 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Visual Impairment and Eye Care Among Older Adults --- Five States, 2005Blindness and visual impairment are among the 10 most common causes of disability in the United States (1) and are associated with shorter life expectancy and lower quality of life (2,3). Previously, state-specific prevalences of visual impairment and eye disease were estimated from national prevalences. However, in 2005, five states (Iowa, Louisiana, Ohio, Tennessee, and Texas) provided state-specific estimates by using the new CDC Behavioral Risk Factor Surveillance System (BRFSS) vision module. CDC analyzed data from the module to determine the self-reported prevalence of visual impairment, eye disease, eye injury, and lack of eye-care insurance and eye examination among persons aged >50 years in each of these five states and among certain sociodemographic populations overall. This report describes the results of that analysis, which indicated variation in disease prevalence and use of eye care among individual states and also among racial/ethnic populations and age groups within the five states combined. The variability among state data suggests that state-specific surveillance of visual impairment and eye care and investigation by states to identify influencing factors might lead to creation of vision programs better suited to individual state needs. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized, U.S. civilian population aged >18 years. The median Council of American Survey Research Organizations response rate for BRFSS in 2005 was 51.1%, with a range among states of 34.6% to 67.4%. Response rates for the five states using the optional BRFSS vision module in 2005 were as follows: Iowa, 60.2%; Louisiana, 51.4%; Ohio, 49.5%; Tennessee, 59.6%; and Texas, 45.2%. Among the five states, Louisiana provided data only for January--August because of Hurricane Katrina. Respondents were classified as having visual impairment if they answered "a little difficulty," "moderate difficulty," "extreme difficulty," or "unable to do because of eyesight" to the question, "How much difficulty, if any, do you have in recognizing a friend across the street?" or to the question, "How much difficulty, if any, do you have watching television?"* Three selected eye diseases (i.e., cataract, glaucoma, and macular degeneration) and workplace eye injury were identified if respondents answered "yes" to the relevant questions.† Diabetic retinopathy was identified (from the BRFSS diabetes module) if respondents with diabetes answered "yes" to the question, "Has a doctor ever told you that diabetes has affected your eyes or that you had retinopathy?" The BRFSS vision module also incorporated questions relating to use of eye care. Respondents were classified as not having eye insurance if they answered "no" to the question, "Do you have any kind of health insurance coverage for eye care?" Respondents were classified as not having had a dilated eye examination in the preceding 12 months if they answered other than "within the past month" or "within the past year (1--12 months ago)" to the question, "When was the last time you had an eye exam in which the pupils were dilated?" They were classified as not having visited an eye-care professional in the preceding 12 months if they answered other than "within the past month" or "within the past year" to the question, "When was the last time you visited any eye-care professional?" In addition, respondents were asked the main reason they had not visited an eye-care professional in the preceding 12 months. The analyses were weighted to make estimates representative of the civilian, noninstitutionalized population in the five states. A total of 13,931 responses§ were analyzed using statistical software to account for the survey design complexity. Trends were assessed using linear regression by the weighted least squares method. The self-reported prevalence of visual impairment and eye disease among persons aged >50 years varied among the five states that used the BRFSS vision module in 2005. The prevalence of visual impairment ranged from 14.3% (95% confidence interval [CI] = 12.9%--15.8%) in Iowa to 20.5% (CI = 18.6%--22.5%) in Ohio (Table 1). Prevalence of cataract ranged from 29.0% (Texas) to 34.3% (Iowa), prevalence of glaucoma ranged from 5.0% (Tennessee) to 7.4% (Louisiana), prevalence of macular degeneration ranged from 3.1% (Tennessee) to 5.4% (Iowa), and prevalence of diabetic retinopathy ranged from 2.7% (Ohio) to 4.3% (Louisiana). The self-reported prevalence of workplace eye injury history ranged from 5.8% (Tennessee) to 9.0% (Iowa) among the five states. With the exception of diabetic retinopathy, women had higher prevalence of visual impairment and eye disease than men. Among age groups, prevalence of cataract and glaucoma increased with age, and prevalence of workplace eye injury history decreased with age (p<0.05). Having eye-care insurance and use of eye care also varied among the five states (Table 2). The percentage of participants reporting no eye-care insurance ranged from 46.2% (Ohio) to 55.0% (Tennessee). In addition, the percentage reporting they had not had a dilated eye examination during the preceding 12 months ranged from 40.6% (Iowa) to 46.2% (Texas); the percentage reporting no visit to an eye-care professional in the preceding 12 months ranged from 30.4% (Iowa) to 34.8% (Texas). Persons in the five states cited "no reason to go" (range: 42.8% in Louisiana to 60.9% in Iowa) and "cost/insurance" (range: 18.5% in Ohio to 22.1% in Tennessee) as the most common reasons for not having visited an eye-care professional in the preceding 12 months. Overall, persons aged 50--59 years were least likely to report not having eye-care insurance. The percentage of persons who had not had a dilated eye examination or a visit to an eye-care professional in the preceding 12 months decreased with increasing age (p<0.05). Men were more likely than women to report not having had a dilated eye examination or not having had an eye-care visit. Having eye-care insurance and use of eye care also varied by race/ethnicity, education, and income (p<0.05). Hispanics were more likely than non-Hispanic whites to report not having eye-care insurance, not having had a dilated eye examination, and not having had an eye-care visit during the preceding 12 months. Respondents with less than a high school education or annual household income <$15,000 were least likely to use eye-care services. Moreover, the percentage without eye-care insurance decreased as education and income levels increased (p<0.05). Reported by: RN Bailey, OD, College of Optometry, Univ of Houston, Texas. RW Indian, MS, Bur of Health Surveillance --- Prevention, Ohio Dept of Health. X Zhang, MD, PhD, LS Geiss, MS, MR Duenas, OD, JB Saaddine, MD, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:This report is the first to provide state-specific estimates of the self-reported prevalence of visual impairment, eye disease, and use of eye-care services. The varied prevalences among states suggest needs for state-level surveillance of visual impairment and investigation of potential barriers to eye care to enable development of vision-loss prevention and eye-health promotion programs tailored to individual state needs. Approximately half of those who did not visit an eye-care professional during the preceding 12 months said they had no reason to go. The lack of concern regarding the need for preventive eye care remains a major public health concern. Early detection and timely treatment can prevent visual impairment and progression of conditions leading to blindness. An annual dilated eye examination is recommended for persons with diabetes or aged >65 years (4); by comparison, approximately 44% of those aged 60--69 years and 32% of those aged 70--79 years had not had a dilated eye examination during the preceding 12 months. Many eye problems are asymptomatic initially, and regular eye examinations can help delay or limit the progression of vision loss and eye diseases (5). In addition, efficacious and cost-effective strategies to detect and treat certain eye diseases exist (6--9). However, in this study, approximately 41%--46% of respondents aged >50 years had not had a dilated eye examination, and approximately 30%--35% had not visited an eye-care professional during the preceding 12 months. The finding that prevalence of workplace eye injury history decreased with increasing age appears counterintuitive and suggests a need for further study. This report is subject to at least three limitations. First, the prevalences of visual impairment and eye diseases are self-reported and might be different than objective clinical measurements. Second, the data are collected by telephone survey and might not be representative of persons without landline telephones. Finally, institutionalized populations (e.g., nursing home residents) are not included in BRFSS. CDC provides resources and technical assistance to state health departments to increase surveillance of visual impairment and eye diseases. The new BRFSS vision module can be used to help public health agencies plan, implement, and evaluate programs on vision-loss prevention and eye-health promotion at national, state, and local levels and can help monitor Healthy People 2010 objectives regarding eye care. These data can enable CDC and states to better assess the need for eye care, identify groups at high risk for eye disease, reduce health disparities, allocate scarce resources, and target effective intervention activities. References
* While wearing glasses or contact lenses, for those who wore them. † "Have you been told by an eye doctor or other health-care professional that you now have cataracts?" "Have you ever been told by an eye doctor or other health-care professional that you had glaucoma?" "Have you ever been told by an eye doctor or other health-care professional that you had macular degeneration?" "Have you ever had an eye injury that occurred at your workplace while you were doing your work?" § Iowa, 2,749; Louisiana, 1,440; Ohio, 3,967; Tennessee, 2,565; and Texas, 3,210.
Table 1 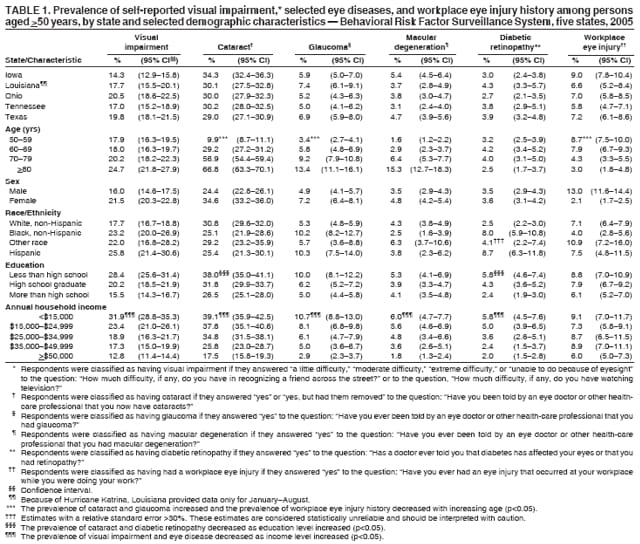 Return to top. Table 2  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/13/2006 |
|||||||||
|