|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
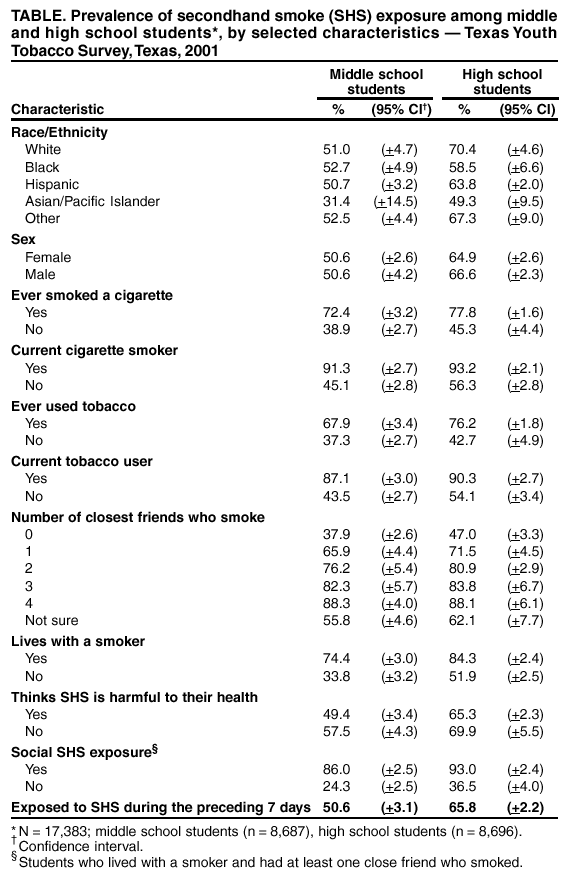
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Secondhand Smoke Exposure Among Middle and High School Students --- Texas, 2001Secondhand smoke (SHS) exposure causes approximately 3,000 deaths each year in Texas (1,2) and is associated with increased morbidity caused by acute respiratory infections and asthma among children and respiratory problems among adults (3,4). Adult lung cancer risk might be increased as a result of SHS exposure during childhood and adolescence (5). To assess SHS exposure among middle and high school students in Texas, the Texas Department of Health (TDH) analyzed data from the 2001 Texas Youth Tobacco Survey (TYTS). This report summarizes the results of that analysis, which indicate that half of 8,687 middle school students and two-thirds of 8,696 high school students reported SHS exposure within the 7 days preceding the survey. The prevalence of SHS exposure was higher among students who reported living with a cigarette smoker or having at least one close friend who smokes. Among middle school students, the prevalence of SHS exposure was lower among those who perceived SHS to be harmful to their health. These findings emphasize the need for continuing efforts to decrease SHS exposure among youth and to increase understanding of the harmful health effects of SHS exposure. During fall 2001, TDH conducted the third TYTS. The survey uses a two-stage cluster sample design to produce representative samples of middle and high school students in Texas public schools. The primary sampling units were public schools with students in grades 6--12. Schools were stratified into middle schools (grades 6--8) and high schools (grades 9--12), and two separate samples were drawn. Schools were selected for participation in the survey with a probability proportional to the number of students enrolled. The secondary sampling units were classes selected randomly within schools that agreed to participate. All students in the selected classes, regardless of tobacco-use status, were eligible to participate in the survey. Students completed an anonymous, self-administered questionnaire that included questions on demographics, tobacco use, tobacco-related knowledge and attitudes, media messages about tobacco use, access to tobacco, tobacco-related school curriculum, SHS, and tobacco-use cessation. Data were weighted to adjust for nonresponse at both the student and school level and to provide generalizable estimates for Texas public school students according to grade, sex, and race/ethnicity. To assess SHS exposure, TYTS asked students to report how many days they had been in the same room or riding in a car with someone who was smoking cigarettes during the 7 days preceding the survey. SHS exposure was compared among middle and high school students by demographics, tobacco use, presence of close contacts who smoke, and attitudes toward SHS. SUDAAN (version 8.0) was used to calculate prevalence estimates and standard errors for 95% confidence intervals (CIs). A total of 17,383 students from 192 schools participated in the 2001 TYTS. The overall response rate, a product of the school and individual student response rates, was 64.5%. The response rates were 71.3% for middle schools and 60.3% for high schools. During 2001, the prevalence of SHS exposure increased with grade: 50.6% (95% CI = +3.1%) of middle school students reported SHS exposure compared with 65.8% (95% CI = +2.2%) of high school students. Asians/Pacific Islanders (42.0%; 95% CI = +9.0%) were less likely than other racial/ethnic groups to report SHS exposure. The prevalence of SHS exposure did not differ significantly among blacks (56.0%; 95% CI = +4.3%), Hispanics (58.1%; 95% CI = +1.8%), whites (62.0%; 95% CI = +3.8%), or other racial/ethnic groups (60.5%; 95% CI = +5.2%). Overall, 73.5% (95% CI = +1.7%) of students who had ever used any tobacco product reported SHS exposure, compared with 39.5% (95% CI = +2.5%) of students who never used any tobacco product. Among students who lived with a cigarette smoker, 80.1% (95% CI = +2.2%) reported SHS exposure compared with 43.9% (95% CI = +1.9%) of students who did not live with a cigarette smoker. Among students with no close friends who smoke, 42.0% (95% CI = +2.0%) reported SHS exposure compared with 79.0% (95% CI = +1.6%) of students with at least one close friend who smokes. The prevalence of SHS exposure was 29.7% (95% CI = +1.1%) among students with no social sources of SHS exposure (i.e., those who did not live with a smoker or did not have any close friends who smoke), compared with 90.7% (95% CI = +2.1%) who lived with a smoker and had at least one close friend who smokes. Students' perception of SHS exposure being harmful to their health varied slightly. Overall, the prevalence of SHS exposure was 58.5% (95% CI = +1.9%) among students who perceived SHS to be harmful to their health, compared with 63.6% (95% CI = +3.7%) of students who did not think SHS was harmful. Among middle school students, those who perceived SHS to be harmful to their health were statistically less likely to report SHS exposure than students who did not think SHS was harmful (Table). Among high school students, perceptions of the health risks for SHS exposure did not affect personal SHS exposure. Reported by: C Alo, P Huang, Texas Dept of Health. ME McCusker, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that, despite its known health hazards, SHS exposure among Texas students is common. Perceptions of the health hazards of SHS exposure were associated with less reported exposure among middle school students. Among students who reported living with a smoker and having at least one close friend who smokes, the prevalence of SHS exposure was three-fold that of students who did not have these social SHS exposures. Even among students without any social sources of SHS exposure, approximately one third reported that they were exposed to SHS. These findings suggest that reducing youth exposure to SHS requires strategies such as policies that limit SHS exposure and interventions to decrease youth tobacco-use initiation and to promote tobacco-use cessation among youth and adults. Serum cotinine levels, a measure of SHS exposure, are higher among youth than among adults in the United States (6), which underscore the need to reduce SHS exposure, especially among youth. Several communities in Texas have passed ordinances that restrict indoor smoking, including a total ban on indoor smoking in all public places in El Paso and a recent ordinance in Dallas that bans indoor smoking in all public places except freestanding bars. In addition, the Environmental Protection Agency has developed the Smoke-Free Home Pledge Initiative, a campaign to reduce SHS exposure among children in their homes (http://www.epa.gov/smokefree/index.html). These initiatives might help reduce SHS exposure both in the community and at home. The findings in this report are subject to at least three limitations. First, the data are representative only of Texas students who attend public schools and might not apply to students who have dropped out of school or who are enrolled in private schools. During the 1999--00 school year, the average dropout rate for Texas public school students enrolled in grades 7--12 was 1.3% (7). In addition, approximately 10% of middle and high school students are enrolled in private schools (8). Second, because TYTS data are self-reported and anonymous, the validity of the responses is difficult to assess. Studies attempting to validate self-reported smoking among youth suggest that the sensitivity of self-reported data on tobacco use is approximately 81% (9). Finally, TYTS asked only if students had been in the same room or car with someone who was smoking during the preceding 7 days. Details about how youths are exposed to SHS, including where the exposure occurs and whether youths are exposed more commonly to SHS from household members, parents, or friends, would help in targeting tobacco-control programs designed to reduce SHS exposure. Effective strategies to reduce SHS exposure include 1) community policies such as smoking bans and restrictions that limit SHS exposure, 2) interventions to decrease youth tobacco-use initiation, and 3) interventions to promote tobacco-use cessation among youth and adults (10). The data presented in this report underscore the need for increased efforts to implement these strategies to reduce SHS exposure among youths and prevent the negative health effects of SHS exposure. References
Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 2/27/2003 |
|||||||||
This page last reviewed 2/27/2003
|