 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Prevalence of Doctor-Diagnosed Arthritis and Possible Arthritis --- 30 States, 2002Arthritis is the leading cause of disability in the United States (1), and its prevalence is expected to increase as the U.S. population ages (2). State-specific estimates of the prevalence of this condition are key to planning health services and programs to prevent arthritis-related disability and to track progress toward meeting national health objectives for 2010 (objectives 2.1--2.8) (3). In 2002, new questions about arthritis were released as an optional module of the Behavioral Risk Factor Surveillance System (BRFSS), and 30 states elected to use the module. This report summarizes results from the 2002 BRFSS on prevalence of doctor-diagnosed arthritis and possible arthritis. The findings indicate that the estimated prevalence of doctor-diagnosed arthritis among adults in the 30 states ranged from 17.8% to 35.8%, and the prevalence of possible arthritis ranged from 10.3% to 21.3%. Increased intervention efforts, including early diagnosis and appropriate clinical and self-management (e.g., physical activity, education, and maintaining appropriate weight), are needed to reduce the impact of arthritis. BRFSS is a state-based, random-digit--dialed telephone survey of the noninstitutionalized, civilian U.S. population aged >18 years. The survey is administered in all 50 states, the District of Columbia, and Puerto Rico. In 2002, respondents in 30 states were asked, "Have you ever been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?" Those who answered "yes" were classified as having doctor-diagnosed arthritis. Respondents also were asked, "The next questions refer to your joints. Please do not include the back or neck. During the past 30 days, have you had any symptoms of pain, aching, or stiffness in or around a joint?" and "Did your joint symptoms first begin more than 3 months ago?" Those who answered "yes" to both were classified as having chronic joint symptoms (CJS). Those with CJS but without doctor-diagnosed arthritis were classified as having possible arthritis. The median response rate for the 30 selected states in 2002 was 58.3% (range: 42.2% [New Jersey]--82.6% [Minnesota]) (4). Data were weighted by age and sex to reflect each state's most recent estimate of the adult population. SUDAAN was used to calculate point estimates and 95% confidence intervals (CIs). During 2002, the prevalence of doctor-diagnosed arthritis ranged from 17.8% in Hawaii to 35.8% in Alabama (median: 27.6%). Among all 30 states, the prevalence of doctor-diagnosed arthritis was higher among women and increased with age (Table 1). The prevalence of possible arthritis ranged from 10.3% in Hawaii to 21.3% in Iowa (median: 17.3%) (Table 2). Possible arthritis was more prevalent among men in 28 states (medians: men, 18.9% [range: 11.2%--23.2%] and women, 15.5% [range: 9.5%--20.4%]) and was consistently more prevalent among persons aged <65 years (medians: aged 18--44 years, 18.3% [range: 10.0%--22.8%]; aged 45--64 years, 18.3% [range: 13.0%--22.7%]; and aged >65 years, 10.7% [range: 6.1%--14.8%]). Reported by: J Bolen, PhD, CG Helmick, MD, JJ Sacks, MD, G Langmaid, Div of Adult and Community Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report provide the first state-specific estimates of doctor-diagnosed arthritis using the new BRFSS module. Doctor-diagnosed arthritis affects a median of 27.6% of adults in 30 states and occurs more frequently among women and older adults. An additional median of 17.3% of adults had possible arthritis. Persons with doctor-diagnosed arthritis tend to report more activity limitation and likely have more severe symptoms than those with possible arthritis. Unlike doctor-diagnosed arthritis, possible arthritis occurred more frequently among men and adults aged <65 years. In 1990, the National Arthritis Data Work Group defined approximately 150 conditions and the associated International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes thought to represent arthritis and other rheumatic conditions (5). However, a practical method to estimate arthritis prevalence by state by using ICD-9-CM codes and other health-care system data has not been developed. As a result, self-reported data are needed to estimate prevalence of doctor-diagnosed arthritis. Because many persons with arthritis do not visit a clinician for their symptoms and their conditions remain undiagnosed, self-report surveys also are needed to estimate possible arthritis in the population (6). The self-report methods used to estimate arthritis and possible arthritis at the state and national levels have evolved over time. During 1996--2001, self-report questions on doctor-diagnosed arthritis and CJS were used in BRFSS (Table 3). To address cognitive problems with these questions, they were revised; those revisions were used for the 2002 BRFSS survey (Table 3). The method of estimating population burden also has evolved over time. During 1996--2001, burden was estimated by totaling doctor-diagnosed arthritis and possible arthritis. However, CDC observed that this approach produced unstable estimates in states from year to year. In consultation with arthritis public health experts, states, and health officials, CDC began to focus on doctor-diagnosed arthritis to estimate population burden starting in 2002 and to report possible arthritis separately. The shift to using doctor-diagnosed arthritis is consistent with the approach used by other programs (e.g., asthma surveillance) to estimate burden (7). The findings in this report are subject to at least three limitations. First, the estimates use self-reported data that were not confirmed by a physician. Second, BRFSS is a telephone survey and does not include persons without telephone service or those in the military or in institutions. Finally, the median response rate for the survey was 58.3%; however, the distribution of demographic characteristics in the BRFSS sample was similar to the distribution based on U.S. census data (i.e., by sex, age, and race/ethnicity). The CDC Arthritis Program funds programs in 36 states that rely on BRFSS data to monitor the burden of arthritis and to target programmatic interventions. BRFSS and the National Health Interview Survey (NHIS) have used identical arthritis questions since 2002 to define doctor-diagnosed arthritis and possible arthritis. To maintain consistency and allow comparison, states should use doctor-diagnosed arthritis to define the burden of arthritis when reporting prevalence for 2002 and beyond for BRFSS and NHIS data. Efforts are under way to better characterize persons with possible arthritis and to identify the best approach to incorporate them into measuring the burden of arthritis. Evidence-based intervention programs (e.g., the Arthritis Foundation's People with Arthritis Can Exercise [PACE] or aquatics programs) and self-management education programs (e.g., the Arthritis Self-Help Course, which has helped persons with arthritis and joint symptoms experience less pain and reduce the number of clinical visits) (8) should continue to be offered to persons with doctor-diagnosed arthritis; persons with possible arthritis also might benefit. Additional information about these programs is available at http://www.arthritis.org/events/getinvolved/programsservices. Acknowledgment This report is based on data contributed by state BRFSS coordinators and arthritis program contacts. References
Table 1  Return to top. Table 2 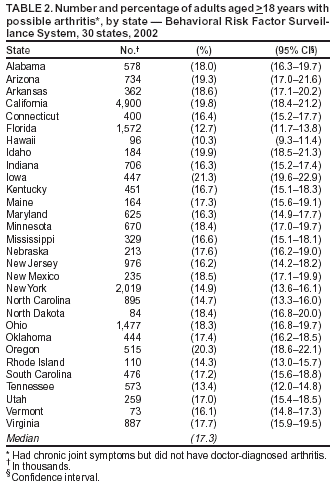 Return to top. Table 3  Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/12/2004 |
|||||||||
This page last reviewed 5/12/2004
|