|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
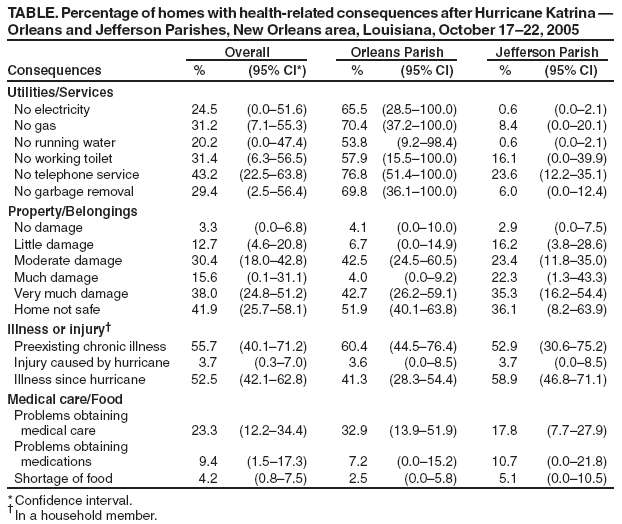
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessment of Health-Related Needs After Hurricanes Katrina and Rita --- Orleans and Jefferson Parishes, New Orleans Area, Louisiana, October 17--22, 2005Residents returning home after natural disasters face numerous physical, mental, and social challenges (1--3). Seven weeks after Hurricane Katrina struck the New Orleans area in Louisiana, causing levees to break and large sections of the city to flood, local authorities had reopened most of Jefferson Parish and much of Orleans Parish to residents. To identify health-related needs among returning parish residents, state and local public health and mental health agencies and CDC conducted an assessment of living conditions, access to basic services, and physical and mental health status. This report describes the results of that assessment, which determined that, approximately 7 weeks after Hurricane Katrina made landfall, 20.2% of housing units lacked water, 24.5% had no electricity, 43.2% had no telephone service, and 55.7% of households contained one or more members with a chronic health condition. In addition, 49.8% of adults exhibited levels of emotional distress, indicating a potential need for mental health services. As a result of these findings, the Louisiana Office of Mental Health established a crisis-counseling program to provide interventions and support to hurricane survivors. Community assessments after natural disasters can identify health-related needs and guide public health interventions. During October 17--22, 2005, survey teams interviewed residents in Orleans Parish, which has the same boundaries as the city of New Orleans, and Jefferson Parish, a suburban area south and west of New Orleans. A total of 45 census blocks were selected by the cumulative sum method, using the total number of housing units in each census block (4). Blocks with 20 or fewer housing units were excluded to increase the efficiency of the assessment. A cluster of four waypoints (i.e., latitude and longitude) in each of the 45 census blocks was randomly generated. Survey teams used global positioning system (GPS) instruments to navigate to the location of each of the 180 waypoints and selected the nearest residence. At multifamily dwellings, teams randomly selected a floor and unit as a starting point. If unable to complete an interview at the starting point, teams noted the reason (e.g., residence destroyed, unoccupied, or resident refused to be interviewed) and proceeded in a systematic manner until one interview was completed. Teams then traveled to the next waypoint within the cluster. Teams continued until they had completed four interviews per cluster or until all residences within the cluster were exhausted. Clusters were visited at most twice to obtain four interviews. To one adult (aged >18 years) resident in each household, interviewers administered a questionnaire concerning basic utilities and services, safety of the home, damage to property and belongings, presence of new persons in the home, health status of household members, and current problems of household members. If more than one adult resident was present, one was chosen at random to represent the household and complete the interview. In addition, each respondent completed an individual assessment that included SPRINT-E, an 11-question postdisaster assessment and referral tool. SPRINT-E contains the Short Post Traumatic Stress Disorder (PTSD) Rating Interview (SPRINT), an eight-question measure that has been determined to have good reliability and convergent validity with other PTSD diagnostic and psychological functioning measures in both clinical trials and population surveys (5). SPRINT-E incorporates three additional questions regarding depression and impaired functioning that were added for use in Project Liberty, the New York crisis-counseling program initiated after the September 11, 2001, terrorist attacks. In New York, responses to SPRINT-E were determined strongly related to perceived need for treatment: 70% of respondents scoring three or more high responses (4 or 5 on a 5-point scale) and 85% of those scoring seven or more high responses out of 11 questions accepted referral for professional mental health services (6). For this assessment, three and seven high responses were used to estimate possible and probable needs, respectively, for mental health assistance. Each survey team included a local mental health professional to provide support and referrals if desired. Teams also had access to two onsite psychiatrists and one clinical psychologist if acute mental health needs were identified in the field or among study personnel. Statistical analyses accounted for the cluster design, and responses were weighted on the basis of sampling probabilities. A total of 24 census blocks were selected in Orleans Parish and 21 in Jefferson Parish. Survey teams contacted 224 persons and successfully interviewed 166 (74%); 58 persons refused. Eighty-four interviews were conducted in Jefferson Parish and 82 in Orleans Parish. No interviews could be completed in two Orleans parish blocks; one had been destroyed and the other converted to commercial use. In four other blocks in Orleans Parish, survey teams completed fewer than four interviews because few residents were encountered. Overall, fewer residents had returned to the selected blocks in Orleans Parish than to those in Jefferson Parish. A substantial percentage of housing units did not have basic utilities and services (Table). This varied markedly between Jefferson and Orleans Parishes, reflecting a greater level of damage to the infrastructure in Orleans Parish. In Orleans Parish, more than 50% of housing units lacked running water and working toilets, more than 60% lacked electricity and garbage removal service, and more than 70% lacked gas and telephone service. In Jefferson Parish, 23.5% of homes lacked telephone service and 16.1% reportedly lacked working toilets, although this was primarily the result of needed repair work not lack of water service. Overall, 41.9% (95% confidence interval [CI] = 25.7%--58.1%) of respondents did not consider their homes safe at the time of the interview, including 51.9% (CI = 40.1%--63.8%) in Orleans Parish and 36.1% (CI = 8.2%--63.9%) in Jefferson Parish. An estimated 25.5% (CI = 7.2%--43.8%) of households included additional persons after the hurricanes, including 31.7% (CI = 4.3%--59.1%) in Jefferson Parish and 14.8% (CI = 0.0--33.9%) in Orleans Parish. In 1 month, 65.9% (CI = 7.2%--43.8%) of persons expected to be living in the housing unit where they were interviewed. Overall, 55.7% (CI = 40.1%--71.2%) of households included at least one member with a preexisting chronic health condition; 52.5% (CI = 42.1%--62.8%) included a person that had been ill in the 7--8 weeks since Hurricane Katrina. Problems obtaining medical care and prescription medications were reported in 23.3% (CI = 12.2%--34.4%) and 9.4% (CI = 1.5%--17.3%) of households, respectively. Problems obtaining medical care included closure of the usual health-care provider site and insurance/financial concerns. Problems obtaining medications included loss of or difficulty obtaining prescriptions, insurance/financial concerns, and pharmacy closure. A substantial proportion of adults had lost their means of employment since Katrina; 72.8% (CI = 60.2%--85.3%) reported being employed before Katrina, compared with 34.5% (CI = 14.1%--54.9%) at the time of the interview. Respondents frequently identified emotional concerns as current problems in their household: feeling isolated (42.8%), feeling crowded (38.1%), feeling overwhelmed as a parent (23.6%), and family conflict (18.4%). According to interview responses, an estimated 25.9% (CI = 21.2%--30.5%) of households contained one or more members in need of counseling services, but only 1.6% (CI = 0.0%--3.2%) contained a person who had used counseling services since the hurricane. However, on the SPRINT-E assessment, 49.8% (CI = 37.3%--62.2%) of respondents scored three or more high responses, indicating possible need for mental health services. In addition, 33.1% (CI = 17.7%--48.6%) scored seven or more high responses, indicating probable need for mental health services. These percentages did not vary significantly between Jefferson and Orleans parishes. Most respondents identified financial concerns (34.7%), housing (24.9 %), or emotional support (8.3%) as their family's greatest need. Reported by: FH Norris, PhD, National Center for Post Traumatic Stress Disorder, White River Junction, Vermont. A Speier, PhD, Louisiana Office of Mental Health. AK Henderson, PhD, SI Davis, MSPH, Div of Health Studies, Agency for Toxic Substances and Disease Registry. DW Purcell, PhD, BD Stratford, PhD, Div of HIV/AIDS Prevention, National Center for HIV, STD, and TB Prevention; CK Baker, PhD, DB Reissman, MD, Div of Violence Prevention, National Center for Injury Prevention and Control; WR Daley, DVM, Career Development Div, Office of Workforce and Career Development, CDC. Editorial Note:This assessment documents that, approximately 7 weeks after Hurricane Katrina struck the New Orleans area, most residential areas in Orleans Parish were still without basic public utilities and services such as water, electricity, gas, and garbage removal. Conversely, most utilities had been restored in Jefferson Parish, although some homes still lacked telephone service. The status of Jefferson Parish 7 weeks after the hurricane resembled that reported for other U.S. communities more than 2 weeks after disasters (7,8), whereas the basic environmental health needs in Orleans Parish were more similar to the needs in other locations in the immediate aftermath of major hurricanes (9,10). In both parishes, the majority of households contained one or more person with a chronic illness, indicating a need for adequate health care and pharmacy services for returning residents. Major population disruption existed at the time of this assessment. Approximately one fourth of households included a person not present in the household before Katrina struck, and many persons returning to the area were still unable to live in their homes. Many respondents were unemployed and identified emotional concerns among members of their family. Nearly half of the respondents had high levels of distress/dysfunction, indicating likely needs for mental health services. However, only one fourth said a household member needed counseling services, and few had used any counseling services. Changed living environments and disruption of preexisting social networks can result in various mental health problems (1--3,7). Mental health interventions should be included within a public health strategy for rebuilding community services and civic networks. Optimal use of mental health services might require community outreach and education activities after natural disasters; combining mental health services with family medical care and social services might reduce stigma associated with mental health services and promote their use. The findings in this report are subject to at least four limitations. First, no stable population estimates existed; survey design was based on preexisting population distribution. Second, findings likely underestimated the severity of conditions because some heavily damaged areas were not sampled. Third, vacant homes were replaced by households with a person present, creating a bias toward persons more likely to be at home (e.g., retired or elderly). Finally, the SPRINT-E assessment has been evaluated as a referral tool by crisis counselors in a clinical setting but has not been evaluated for use 7 weeks after a natural disaster in a field environment; responses and interpretations might vary. However, the original SPRINT, on which SPRINT-E was based, demonstrated strong validity in both clinical and community populations (5). The results of this assessment were provided to the Louisiana Office of Mental Health within 2 weeks of initiation and were used to guide strategies for providing medical, social, and mental health services. Crisis-counseling services were initiated that, when integrated with social service interventions, might begin to restore stability to disrupted social networks. As both the current conditions and resident population continue to change, ongoing assessment will be required to track evolving health needs and evaluate the effectiveness of implemented programs. Acknowledgment This report is based, in part, on contributions by the Orleans and Jefferson Parish Offices of Mental Health and the CDC Mental Health and Community Resilience Team, New Orleans. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 1/19/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|