|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
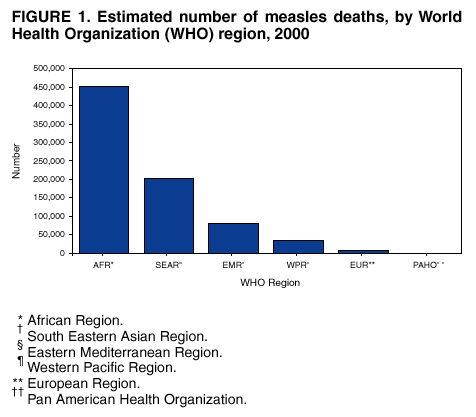
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Update: Global Measles Control and Mortality Reduction --- Worldwide, 1991--2001Despite international recognition of the high burden of disease associated with measles and the existence for 40 years of a safe, effective, and inexpensive vaccine, measles remains the leading cause of vaccine-preventable childhood mortality. In 1990, the World Summit for Children adopted a goal of vaccinating 90% of the world's children against measles by 2000 (1). In 2001, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) developed the Global Measles Strategic Plan for 2001--2005 (2). The plan's objectives are 1) to decrease the annual number of measles deaths by 50% by 2005 compared with 1999 levels (875,000 deaths), 2) to achieve and maintain interruption of indigenous measles transmission in large geographic areas with elimination goals, and 3) to convene a global consultation in 2005 to review progress and assess the feasibility of global measles eradication. In May 2002, the United Nations General Assembly Special Session on Children also resolved to reduce measles deaths by 50% by 2005 compared with 1999 levels (3). This report describes progress toward eliminating measles worldwide. Data from WHO's Global Burden of Disease (GBD) project indicate that approximately 1.7 million vaccine-preventable childhood deaths occurred in 2000, of which 777,000 (46%) were attributed to measles (4). The measles deaths occurred overwhelmingly among children living in poor countries with inadequate vaccination services. To prevent these deaths, stronger political commitment is needed to provide all children worldwide with two opportunities for measles immunization. To estimate cause-specific deaths, GBD first estimates a total number of worldwide childhood deaths based on WHO life table estimates (4). Total deaths are classified into three groups according to a model derived from the WHO mortality database (4). Within the communicable disease category, the contributions of individual causes of death are estimated based on data from multiple sources (e.g., vital registration systems, population laboratories, surveys, and epidemiologic modeling of specific conditions) (4). An alternative approach using a model to estimate measles-associated morbidity and mortality based on country-specific data, including demographic profiles, vaccine coverage, and estimated case-fatality ratios, determined that approximately 805,000 measles-associated deaths occurred globally during 2000, compared with the 777,000 deaths annually estimated through the GBD project (5). Countries report measles vaccination coverage routinely to WHO. Coverage usually is determined by the number of doses of vaccine delivered through routine health services divided by the birth cohort of the previous year. When reports are not received, WHO estimates the most likely coverage based on previous reports from the country or current reports from countries with historically similar vaccination coverage. During 2001, a total of 159 countries representing 90% of the global population reported measles vaccination coverage to WHO; coverage was estimated for the remaining countries. To supplement this information, WHO requests that countries report on an annual basis results from any coverage surveys conducted (6). According to GBD, of the estimated 777,000 worldwide measles deaths in children during 2000, approximately 453,000 (58%) occurred in the WHO African Region, and approximately 202,000 (26%) in the South East Asian Region (4) (Figure 1). Of the global measles deaths, >98% occurred in the 75 countries with per capita gross domestic products of <$1,000 (WHO, unpublished data, 2003). During 1991--2001, estimated worldwide measles vaccination coverage ranged from 69% to 76%. However, worldwide figures mask regional and national disparities. During this period, estimated coverage for the WHO regions of the Americas, Europe, and the Western Pacific was 82%--94%; estimated coverage for the Eastern Mediterranean Region was 67%--73%, and coverage in the South East Asia Region was 50%--72%. The African Region had the lowest estimated coverage, at 51%--60%. Since 2000, WHO and UNICEF have recommended that, in addition to achieving high coverage with the first dose of measles vaccine, all children be offered a second opportunity for measles vaccination to maximize both individual and population immunity (7). This represents a second opportunity for measles immunization for children who did not receive measles vaccine from the routine program and for those who did not develop immunity to measles after receiving measles vaccine. During 1997--2001, a total of 156 (82%) of 191 countries provided a second opportunity through supplementary immunization activities or through routine health services (6) (Figure 2). Reported by: V Dietz, Pan American Health Organization, World Health Organization, Washington, DC. J Spika, European Regional Office; R Kezaala, African Regional Office; E Moshni, Eastern Mediterranean Regional Office; A Thapa, South Eastern Asian Regional Office; J McFarland, Western Pacific Regional Office; M Gacic-Dobo, M Birmingham, J Bilous, B Hersh, Dept of Vaccines and Biologicals, World Health Organization, Geneva, Switzerland. L Cairns, P Strebel, Global Immunization Div, National Immunization Program, CDC. Editorial Note:Although substantial progress has been made in reducing measles deaths globally, in 2000, measles was estimated to be the fifth leading cause of mortality worldwide for children aged <5 years (4). Measles deaths occur disproportionately in Africa and South East Asia. In 2000, the African Region of WHO, with 10% of the world's population, accounted for 41% of estimated measles cases and 58% of measles deaths; the South East Asia region, with 25% of the world's population and 28% of measles cases, accounted for 26% of measles deaths (4). The burden of mortality in Africa reflects low routine vaccination coverage and high case-fatality ratios. In South East Asia, where vaccination coverage is slightly below average worldwide levels, the large population amplifies the number of cases and deaths resulting from ongoing measles transmission. The overwhelming majority of measles deaths in 2000 occurred in countries eligible to receive financial support from the Global Alliance for Vaccines and Immunization's Vaccine Fund (WHO, unpublished data, 2003). The majority of measles deaths occur among young children living in poor countries with inadequate vaccination services. Like human immunodeficiency virus, malaria, and tuberculosis, measles can be considered a disease of poverty. However, unlike these diseases, measles can be prevented through vaccination. Support from the Vaccine Fund for strengthening vaccination services and raising routine vaccination coverage can help reduce the high burden of measles. However, in countries with historically inadequate vaccination services, routine vaccination alone is not sufficient to reduce measles deaths or to achieve measles control because the large numbers of older children who missed routine vaccination remain susceptible to measles. The Measles Mortality Reduction and Regional Elimination Strategic Plan 2001--2005 outlines four main elements to reduce measles mortality: 1) achieving high (i.e., >90%) vaccination coverage nationally and in each district with the first dose of measles vaccine administered through routine health services to children who are aged 9 months or slightly older, 2) offering a second opportunity for measles immunization to all children, 3) establishing effective surveillance for measles, and 4) improving case management (3). Countries are encouraged to review measles epidemiology, develop a 3--5 year plan for measles mortality reduction (8), identify reasons for low routine coverage, strengthen routine vaccination services, improve vaccination safety, and integrate measles vaccination activities with other public health activities as appropriate. Although well-conducted supplemental vaccination activities can increase population immunity substantially and reduce measles cases and deaths, new birth cohorts rapidly add susceptible persons to the population. Bolstering routine vaccination services to ensure that the majority of infants receive measles vaccine and other vaccines is essential to sustain the impact of measles mortality reduction activities. In 2001, the Measles Partnership was formed to reduce measles deaths in Africa. Members of this partnership include WHO, UNICEF, the United Nations Foundation, the American Red Cross, and CDC. During 2001--2002, this partnership contributed $40 million for the vaccination of approximately 60 million children aged 9 months--14 years living in 13 African countries. Preliminary evidence suggests that these campaigns have had a substantial impact in reducing measles deaths (WHO African Regional Office, unpublished data, 2002). Surveillance to assess burden of disease and guide vaccination policy remains critical. Outbreak investigations should be used as an opportunity to learn about the changing epidemiology of measles. These investigations can provide information about patterns of transmission, including case-fatality ratios and age distribution and vaccination status of cases. References
Figure 1
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 5/22/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 5/22/2003