|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
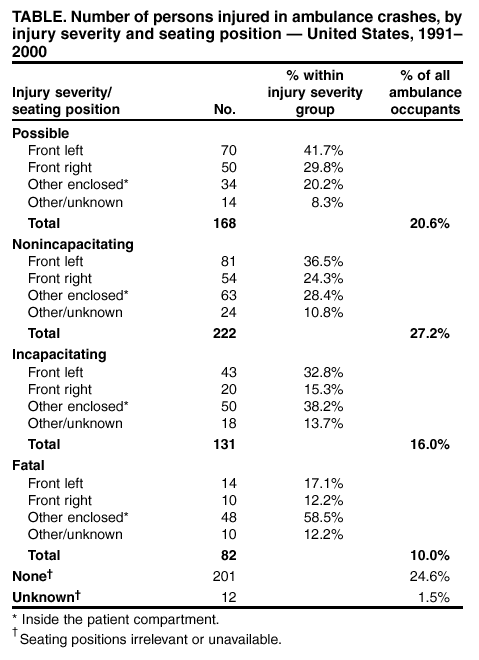
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Ambulance Crash-Related Injuries Among Emergency Medical Services Workers --- United States, 1991--2002Ambulance crashes are one of many hazards faced by Emergency Medical Services (EMS) personnel. Although no complete national count of ground ambulance crashes exists, the total number of fatal crashes involving ambulances can be ascertained by using the National Highway Traffic Safety Administration (NHTSA) Fatality Analysis Reporting System (FARS). To characterize risk factors for EMS workers involved in ambulance crashes, CDC's National Institute for Occupational Safety and Health (NIOSH) and NHTSA investigated three case reports of ambulance crashes. This report summarizes these investigations, presents surveillance data, and discusses recommendations for prevention measures. NIOSH is identifying and testing alternative measures to reduce injury risk for EMS workers. Case ReportsCase 1. In May 2001, an Emergency Medical Technician (EMT) aged 26 years died when her ambulance was struck head-on by a pick-up truck at 6:30 a.m. The EMT had been riding unrestrained in the patient compartment while attending a patient during a nonemergency transport. During the collision, the EMT struck the front bulkhead of the patient compartment; she died en route to the hospital from blunt force trauma to the head and chest. The patient and pick-up driver also suffered fatal injuries. The ambulance driver had been driving unrestrained and suffered multiple serious injuries, including a fractured leg. Case 2. In July 2001, an EMT aged 27 years died when her ambulance struck an elevated train-track support column at 12:30 p.m. She had been riding unrestrained in the patient compartment while attending a patient during a nonemergency transport. During the collision, the EMT and the patient both struck the front bulkhead of the patient compartment. Both the driver and patient were hospitalized; the EMT was transported to a hospital, where she was pronounced dead. Case 3. In March 2002, an EMT aged 22 years who was driving and a paramedic aged 37 years were injured when their ambulance struck an oncoming vehicle head-on and overturned. The paramedic was riding unrestrained on the patient compartment squad bench while attending a patient during a nonemergency transport. A relative of the patient was seated in the rear-facing attendant's seat and was wearing a seatbelt. During the collision, the unrestrained EMT driver sustained minor injuries. The paramedic struck the interior cabinets and shelves of the patient compartment. The EMT and the paramedic were transported to a hospital, where the EMT was treated and released; the paramedic was hospitalized and released 2 days later. The patient's injuries included scalp and shoulder contusions and a shoulder laceration. The patient's relative sustained minor internal injuries. Surveillance DataDuring 1991--2000, the most recent year for which data were available, 300 fatal crashes occurred involving occupied ambulances, resulting in the deaths of 82 ambulance occupants and 275 occupants of other vehicles and pedestrians. The 300 crashes involved a total of 816 ambulance occupants. FARS does not differentiate ambulance workers from passengers among those experiencing nonfatal injuries in fatal crashes; however, the seating positions for all occupants and the severity of injuries can be determined from FARS data (Table). Although which occupants were EMS workers and which were patients or other passengers cannot be ascertained precisely, calculations using the FARS "fatal injury at work" variable based on death certificate information indicate that 27 of the occupants killed were on-duty EMS workers. These comprised 3% of all ambulance occupants and 33% of occupant fatalities. The majority of the 27 EMS worker fatalities occurred in the front of the vehicle: 11 (41%) in the driver's seat and five (19%) in the front right-side seat.* Those coded as "other enclosed" accounted for seven (26%) of the EMS worker fatalities; these persons probably were working in the patient compartment. Four EMS workers were listed in "other/unknown" seating positions (Table). Reported by: SL Proudfoot, NT Romano, MS, TG Bobick, PhD, PH Moore, Div of Safety Research, National Institute for Occupational Safety and Health, CDC. Editorial Note:EMS personnel in the United States have an estimated fatality rate of 12.7 per 100,000 workers, more than twice the national average (1). This report documents 27 ambulance crash-related fatalities among EMS workers over a 10-year period. The surveillance data and case investigations identify riding unrestrained as an important risk factor for EMS workers. Among all ambulance occupants, riding in the patient compartment was associated with greater injury severity. However, in 27 incidents coded as "fatal injury at work," seven (26%) of the EMS workers killed were drivers who were not wearing a restraint, and two (7.4%) were unrestrained in the front right seat. Six (22%) of the EMS workers killed were not wearing restraints while riding in the patient compartment. In 1966, the National Academy of Sciences cited deficiencies at various levels of emergency care, including unsuitable ambulances with inadequate equipment, incomplete supplies, untrained attendees, lack of traffic control, and lack of voice communication facilities (2). Since 1966, substantial improvements have been made in communications systems, the routine use of modern lifesaving equipment, and the level of worker expertise. In addition, the amount of emergency care has increased in volume, in level of complexity, and in required competency of EMS workers (3). However, in January 1992, minimal workplace safety research was conducted for EMS personnel, and statistics related to worker characteristics and job duties were largely unavailable (4). According to a retrospective study investigating characteristics of fatal ambulance crashes during an 11-year period that emphasized emergency versus nonemergency use incidents, the majority of ambulance crashes occurred during emergency use, and rear compartment occupants were more likely to be injured than those in front (5). Less than half of EMS workers use restraints in the patient compartment (6). In addition, lap-belt restraint systems commonly provided in patient compartments do not allow full access to the patient. When properly used, the squad bench lap belts position the EMS worker against the side wall, making it impossible for the worker to bend forward to access the patient. If the EMS worker needs to access the cabinets along the driver-side wall, the belts must be unbuckled to allow the worker to stand up. If CPR or other procedures such as intubation or insertion of IVs must be performed, EMS personnel might need to stand over or kneel near the cot. For these reasons, EMS workers often ride unrestrained, seated on the edge of the squad bench (7). In addition, unrestrained or improperly restrained patients who become airborne in a crash might pose an additional injury risk to EMS personnel and to themselves. The findings in this report are subject to at least three limitations. First, FARS records only crashes involving a motor vehicle traveling on a traffic-way customarily open to the public that result in the death of a person (either a vehicle occupant or nonmotorist) within 30 days of the crash (8). As a result, fatal crashes on private property (e.g., driveways, parking lots, or private roads) are excluded. Second, which ambulance occupants were EMS workers cannot be determined precisely by examining injuries by occupation code. EMS might be provided by local career or volunteer fire departments, private ambulance companies, or volunteer rescue services. Finally, data about nonfatal injuries to volunteer firefighters and EMS workers are not included routinely in occupational injury databases. CDC recommends that EMS employers ensure that EMS workers use patient compartment vehicle occupant restraints whenever possible, ensure that drivers and front-seat passengers of EMS vehicles use the occupant restraints provided, consider equipping ambulances with patient cots that include upper body restraints, and ensure that EMS workers who operate ambulances are qualified and trained appropriately. Ambulance manufacturers should evaluate and develop occupant protection systems designed to increase the crash survivability of EMS workers and patients in ambulance patient compartments and ensure that such systems allow EMS workers mobility to access patients and equipment. References
* A total of 14 fatalities occurred among driver's seat occupants; two of them were coded "unknown" for "fatal injury at work," and a third was coded "no." Although an ambulance driver might be an EMS worker, only those coded positively for "fatal injury at work" were included as EMS workers.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/27/2003 |
|||||||||
This page last reviewed 2/27/2003
|