|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
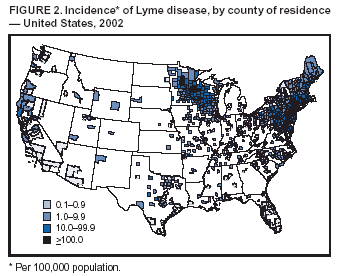
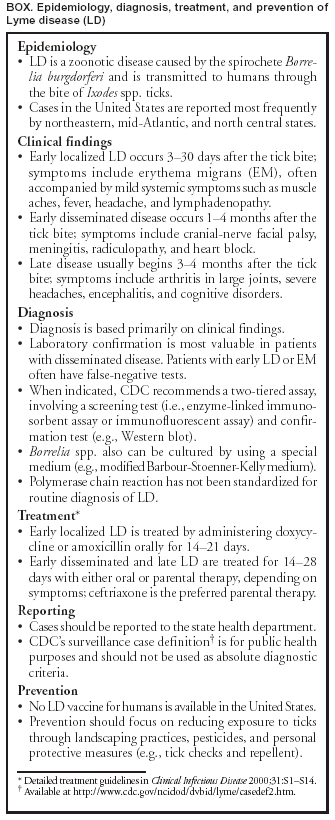
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Lyme Disease --- United States, 2001--2002Lyme disease (LD) is caused by the spirochete Borrelia burgdorferi and is transmitted through the bite of Ixodes spp. ticks. CDC began LD surveillance in 1982, and the Council of State and Territorial Epidemiologists designated LD a nationally notifiable disease in 1991. This report summarizes the analysis of 40,792 cases of LD reported to CDC during 2001--2002. The results of that analysis indicate that annual LD incidence increased 40% during this period. The continued emergence of LD underscores the need for persons in areas where LD is endemic to reduce their risk for infection through integrated pest management, landscaping practices, repellent use, and prompt removal of ticks. For surveillance purposes, a case of LD is defined as physician-diagnosed erythema migrans (EM) >5 cm in diameter or at least one objective manifestation of late LD (e.g., musculoskeletal, cardiovascular, or neurologic) with laboratory confirmation of B. burgdorferi infection using a two-tiered assay (1). National, state, and age-specific incidence was calculated by using U.S. Census Bureau data for 2001 and 2002; incidence by county was calculated by using U.S. Census data for 2000. In 2001, a total of 17,029 cases of LD were reported to CDC by 43 states and the District of Columbia, yielding a national incidence of 6.0 cases per 100,000 population. In 2002, the number of reported cases increased 40% to 23,763 cases, yielding a national incidence of 8.2 cases per 100,000 population (Table, Figure 1). All states except Hawaii, Montana, and Oklahoma reported cases during 2002. Twelve states reported an incidence of LD that was higher than the national average in both 2001 and 2002: Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, and Wisconsin. These 12 states account for 95% of cases reported nationally (Table, Figure 2). During 2000--2001, LD case reports increased in 15 states, decreased in 26 states, and remained the same in nine states. During 2001--2002, LD case reports increased in 39 states, decreased in seven states, and remained the same in four states. Only one state, Arkansas, reported a decrease for both 2001 and 2002. Counties reporting >15 cases accounted for >90% of all cases reported in both years. During 2001--2002, the number of counties reporting >15 cases increased from 123 to 151. In 2001, a total of 35 counties in seven states (Connecticut, Delaware, Massachusetts, New Jersey, New York, Pennsylvania, and Rhode Island) reported >100 cases. In 2002, a total of 53 counties in 10 states (i.e., the seven states from 2001 plus Maine, Minnesota, and New Hampshire) reported >100 cases. For both 2001 and 2002, the highest incidence of LD was reported from Columbia County, New York, with 1,026 and 1,583 cases per 100,000 population, respectively. Combining data for both years, information on patient age and sex was available for 99% of patients. Patient ages ranged from <1 to 101 years and followed a bimodal distribution, with incidence peaks among children aged 5--14 years (9.9 cases per 100,000 population per year) and adults aged 50--59 years (9.2 cases per 100,000 population per year). Overall, 21,525 (53%) of 40,440 patients were male. Demographic features differed for states with above- and below-average incidence. Among 12 states with above-average incidence, the modal age of patients was 6 years; 54% were males. Among 38 states with below-average incidence, the modal age of patients was 44 years; 47% were males. A total of 83% of reports for 2001 and 2002 had a date of illness onset provided. Patients were most likely to have illness in May (7%), June (28%), July (31%), or August (12%). Fewer than 7% were reported to have illness onset during December--March. Among 31,120 patients for whom at least one clinical finding was indicated, a history of EM was reported for 21,126 (68%) patients, arthritis for 10,126 (33%) patients, Bell's palsy for 2,510 (8%) patients, and radiculopathy for 1,009 (3%) patients. Meningitis, encephalitis, and heart block were reported in <1% of patients. Reported by: State and District of Columbia health departments. RM Bacon, MS, PS Mead, MD, JL Kool, MD, AS Postema, MPH, Div of Vector-Borne Infectious Diseases, National Center for Infectious Diseases; JE Staples, MD, EIS Officer, CDC. Editorial Note:During 2002, a total of 23,763 LD cases were reported to CDC, more than in any previous year. Analysis of 2001 and 2002 data indicates that, as in previous years, most cases occur in northeastern, mid-Atlantic, and north central states, and the largest proportion of cases are reported among persons aged 5--14 years and 50--59 years. Factors potentially contributing to the increase in reported cases include growing populations of deer that support the Ixodes tick vector, increased residential development of wooded areas, tick dispersal to new areas, improved disease recognition in areas where LD is endemic, and enhanced reporting. Surveillance for LD is subject to several limitations. Studies from the early 1990s suggested that LD cases were underreported by six to 12-fold in some areas where LD is endemic (2,3); the current degree of underreporting for national data is unknown. In addition, differences in the demographics of reported cases among states with above- and below-average incidence suggest variation in diagnostic and reporting practices among states. Clinicians are reminded that the LD case definition was developed for surveillance purposes and might not be appropriate for clinical management of individual patients (1). In February 2002, the only Food and Drug Administration--approved LD vaccine for humans was withdrawn from the market, reportedly because of poor sales. However, several other effective preventive measures remain available to persons living in areas where LD is endemic (4). Personal protective measures, such as repellent use and routine tick checks, are key components of primary prevention (Box). Removing infected ticks within 48 hours of attachment can reduce the likelihood of transmission (5), and prompt antimicrobial prophylaxis of tick bites, although controversial, might be beneficial under certain circumstances (6). Exposure to ticks in peridomestic and recreational areas can be reduced 50%--90% through simple landscaping practices, such as removing brush and leaf litter or creating a buffer zone of wood chips or gravel between forest and lawn or recreational areas (4,7) (Figure 3). Correctly timed applications of pesticides to yards once or twice a year can decrease the number of nymphal ticks 68%--100% (8,9). In addition to these interventions, several novel approaches to LD prevention are under investigation or will soon be available. These include bait boxes and "four-poster" devices that deliver acaricides to rodents and deer without harming them, and the use of biologic agents, such as fungi that kill Ixodes ticks (4,10). References
Table 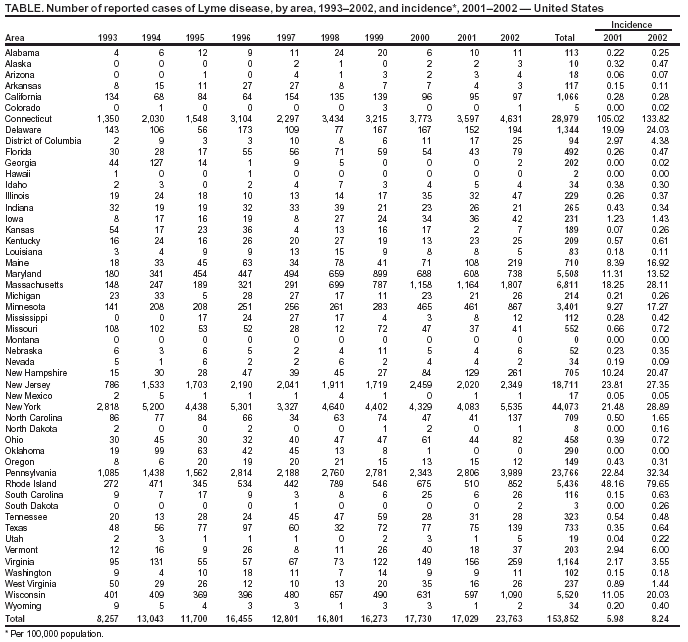 Return to top. Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 5/6/2004 |
|||||||||
This page last reviewed 5/6/2004
|