 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tuberculosis Outbreak in a Community Hospital --- District of Columbia, 2002After declining for nearly 30 years, during 1985--1992, tuberculosis (TB) rates in the United States experienced a resurgence, and several large nosocomial TB outbreaks occurred (1). Although data on such outbreaks are not collected systematically by CDC, the occurrence of nosocomial TB is believed to have declined sharply since the issuance and widespread implementation of infection-control guidelines in 1994 (2--4). During April 2--September 12, 2002, TB was diagnosed in six persons who either had been patients or had worked in a large community hospital (hospital A) in March or early April. This report describes the results of an investigation of the presumed source patient, who had spent 3 weeks on two general medical wards of hospital A before being placed in respiratory isolation and having TB diagnosed on April 2. To prevent transmission of Mycobacterium tuberculosis, hospital staff should remain vigilant to identify and treat suspected TB cases promptly. In July 2002, after five patients at hospital A had been diagnosed with TB, the District of Columbia Department of Health requested epidemiologic assistance from CDC. An investigative team, consisting of CDC staff, the local health department TB-control program, and the infection-control department of hospital A was formed. The team conducted a contact and case-finding investigation by reviewing hospital and health department records of all six patients. Three patients were interviewed, including the index patient. An expanded contact investigation extended to persons possibly exposed to patients with TB disease at the hospital. Patients who spent >1 day on the same medical ward with the index patient were identified through the hospital A admission database and medical ward logs. Hospital staff contacts who were determined from the index patient's medical record and from hospital employment records were categorized as 1) direct-care providers, 2) workers assigned to the same ward but not involved in the patient's medical care, or 3) other workers who spent time on the medical ward but were not assigned there. Latent TB infection (LTBI) was diagnosed in anyone with a tuberculin skin test (TST) reaction of >5 mm induration who did not have evidence of TB disease on the basis of symptom and chest radiographic evaluation. Among staff contacts, a positive TST was defined as induration of >5 mm during the investigation in a person with a documented negative TST during the preceding 2 years (5). M. tuberculosis isolates from all six patients were sent to CDC for genotyping. Index PatientThe index patient was a man aged 42 years with schizophrenia and acquired immunodeficiency syndrome (AIDS). The mental illness contributed to patient-care problems because of inability of the patient to understand questions and follow instructions. He was admitted twice to a different hospital (hospital B) in late February 2002 for fever and nonproductive cough. His chest radiographs were interpreted as normal. He produced one sputum specimen, which was negative for acid-fast bacilli (AFB), before leaving the hospital against medical advice. In early March, he was admitted to hospital A with similar symptoms, treated with intravenous vancomycin for a presumed central line infection, and released after a 6-day hospital stay. Three days later, he returned to the hospital. His CD4 T-lymphocyte count was 30 cells/µL. A chest radiograph revealed hilar adenopathy, and a computerized tomography scan of the chest revealed a questionable left upper lobe infiltrate thought to represent pneumonia; ceftriaxone was administered. On April 2, the hospital staff learned that a stool culture obtained during the patient's first admission had grown M. tuberculosis. The patient was placed in isolation that day. Three subsequent sputum specimens were 4+ AFB smear-positive, indicative of a high degree of infectiousness, and a contact investigation was initiated. The index patient was ambulatory and was in contact with several patients and medical personnel. This contact continued even after the patient was placed in isolation. Secondary PatientsDuring June 21--September 12, five secondary TB patients were identified. Four were men aged 35--49 years who had been hospitalized in different rooms on the same medical ward as the index patient. All four had at least one condition associated with increased risk for progression to TB disease (one had human immunodeficiency virus [HIV] infection and diabetes, one had diabetes, and two had end-stage renal disease) (1). The fifth secondary patient was a phlebotomist on the same medical ward as the index patient. She had been evaluated in May and found to have a TST of 50 mm induration. She was asymptomatic at that time. Because of slightly elevated serum liver enzyme concentrations, she was not treated for LTBI and was monitored only for development of symptoms. In September, she had TB diagnosed. All five secondary patients received diagnoses 3--6 months after exposure to the index patient (Figure). M. tuberculosis isolates from all six patients had matching genotypes by three methods (i.e., identical spoligotyping, mycobacterial interspersed repetitive units, and a 6-band pattern on restriction fragment-length polymorphism). All strains were susceptible to isoniazid and rifampin. Contact InvestigationOf the 1,045 contacts who were identified as having been exposed to the index patient during March 9--April 2 at hospital A, 261 (25%) were patients, and 784 (75%) were staff. All staff contacts with positive TST reactions were evaluated for disease by symptom assessment and chest radiograph. Among the 784 staff members, 106 (14%) provided direct care to the index patient, 49 (6%) were ward-based staff, and 629 (80%) were other staff who had spent some time on the ward during the admissions of the index patient. Of 261 patient-contacts, 173 (66%) received TSTs, and 39 (23%) had a positive reaction. In addition, 495 (63%) of 784 staff members were evaluated with TSTs; 56 staff members tested positive, of whom 21 (38%) were direct-care providers, six (11%) were ward-based staff, and 29 (52%) were other staff (Table). During the investigation, hospital A engineers and the infection-control staff determined that the index patient's room met specifications for an airborne infection isolation room. Infection-control staff at hospital B also were notified about the index patient so that a contact investigation could be initiated there. Contacts with HIV and a negative TST were recommended for therapy with isoniazid for 9 months (1). Staff contacts who did not know their HIV status were offered voluntary HIV counseling and testing. Foreign-born persons and contacts with a previous positive TST reaction were offered treatment if they had no past history of treatment. Reported by: MA Tipple, MD, W Heirendt, Virginia Dept of Health. B Metchock, DrPH, K Ijaz, MD, PD McElroy, PhD, Div of TB Elimination, National Center for HIV, STD, and TB Prevention; AM Andre, MD, EIS Officer, CDC. Editorial Note:This report describes recent nosocomial transmission of M. tuberculosis in a community hospital. The index patient spent 3 weeks hospitalized with unrecognized TB, possibly masked by HIV infection. AIDS patients can have atypical presentations of TB disease resulting in diagnostic delays (6). Because TB was not initially a diagnostic consideration, the patient was not placed immediately in respiratory isolation. Although the incidence of TB continues to decline (7), heightened awareness and vigilance is required by hospital staff to identify and treat persons with suspected TB promptly. Patients with suspected TB should be placed in respiratory isolation until infectious TB is ruled out. When the patient is transported for medical procedures that cannot be performed in the isolation room, the patient should wear a surgical mask. Hospital infection-control programs are encouraged to develop protocols and implement administrative procedures for HIV-infected patients with pulmonary symptoms suggestive of TB. Finally, local TB-control programs can assist hospital infection-control staff in investigating community contacts of persons hospitalized with TB (2). References
Table 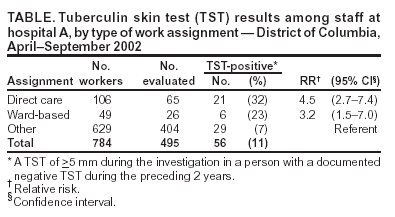 Return to top. Figure 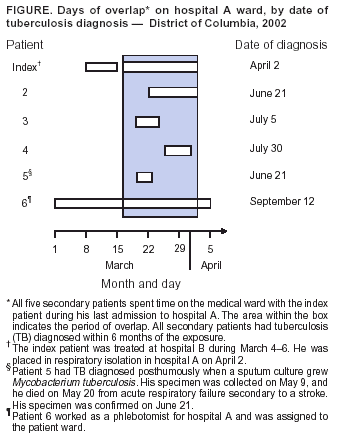 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/18/2004 |
|||||||||
This page last reviewed 3/18/2004
|