 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Acute Public Health Consequences of Methamphetamine Laboratories --- 16 States, January 2000--June 2004Methamphetamine (meth), a powerfully addictive stimulant, can be easily produced in illicit, makeshift laboratories and generally is considered the fastest-growing illicit drug in the United States (1). Aside from the inherent physical and physiological dangers of the drug itself, persons in and around meth laboratories can be acutely exposed to hazardous substances used in meth production. Exposure to these substances can occur from volatile air emissions, spills, fires, and explosions. This report describes examples of meth-associated events, summarizes the events reported to the Agency for Toxic Substances and Disease Registry (ATSDR), and suggests injury prevention recommendations, such as how to recognize and properly respond to meth laboratories. ATSDR maintains the Hazardous Substances Emergency Events Surveillance (HSEES) system to collect and analyze data about the public health consequences (e.g., morbidity, mortality, and evacuations) of acute hazardous substance--release events*. The data in this report are based on events reported to HSEES from 16 state health departments† during January 1, 2000--June 30, 2004§. Case ReportsMinnesota. In June 2004, two men, aged 31 and 41 years, were manufacturing meth in a camper when a flash fire and explosion occurred. Chemicals being used included acetone, propane, solvent not otherwise specified (NOS), and meth chemicals NOS. Both men received thermal burns and transported themselves to the hospital without assistance from emergency medical services. The older man was treated at the hospital and admitted with burns on his hands, arms, and knees. The man aged 31 years received burns on 80% of his body and died at the hospital. The fire had burned out by the time authorities responded. New York. In January 2003, a police officer noted an odor of ammonia on a stranded motorist he was aiding. The motorist, aged 35 years, complained of respiratory and eye irritation but was not treated. Federal drug agents were notified and searched the homes of the motorist and his neighbor. Substances used to make meth, including ammonia, sulfuric acid, lithium, sodium hydroxide, and ether, were found at the two homes. Access was restricted to the homes while cleanup and environmental sampling were conducted. Iowa. In November 2002, three occupants (aged 18, 19, and 20 years) of an apartment were making meth in a bathroom using ether, muriatic acid, and other meth chemicals NOS. A flash fire occurred; two men received thermal burns, and a woman received nonchemical-related trauma injuries when she jumped through a window. Both men were admitted to a hospital; the woman was treated at a hospital but not admitted. Twenty-four apartment building residents were evacuated for 3 hours while police, firefighters, and emergency medical technicians responded and initiated clean-up. Summary of HSEES System DataOf the 40,349 events reported to the HSEES system during January 1, 2000--June 30, 2004, a total of 1,791 (4%) were associated with illicit meth production. Meth events were reported in 15 of the 16 HSEES states, with Washington (399 events [22%]) and Missouri (351 [20%]) reporting the most events (Figure). The number of meth events increased during the analysis period, from 184 during all of 2000 to 320 during January--June 2004. Of the known meth-event locations (1,544 [86%]), releases occurred most frequently in private households (842 [55%]) and agricultural settings (e.g., farms and farm supply stores) (117 [8%]). The most common substances associated with meth events were ammonia (16%), meth chemicals NOS (13%), and hydrochloric acid (8%). Of the 1,791 meth events, 186 (10%) involved fires or explosions. Meth events consistently had a higher percentage of persons with injuries (i.e., victims) than did nonmeth events (Table). Of the 1,791 meth events, 558 (31%) resulted in a total of 947 injured persons. Persons most frequently injured were police officers (531 [56%]) and members of the general public (314 [33%]). Median age of victims was 32 years (range: <1--72 years). The 947 victims had a total of 1,371 reported injuries, most frequently respiratory irritation (531 [39%]), headache (348 [26%]), eye irritation (109 [8%]), and burns (104 [8%]). A total of 274 (29%) victims were treated at hospitals but not admitted, 68 (7%) were treated at hospitals and admitted, and 62 (7%) were treated at the scene; nine (1%) died. A total of 255 (13%) meth events involved ordered evacuations. The number of evacuees was known for 203 (80%) of these events. A total of 2,732 persons were known to have evacuated, ranging from one to 300 persons per event (median: five persons). Median length of evacuation was 3 hours (range: <1--96 hours). Decontamination of potentially exposed persons was necessary in 288 (16%) events. A total of 1,154 persons underwent decontamination; 698 (60%) were emergency responders, and 396 (34%) were members of the general public. Reported by: D Cooper, Iowa Dept of Public Health. N Rice, Minnesota Dept of Health. R Wilburn, MPH, New York State Dept of Health. DK Horton, MSPH, S Rossiter, MPH, Div of Health Studies, Agency for Toxic Substances and Disease Registry. Editorial Note:This report illustrates the dangers associated with illicit meth laboratories. Substances used in these laboratories are corrosive, explosive, flammable, and toxic and can cause fires, explosions, and other uncontrolled reactions (4,5). An estimated 20%--30% of known meth laboratories are discovered because of fires and explosions (6). These laboratories are located in various environments, including private residences, motel rooms, rental storage facilities, campgrounds, and motor vehicles (4,7). Historical data from the Drug Enforcement Administration (DEA) demonstrate a substantial increase in the numbers of meth laboratories seized by law enforcement officials, from 263 in 1994 to 1,815 in 2000, representing a 590% increase (8). Relative ease of production, short production time, and profit potential are possible reasons contributing to the likely increase in the numbers of laboratories discovered. Similar to DEA data, the overall numbers of meth events in the HSEES system appear to be increasing. Although this trend might be attributed to an actual increase in the number of laboratories, the addition of a new state during the analysis period and better reporting might have also contributed to an increase in meth events. Meth events accounted for a limited number of HSEES events; however, they resulted in a greater overall percentage of victims than nonmeth events (31% and 7%, respectively). The majority of victims were emergency responders who usually arrive first on the scene to secure the area or provide rapid onsite emergency care to victims. A previous analysis suggests that many responders might not have sufficient information to alert them that they are responding to a meth event (3). In addition, many responders do not wear personal protective equipment appropriate for entering meth laboratories. Another group vulnerable to meth laboratory toxicity is children; an estimated 20% of meth laboratories have children present (1). A recent HSEES analysis indicated that at least eight known meth events involved 13 children who were injured after being exposed to lethal substances such as anhydrous ammonia and acid (9). The findings in this report are subject to at least two limitations. First, reporting of any event to HSEES is not mandatory; therefore, participating state health departments might not be informed about every event. In addition, because meth laboratories are illicit, sources (e.g., primarily law enforcement officials) might hesitate to report events that could jeopardize criminal investigations. Second, HSEES is not conducted in all states; therefore, HSEES data might not be representative of populations in other areas. To prevent chemical exposures and injuries, emergency responders and the public should be educated to recognize meth laboratories (10) (Box 1), particularly in areas where they are prevalent. In addition, certain interventions can reduce the risk for injury among emergency responders at meth events (3) (Box 2). HSEES data have been used by ATSDR and participating states for conducting hazardous substances injury-prevention outreach activities (e.g., presentations, fact sheets, and articles) for emergency responders, employers, and the general public. Additional information on HSEES is available at http://www.atsdr.cdc.gov/HS/HSEES. Acknowledgments The findings in this report are based, in part, on contributions by T Arant, Alabama Dept of Public Health. C Kelley, Colorado Dept of Health. D Dugas, MPH, Louisiana Dept of Health and Hospitals. R Mozingo, Mississippi State Dept of Health. C Henry, Missouri Dept of Health and Senior Svcs. J Savrin, New Jersey Dept of Health and Senior Svcs. S Giles, North Carolina Dept of Health and Human Svcs. T Tsongas, PhD, Oregon Public Health Svcs. L Phillips, Rhode Island Dept of Health. R Harris, Texas Dept of Health. W Ball, PhD, Utah Dept of Health. W Clifford, Washington Dept of Health. J Drew, Wisconsin Dept of Health and Family Svcs. References
* An HSEES event is the release or threatened release of a hazardous substance into the environment in an amount that requires (or would have required) removal, cleanup, or neutralization according to federal, state, or local law (2). A hazardous substance is one that can reasonably be expected to cause an adverse health effect. † Alabama, Colorado, Iowa, Louisiana, Minnesota, Mississippi, Missouri, New Jersey, New York, North Carolina, Oregon, Rhode Island, Texas, Utah, Washington, and Wisconsin. § An earlier HSEES analysis examined data for 1996--1999 because 1996 was the first year in which several meth events appeared in the system (3). Data as of June 30, 2004, were the most recent data available when the analysis was conducted; data for 2004 are still considered preliminary.
Box 1 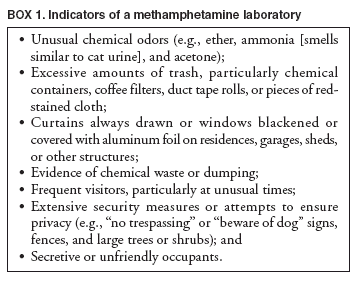 Return to top. Box 2 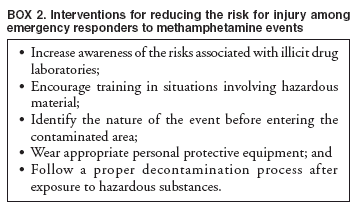 Return to top. Table 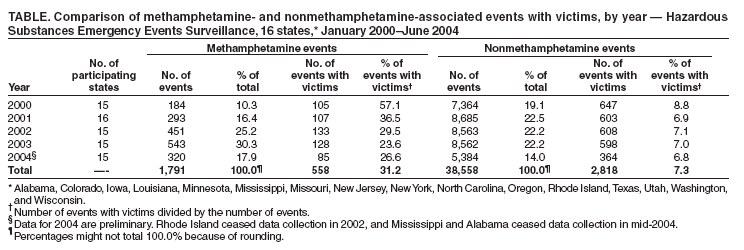 Return to top. Figure 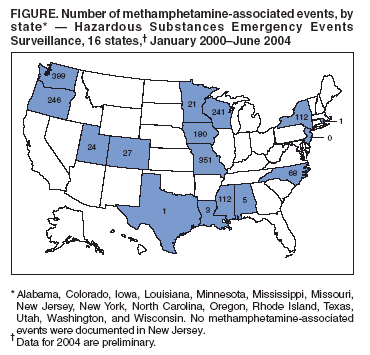 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 4/14/2005 |
|||||||||
|