|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
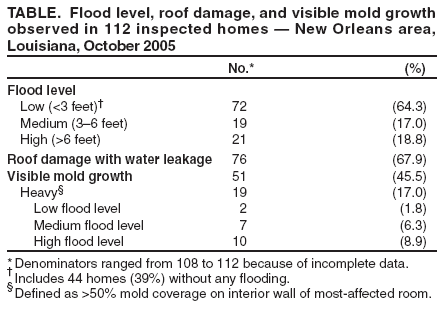
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Health Concerns Associated with Mold in Water-Damaged Homes After Hurricanes Katrina and Rita --- New Orleans Area, Louisiana, October 2005After Hurricanes Katrina and Rita made landfall on August 29 and September 24, 2005, respectively, large sections of New Orleans (Orleans Parish) and the three surrounding parishes (Jefferson, Plaquemines, and St. Bernard) were flooded for weeks, leading to extensive mold growth in buildings. As residents reoccupied the city, local health-care providers and public health authorities were concerned about the potential for respiratory health effects from exposure to water-damaged homes. On October 6, CDC was invited by the Louisiana Department of Health and Hospitals (LDHH) to assist in documenting the extent of potential exposures. This report summarizes the results of that investigation, which determined that 46% of inspected homes had visible mold growth and that residents and remediation workers did not consistently use appropriate respiratory protection. Public health interventions should emphasize the importance of safe remediation practices and ensure the availability of recommended personal protective equipment. Housing Assessment for Mold and Mold ExposureDuring October 22--28, a team representing CDC and LDHH assessed a cross-section of the 440,269 households in the four-parish area (on the basis of the 2000 U.S. Census). Sampling was restricted to blocks with more than 20 housing units (areas with fewer housing units are likely to be sparsely populated and to contain mostly industrial buildings or parks) and areas where residents were permitted entry, yielding 239,949 potential households (Figure). Blocks were classified into three strata (mild, moderate, and severe) on the basis of Federal Emergency Management Agency flood and damage maps. Geographic information system (GIS) mapping software was used to select a random number of waypoints (latitude and longitude) proportionate for each stratum (1). A sample size of 88 homes was required to obtain estimates within 10% accuracy. Global positioning system (GPS) units were used to locate each waypoint as the random starting point to locate the nearest home at or north of the waypoint. In the sampled areas, 141 homes were found to be occupied. A questionnaire on demographics, home occupancy, and participation in remediation activities was administered to one consenting adult from 113 of the 141 homes in which someone was in the home. One assessment was abandoned for safety reasons, resulting in a final sample of 112. A standard instrument designed for this study and pilot-tested with occupants of flood-damaged homes was used to visually assess water damage and mold growth. Air samples were collected at a subset of 20 homes; samples were collected for 36--144 minutes with 0.4 µm, 37 mm polycarbonate closed-faced cassettes at 3 L/min. The filters were analyzed for culturable fungi, (1®3,1®6)-b-D-glucan (a cell-wall component of many fungi) (2), and endotoxin (a cell-wall component of gram-negative bacteria) (3). Of 112 homes inspected (Table), flood levels had been high (>6 feet) in 21 (18.8%) homes, medium (3--6 feet) in 19 (17.0%), and low (<3 feet) in 72 (64.3%) (including 44 [39.3%] homes with no flooding). Seventy-six (67.9%) homes had roof damage with water leakage. Visible mold growth occurred in 51 (45.5%) homes, and 19 (17.0%) had heavy mold coverage (>50% coverage on interior wall of most-affected room). The distribution of homes with heavy mold coverage was 10 (52.6%), seven (36.8%), and two (10.5%) in high, medium, and low flood areas, respectively. Participants reported being indoors doing heavy cleaning an average of 13 hours since the hurricanes (range: 0--84 hours) and 15 hours doing light cleaning (range: 0--90 hours). Sixty-eight (60.7%) participants reported inhabiting their homes overnight for an average of 25 (standard deviation: +13.7) nights since the hurricanes. Indoor air samples were collected nonrandomly at 20 (16%) homes; outdoor air samples were also collected for 11 of these homes. Predominant fungi indoors and outdoors were Aspergillus spp. and Penicillium spp. Geometric mean (1®3,1®6)-b-D-glucan air levels were 1.6 µg/m3 (geometric standard deviation [GSD]: 4.4) indoors and 0.9 µg/m3 (GSD: 2.0) outdoors; endotoxin levels were 23.3 EU/m3 (GSD: 5.6) indoors and 10.5 EU/m3 (GSD: 2.5) outdoors. Glucan and endotoxin levels were significantly correlated (correlation coefficient r = 0.56; p = 0.0095). The geometric mean glucan and endotoxin levels were higher indoors compared with outdoors but the differences were not statistically significant. Survey of Residents and Workers Regarding MoldDuring October 18--23, the assessment team conducted interviews with residents and remediation workers in recently flooded communities at three sites (i.e., the FEMA Disaster Recovery Center in St. Bernard, a home improvement store in West Jefferson, and a grocery store in East Jefferson) and at worker gathering places (e.g., work sites, campsites, and social venues). A convenience sample of residents and remediation workers with potential exposure to mold were asked questions about their knowledge, attitudes, and practices regarding mold; nonidentifying demographic information was also collected. A total of 332 persons (workers and residents combined) were approached for interviews; 235 (70.1%) participated. Interviews were conducted in English and Spanish. A display of respirators was used for reference during the interviews. Of 159 residents interviewed, 82 (51.6%) were male; the overall mean age was 51 years (range: 18--81 years). Nearly all (96.2%) residents responded affirmatively to the question, "Do you think mold can make people sick?" One hundred eight (67.9%) correctly identified particulate-filter respirators as appropriate respiratory protection for cleaning of mold. Sixty-seven (42.1%) had cleaned up mold; of these, 46 (68.7%) did not always use appropriate respirators. Reasons for not using respirators included discomfort (10 [21.7%] respondents) and lack of availability (10 [21.7%]). For public communications about potential risks from exposure to mold and the use of personal protective equipment, 139 (87.4%) respondents recommended the use of television or radio. Seventy-six persons who self-identified as remediation workers were interviewed. Of these, 14 (18.4%) were self-employed, and 62 (81.6%) worked for a company doing remediation. Of the 76 workers, 70 (92.1%) were male; the mean age of respondents was 33 years (range: 18--57 years); 40 (52.6%) spoke only Spanish. Seventy-two (94.7%) thought mold causes illness. Sixty-five (85.5%) correctly identified particulate-filter respirators as appropriate protection for cleaning of mold. Sixty-nine (90.7%) had already participated in mold remediation activities at the time of the interview. Of these, 34 (49.3%) had not been fit tested for respirator use and 24 (34.8%) did not always use appropriate respirators; 13 (54.2%) cited discomfort as the reason for not using respirators. For worker communications about potential risks from exposure to mold and the use of personal protective equipment, 36 (47.4%) recommended use of television or radio and 17 (22.4%) recommended communication through employers. Reported by: R Ratard, MD, Louisiana Dept of Health and Hospitals; CM Brown, MBBS, J Ferdinands, PhD, D Callahan, MD, KH Dunn, MS, MR Scalia, MPH, RL Moolenaar, MD, Div of Environmental Hazards and Health Effects, National Center for Environmental Health; SI Davis, MSPH, Div of Health Studies, Agency for Toxic Substances and Disease Registry; Lynne Pinkerton, MD, Div of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health; C Rao, PhD, D Van Sickle, PhD, MA Riggs, PhD, KJ Cummings, MD, EIS officers, CDC. Editorial Note:In 2004, the Institute of Medicine (IOM) reviewed the literature regarding health outcomes related to damp indoor spaces (4). In addition to the risk for opportunistic fungal infections in immunocompromised persons, IOM found sufficient evidence for an association between both damp indoor spaces and mold and upper respiratory symptoms (nasal congestion and throat irritation) and lower respiratory symptoms (cough, wheeze, and exacerbation of asthma). The findings of this report indicate that, in the New Orleans area post-hurricane, indoor environmental conditions and personal practices provided exposures that potentially put residents and remediation workers at risk for these negative health effects. This study used markers that have been used in exposure assessments in water-damaged buildings, including cultured fungi and microbial structural components (bacterial endotoxins and fungal glucans). Interpreting the significance of these measures is not straightforward, and health-based indoor exposure limits for these compounds have not been established (4,5). Previous measurements of airborne endotoxin in homes have averaged <1.0 EU/m3, with indoor levels generally lower than outdoor ones (6). In post-hurricane New Orleans homes, mean indoor endotoxin levels were more than 20 times higher than the 1.0 EU/m3 average, with an inversion of the expected indoor-outdoor relationship. This mean level exceeds that associated with respiratory symptoms in one study (7). In five New Orleans homes, the measured indoor endotoxin levels were comparable to those of certain industrial settings in which declines in pulmonary function have been demonstrated (8). Exposure to (1®3)-b-D-glucan, a cell-wall component not specific to fungi, has also been linked to respiratory health effects in certain studies (5). In this assessment, a newer assay for (1®3,1®6)-b-D-glucan (2), a different glucan with higher specificity for fungi, yielded higher indoor than outdoor levels in New Orleans homes. Although differences in the two glucan assays preclude direct comparisons, the findings of this assessment indicated that mold growth inside homes was likely at or above a level sometimes reported to be associated with certain health effects (e.g., cough; airway hyper-reactivity; influenza-like symptoms; ear, nose, and throat irritation; decreased lung function; and skin rash) (5). In October 2005, the CDC Mold Work Group published guidelines for remediation workers and the public on preventing mold-associated illness in areas affected by hurricane-related flooding (9). Recommendations included avoiding exposure when possible and using a particulate-filter respirator during activities that create mold-contaminated dust. Despite their awareness of health effects associated with mold, one third of a convenience sample of residents could not identify an appropriate respirator, and the majority of those participating in mold-remediation activities reported doing so without consistently using respiratory protection. Although the majority of remediation workers reported consistently using an appropriate respirator, one third still failed to do so. Even those workers who used respiratory protection consistently might not have benefited from its full effectiveness; only half of the workers reported having had a respirator fit test, an Occupational Safety and Health Administration (OSHA) requirement (10). The findings of this report are subject to at least three limitations. First, because homes at which persons were present likely had less water damage and mold than homes that were unoccupied at the time of the study, this study might have underestimated the extent of mold-contaminated homes. Second, air-sampling results might not be representative because a convenience sample was used and because sampling occurred after six homes had been remediated. Finally, residents and workers surveyed were not randomly selected and might not be representive of their respective populations. This report provides an early assessment of the impact of water damage and mold growth in the New Orleans area after Hurricanes Katrina and Rita. This assessment benefited from the random sampling method used to assess homes and the survey of remediation workers, a group with high potential for exposures. Results of this assessment should be used to guide future public health interventions in this setting and after other catastrophic floods. Specifically, measures to increase awareness of appropriate respiratory protection among the public are warranted. This could be carried out via traditional media announcements and educational sessions for employees of home improvement stores and other commercial entities that sell respirators. Public availability of particulate-filter respirators might be increased through partnerships with respirator manufacturers. For remediation workers, the importance of appropriate respiratory protection should be emphasized via traditional media announcements and/or employers, with messages in both English and Spanish. Fit testing should occur according to the OSHA Standard (10); making such services available to small or individual operators might increase compliance with requirements. Given the extent of flooding in the New Orleans area, exposure to water-damaged buildings and mold will likely be an ongoing problem; investigation of sentinel clinical case reports might enable primary and secondary prevention of exposure-related respiratory disease. Acknowledgments This report is based, in part, on data contributed by GL Chew, ScD, Mailman School of Public Health, Columbia University, New York, New York; PS Thorne, PhD, College of Public Health, University of Iowa, Iowa City, Iowa; M Muilenberg, MS, School of Public Health, Harvard University, Boston, Massachusetts; H Alsdurf, School of Public Health and Tropical Medicine, Tulane University, New Orleans, Louisiana; D Dyce, C Muller, Office of Inspector General, US Department of Health and Human Services; J-H Park, ScD, K Kreiss, MD, Division of Respiratory Disease Studies, M Hein, MS, P Laber, MS, F Armstrong, N Burton, MPH, Division of Surveillance, Hazard Evaluations, and Field Studies, National Institute for Occupational Safety and Health; WR Daley, DVM, Office of Workforce and Career Development; S Hurston, Division of Sexually Transmitted Disease Prevention, National Center for HIV, STD, and TB Prevention; S Benoit, MD, R Noe, MPH, A Sumner, MD, EIS officers, CDC. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/19/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|