treatment or procedures
(i.e., iatrogenic), including causes that result from therapy for another condition. Immunocompromised persons are at
increased risk for rapidly progressing to TB disease after infection with
M. tuberculosis. Immunocompromising conditions also make
TB disease more difficult to diagnose, increasing the likelihood of a false-negative result for a test for
M. tuberculosis (e.g., TST and QFT-G).
Incentive. An item or service that rewards desired behavior (e.g., adherence to anti-TB therapy). Examples of
incentives include cookies, food, food vouchers, clothing vouchers, and stickers. Incentives motivate patients to take medication
and keep clinic appointments, and they should be specifically tailored to each patient.
Induration. Area of firmness produced by an immune cell infiltration in response to an injected antigen. In tuberculin
skin testing (TST) or anergy testing, the diameter of the indurated area is measured 48--72 hours after the injection in a
direction perpendicular to the long axis of the forearm and the result recorded in mm. The induration of the TST result should
be measured, and not erythema (abnormal redness of the skin).
Infectious. See Contagious.
Infectious droplet nuclei. Droplet nuclei produced by an infectious TB patient that can carry tubercle bacilli and
be inhaled by others. Although these nuclei typically are produced from patients with pulmonary TB through coughing, they
can also be generated from aerosolizing procedures (e.g., during bronchoscopy, autopsy, or wound irrigation) performed at the
site of infectious tissue.
Infectious period. The time during which a person with TB disease might have transmitted
M. tuberculosis organisms to others. The infectious period typically is defined as 12 weeks before TB diagnosis or onset of cough (whichever is longer). If
a patient has no TB symptoms, is AFB-smear negative, and has a non-cavitary chest radiograph, the presumed infectious
period can be reduced to 4 weeks before the date of diagnosis of suspected TB. If the contact investigation indicates that
TB transmission occurred throughout the identified infectious period, the time for contact investigation might need to
be expanded beyond the basic 12 weeks.
Isolation. Separation of a person or group of persons from others to prevent the spread of droplet nuclei. In this report,
the term "airborne infection isolation" is used interchangeably with "isolation."
Isoniazid (INH). A drug used to prevent TB disease in persons who have latent TB infection (LTBI). INH is also one of
the four drugs often used to treat TB disease.
Latent TB infection (LTBI). Infection with M.
tuberculosis in which the bacilli are alive but inactive in the body.
Persons who have LTBI but who do not have TB disease are asymptomatic, do not feel sick, and cannot spread TB to other
persons. They typically have a positive TST or QFT-G result. Approximately 5%--10% of infected persons will develop TB disease
at some point in their lives, but the risk is considerably higher for persons who are immunocompromised, especially
persons infected with HIV. Persons with LTBI can be given treatment to prevent the infection from progressing to disease.
Mantoux method. The recommended TST method, performed by injecting 0.1 ml containing 5 tuberculin units (TU)
of purified protein derivative (PPD) intradermally into the volar or dorsal surface of the forearm. The injection is made using
a 1/4--1/2-inch, 27 gauge needle and a tuberculin (preferable a safety-type) syringe.
Medical evaluation. An examination conducted for the purpose of diagnosing TB disease or LTBI, selecting treatment,
and assessing response to therapy. A medical evaluation might include the following components:
medical history and TB symptom screening,
clinical or physical examination,
screening and diagnostic tests (e.g., TSTs, chest radiographs, bacteriologic examination, and HIV testing),
counseling, and
treatment referrals.
Multidrug-resistant tuberculosis (MDR TB). TB disease caused by
M. tuberculosis organisms that are resistant to at
least isoniazid and rifampin.
Mycobacterium tuberculosis. The bacterium that causes LTBI and TB disease.
Mycobacterium tuberculosis culture. A laboratory test to determine the presence of
M. tuberculosis. In the absence of cross-contamination, a positive culture confirms the diagnosis of TB disease.
N95 disposable respirator. Air-purifying, filtering facepiece respirators certified by the National Institute for
Occupational Safety and Health with filters
>95% efficient at removing 0.3 micron particles; these respirators are not resistant to oil
(see Respirator).
Negative pressure. The difference in air pressure between two areas in a health-care setting. A room that is under
negative pressure has a lower pressure than adjacent areas, which keeps air from flowing out of the room and into adjacent rooms
or areas.
Nontuberculous mycobacteria (NTM). Refers to mycobacterium species other than those included as part of
M. tuberculosis complex. Although valid from a laboratory perspective, the term can be misleading because certain types of
NTM cause disease with pathological and clinical manifestations similar to TB disease. Another term used interchangeably
with NTM is "mycobacteria other than tuberculosis" (MOTT).
Nucleic acid amplification (NAA) test. Laboratory test used to target and amplify a single DNA or RNA sequence
for identification. This technique is highly sensitive and specific for identification of
M. tuberculosis, and results from these
tests typically are available within 1--3 days.
Outbreak (TB). The result when transmission of
M. tuberculosis continues to occur (i.e., potentially ongoing or
newly recognized transmission).
Periodic fit testing. Repetition of fit testing performed in accordance with federal, state, and local regulations.
Additional fit testing should be used when 1) a new model of respirator is used, 2) a physical characteristic of the user changes, or
3) when the user or respiratory program administrator is uncertain that the staff member is obtaining an adequate fit.
Pulmonary TB. TB disease that occurs in the lung parenchyma. The majority of TB disease is pulmonary.
Purified protein derivative (PPD) tuberculin. A material used in diagnostic tests for infection with
M. tuberculosis. PPD is a purified tuberculin preparation that was developed in the 1930s and derived from old tuberculin. In the United States, it
is administered as part of a TST that is given as an intradermal injection of 0.1 ml containing 5 TU (Mantoux method) and
read 48--72 hours later. It also was used in the older version of QFT-G (see Tuberculin skin test).
QuantiFERON®-TB Gold test
(QFT-G). An in vitro cytokine assay that assesses the cell-mediated immune response
to specific antigens of M. tuberculosis (ESAT6 and CFP-10) in whole blood used to determine
M. tuberculosis infection. Unlike the TST, the QFT-G requires only a single visit. The QFT-G is more specific than the TST and is less affected by
previous BCG vaccination and infection with nontuberculous mycobacteria (NTM).
QFT-G converter. A change from a negative to a positive QFT-G result.
Radiography. Method of viewing internal body structures by using radiation to project an image onto a film,
computer screen, or paper. A chest radiograph is taken to view the respiratory system of a person who is being evaluated for
pulmonary TB disease. Abnormalities (e.g., infiltrates or cavities in the lungs and enlarged lymph nodes) described on a chest
radiography can indicate the presence of TB disease.
Recirculation. Ventilation in which all or most of the air exhausted from an area is returned to the same area or other
areas of the setting.
Reinfection. A second infection that follows recovery from a previous infection by the same causative agent. Often
used when referring to an episode of TB disease resulting from a subsequent infection with
M. tuberculosis.
Resistance. Ability of certain strains of mycobacteria, including
M. tuberculosis, to grow and multiply in the presence
of certain drugs that ordinarily kill them. Such strains are referred to as drug-resistant strains and contribute to drug-resistant
TB disease (see Multidrug-resistant TB.)
Respirator. A device worn to prevent the wearer from inhaling airborne contaminants.
Respiratory protection. The third level in the hierarchy of TB infection-control measures (after administrative
and environmental controls).
Risk factor. Any condition or circumstance (i.e., causal agents) that is associated (without confounding or bias) with
an increase in the frequency of disease.
Screening. Measures used to identify persons who have TB disease or LTBI (see Symptom screen).
Secondary cases. Cases of TB disease caused by transmission from the source patient.
Smear (AFB smear). Laboratory technique for visualizing mycobacteria. The specimen (direct or concentrated) is
spread onto a laboratory slide, stained, and examined using a microscope. Smear results typically are available within
24 hours of specimen collection. The concentration of organisms per unit area of slide (the smear grade) correlates with the degree
of infectiousness. However, a positive AFB smear result is not diagnostic of TB disease because organisms other than
M. tuberculosis (e.g., nontuberculous mycobacteria [NTM]) might be seen on an AFB smear result (see
Nontuberculous mycobacteria and Acid-fast bacilli).
Source control. Manipulation of a process preventing an emission (e.g., aerosolized
M. tuberculosis) at the place of origin. Examples of source control methods include booths in which a patient coughs and produces sputum, biological safety
cabinets in laboratories, and local exhaust ventilation.
Source patient (TB). The patient who was the original source of infection for secondary cases or contacts.
Specimen. Any body fluid, secretion, or tissue sent to a laboratory in which diagnostic tests, smears, and cultures for
M. tuberculosis are performed.
Sputum. Mucus secretions coughed up from deep within the lungs (to be distinguished from saliva and nasal secretions).
If a patient has pulmonary disease, an examination of the sputum by smear and culture can be helpful in evaluating
the organism responsible for certain infectious diseases (e.g., TB). Sputum is different than and should not be confused with
saliva or nasal secretions.
Sputum induction. Method used to obtain sputum from a patient who is unable to cough up a specimen
spontaneously. The patient inhales a saline mist, which stimulates coughing from deep within the lungs.
Susceptibility. See Drug-susceptibility test.
Suspect TB patient. A person in whom a diagnosis of TB disease is being considered, regardless of whether anti-TB
therapy has been started. Persons should not remain in this category for >3 months. A patient might be determined as suspect if one
or more of the following criteria are satisfied:
coughing for >3 weeks and one or more additional signs or symptoms of TB disease (e.g., loss of appetite,
unexplained weight loss, night sweats, bloody sputum or
hemoptysis, hoarseness, fever, fatigue, and chest pain),
a positive TST result and signs or symptoms of infection in the lung, pleura, or airways,
positive AFB sputum smear result, or
Pending results from sputum culture or NAA test for M. tuberculosis.
Symptomatic. Exhibiting signs or symptoms of a particular disease or disorder. Symptoms of pulmonary TB disease
(or infection in the lung, pleura, or airways [including the larynx]) include coughing for
>3 weeks, loss of appetite, unexplained weight loss, night sweats, bloody sputum or hemoptysis, hoarseness, fever, fatigue, or chest pain.
Symptom screen. A procedure used during a clinical evaluation in which the patient is asked if they have experienced
any signs or symptoms of TB disease.
TB case. A particular episode of clinical TB disease. This term refers only to the disease, not to the person with the
disease. By law, TB cases and suspect TB cases must be reported to the state or local health department.
TB contact. A person who has shared the same air space with a person who has TB disease for a sufficient amount of
time to allow possible transmission of M.
tuberculosis.
TB disease. TB disease is caused by Mycobacterium
tuberculosis. The bacteria can attack any part of the body, but
they typically attack the lungs. TB disease is diagnosed by isolation of
M. tuberculosis in a culture. TB disease of the lungs or
larynx can be transmitted when a person with the disease coughs, sings, laughs, speaks, or breathes. TB disease might be infectious.
TB infection. TB infection is the term used for persons with positive TST or QFT-G results, negative bacteriologic
studies (if conducted), and no clinical, bacteriologic, or radiographic evidence of TB disease. A better term is infection with
M. tuberculosis. In the majority of persons who inhale TB bacteria and become infected, the body is able to fight the bacteria
to stop them from growing. The bacteria become inactive, but they remain alive in the body and can become active later.
TB infection is not contagious; patients with TB infection can not spread TB to other persons.
TB infection control program. Early detection, isolation, and treatment of persons with infectious TB through a
hierarchy of control measures, including 1) administrative controls to reduce the risk for exposure to persons with infectious TB
disease; 2) environmental controls to prevent the spread and reduce the concentration of infectious droplet nuclei in the air; and
3) respiratory protection in areas where the risk for exposure to
M. tuberculosis is high (e.g., in airborne infection
isolation rooms). A TB infection-control plan should include surveillance of inmates and correctional staff.
TB screening. Screening conducted for administrative infection control purposes. Initial TB screening can be
conducted through use of TSTs, QFT-Gs, and symptom screening, and follow up tests can be conducted using various other
testing methods (e.g., chest radiograph or sputum examination for AFB and culture) (see Symptom screen).
TB risk assessment. An initial and ongoing evaluation of the risk for transmission of
M. tuberculosis in a particular correctional facility. A risk assessment considers certain factors, including the number of inmates with TB housed during
the preceding year and the number of inmates housed who come from groups that are at risk for TB (e.g., HIV-infected
persons and recent immigrants from high-incidence countries). The TB risk assessment determines the types of screening
and infection-control measures indicated for the correctional facility.
TB skin test. See Tuberculin skin test.
Transmission. Spread of an infectious agent from one person to another. The likelihood of transmission of
M. tuberculosis is directly related to the duration and intensity of exposure (see Exposure).
Treatment for LTBI. Treatment for persons with LTBI that prevents development of TB disease.
TST. See Tuberculin skin test.
TST conversion. In programs using the TST method of screening, a change from a negative test result to a positive
test result. The size of the change in mm induration needed to be considered a conversion varies based on the baseline
testing results and whether the inmate or employee has a known exposure to a TB patient. In programs using QFT-G, a change
from negative to positive result is considered a QFT-G conversion. A conversion (TST or QFT-G) typically is interpreted
as presumptive evidence of new M.
tuberculosis infection and poses an increased risk for progression to TB disease.
TST conversion rate. The percentage of a population in which TST results converted within a specified time. This rate
is calculated by dividing the number of TST conversions among persons in the setting in a specified period (numerator) by
the number of persons who received TSTs in the setting over the same period (denominator), multiplied by 100.
Tuberculin. A sterile liquid containing proteins extracted from cultures of tubercle bacilli and used in tests for tuberculosis.
Tuberculin skin test (TST). Method used to assess the likelihood that a person is infected with
M. tuberculosis. A small dose of PPD-tuberculin is injected just beneath the surface of the skin by the Mantoux method, and the area is examined
48--72 hours after the injection. The indurated margins should be read transverse (i.e., perpendicular) to the long axis of the forearm.
Tuberculosis (TB). Clinically active disease caused by an organism in the
M. tuberculosis complex (typically M.
tuberculosis, but also including M.
bovis, M. africanum, and others).
Two-step skin testing. Procedure used for the baseline skin testing of persons who will routinely receive TSTs to reduce
the likelihood of mistaking a boosted reaction for a new infection. If an initial TST result is classified as negative, the second
step of a two-step TST should be administered 1--3 weeks after the first TST was administered. If the second TST result is
positive, it likely represents a boosted reaction, indicating that infection most likely occurred in the past. If the second TST result is
also negative, the person is classified as not infected.
Ultraviolet germicidal irradiation (UVGI). Use of ultraviolet radiation to kill or inactivate microorganisms.
CDC Advisory Council for the Elimination of Tuberculosis (ACET) Ad Hoc Working Group
Membership List
Michael E. Kimerling, MD, University of Alabama at Birmingham, Birmingham, Alabama; Cheryl McRill, MD, Arizona Tuberculosis
Control Program, Phoenix, Arizona; Joe Goldenson, MD, Jail Health Services, San Francisco Department of Public Health, L. Masae Kawamura, MD,
San Francisco Department of Health, John Lewis, MPA, Francis J. Curry National Tuberculosis Center, Jacqueline Peterson-Tulsky, MD, Mary
Castle White, PhD, University of California-San Francisco, San Francisco, CA, Renee Kanan, MD, California Department of Corrections,
Sacramento,
California; Madeline Gallagher, Connecticut Department of Corrections, Hartford, Kaveh Khoshnood, PhD, Yale University School of Public
Health, New Haven, Connecticut; Patrick Brown, MD, Florida Department of Corrections,
Talahassie,Tara Wildes, Jails Division, Jacksonville Sheriff's
Office, Jacksonville, Ellen Murray, Florida Department of Health, Tallahassee, Joan Carver, Hillsborough County Sheriff's Office, Robert Lucas, American
Jail Association and Hillsborough County Sheriff's Office, Tampa, Florida; Sidney Parsons, M Eng, American Society of Heating, Refrigerating and
Air-Conditioning Engineers, Michael Puisis, DO, Advisory Council for the Elimination of Tuberculosis, Atlanta, Georgia; Edward Harrison,
National Commission on Correctional Health Care, James McAuley, MD, Rush University Medical School, Mary Muse, MS, Cermak Health Services of
Cook County and Academy of Correctional Health Professionals, Ron Shansky, MD, Society of Correctional Physicians, Chicago, Illinois; Sarah Bur,
MPH, Maryland Department of Health and Federal Bureau of Prisons, Health Services Division, Baltimore, Connie Lawson, American
Correctional Association, Lanham, Maryland; Cheryl Roberts, MPA, Crime and Justice Institute, Boston, Ted Hammett, PhD, Abt Associates,
Cambridge, Massachusetts; Louis Tripoli, MD, Correctional Medical Services, St. Louis, Missouri; Karl Brown, MD, Infectious Diseases, Prison Health
Services, Rikers Island, New York City, Robert B. Greifinger, MD, Dobbs Ferry, Nick Pavelchak, New York State Department of Health, Center
for Environmental Health, Albany, New York; Eileen C. Napolitano, New Jersey Medical School Global Tuberculosis Institute, Newark, New
Jersey; Michael Kelley, MD, MPH, Texas Department of Criminal Justice, Austin, Texas; Teresa Garrett, MS, Division of Epidemiology and
Laboratory Services, Public Health Nursing, Utah Department of Health, Salt Lake City, Utah; Maria Dinger, MS, U.S. Marshals Service, Office of
Interagency Medical Services, Todd Gritch, American Institute of Architects, Lori Hanton, MSN, U.S. Marshals Service, Office of Interagency Medical
Services, Newton Kendig, MD, Federal Bureau of Prisons, Marilyn Moses, National Institute of Justice, Sara Newman, DrPH, Luz Peredo-Berger, MD,
Diana Schneider, DrPH, Health Resources and Services Administration, Division of Immigration Health Services, Donna Olive, MS, Federal Bureau
of Prisons, Health Services Division, Sandra Woerle, National Institute of Justice, Washington, District of Columbia; Phyllis Cruise, Judy Gibson,
MSN, Michael F. Iademarco, MD, Paul Jensen, PhD, Mark Lobato, MD, Philip LoBue, MD, Scott McCoy, MEd, Farah Parvez, MD, Maureen
Wilce, Division of Tuberculosis Elimination; Scott Santibanez, MD, Office of Health Disparities,
National Center for HIV/AIDS, Viral Hepatitis, STD,
and TB Prevention (proposed), Atlanta, Georgia; Stephen Martin, Jr., Christopher Coffey, PhD, National Institute for Occupational Safety and
Health, CDC, Morgantown, West Virginia.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.